Define.
What would you like me to define? Please share the word, term, or concept you have in mind.
Define difference between cancerous and non-cancerous lumps in breast. Location of nipple and extent of breast. Lymphatic drainage of each quadrant of breast. According to MS1 level
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a complete MS1-level answer. Let me compile it.
Breast - MS1 Complete Notes
1. Location of the Nipple and Extent of the Breast
Extent (Boundaries)
The breast (mammary gland + overlying skin + superficial fascia) lies in the pectoral region of the anterior thoracic wall.
| Direction | Boundary |
|---|---|
| Vertical | Rib II (superiorly) to Rib VI (inferiorly) |
| Horizontal | Lateral border of sternum --> Midaxillary line |
| Depth | Lies on deep fascia of pectoralis major; separated from it by the retromammary space (loose connective tissue allowing mobility) |
An axillary tail (tail of Spence) extends superolaterally through an opening in the deep fascia into the axilla - this is clinically relevant because it can be mistaken for an axillary lump.
Position of the Nipple
- The nipple lies at approximately the 4th intercostal space (mid-clavicular line) in the non-pendulous breast
- It is innervated by the 4th intercostal nerve (T4 dermatome)
- Surrounded by the pigmented areola
- The nipple receives the openings of 15-20 lactiferous ducts
Gray's Anatomy for Students: "The nipple is surrounded by a circular pigmented area of skin termed the areola... innervation of the nipple is by the fourth intercostal nerve."
2. Cancerous vs. Non-Cancerous Breast Lumps
This is one of the most tested clinical comparisons at MS1 level. The features can be remembered using the mnemonic SITS (Surface, Invasiveness, Tenderness, Shape).
| Feature | Benign (Non-Cancerous) | Malignant (Cancerous) |
|---|---|---|
| Shape | Round, oval, well-defined | Irregular, ill-defined |
| Borders | Smooth, circumscribed | Spiculated, irregular |
| Consistency | Soft/rubbery (fibroadenoma) or tense (cyst) | Hard, stony |
| Mobility | Freely mobile ("breast mouse") | Fixed to skin or chest wall |
| Skin changes | None | Peau d'orange (skin dimpling), nipple retraction, skin tethering |
| Tenderness | Often tender (cysts, fibrocystic) | Usually non-tender (painless mass) |
| Nipple discharge | May occur; bilateral, non-bloody | Unilateral, spontaneous, bloody = malignant until proved otherwise |
| Borders on imaging | Circumscribed on mammogram/US | Spiculated/irregular density, microcalcifications |
| Lymph nodes | Not involved | Hard, fixed axillary nodes = metastasis |
| Age | Fibroadenoma: 15-35 years | Carcinoma: >40 years; risk increases with age |
Robbins Basic Pathology: "Most (~95%) [palpable masses] are benign and tend to be round to oval with circumscribed borders. By contrast, malignant tumors usually invade across tissue planes and have irregular borders. However, because some cancers mimic benign lesions by growing as circumscribed masses, all palpable masses require evaluation."
Common Benign Lumps
| Type | Key Features |
|---|---|
| Fibroadenoma | Most common in young women (15-35 yrs); firm, rubbery, very mobile, non-tender; "breast mouse" |
| Breast cyst | Fluctuant, tense, smooth; may be tender; disappears on aspiration |
| Fibrocystic change | Diffuse nodularity; bilateral; worse premenstrually |
| Fat necrosis | History of trauma; may mimic cancer; can cause skin tethering |
| Fibroadenoma (phyllodes) | Large, rapidly growing; rarely malignant; leaf-like pattern on histology |
Skin Signs of Malignancy - Mechanism
- Peau d'orange (orange peel skin): Cancer invades dermal lymphatics causing lymphedema of the skin; hair follicles create dimples
- Skin dimpling/tethering: Carcinoma invades and contracts the suspensory ligaments of Cooper, pulling the skin inward
- Nipple retraction: Cancer invades the lactiferous ducts, causing fibrosis and inward retraction of the nipple
Gray's Anatomy for Students: "Carcinoma of the breast creates tension on these [suspensory] ligaments, causing pitting of the skin."
Distribution of Malignant Tumors by Quadrant
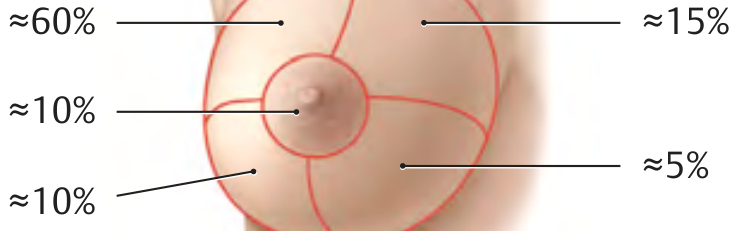
| Quadrant | Approximate % of breast cancers |
|---|---|
| Upper outer quadrant (UOQ) | ~60% (most common - largest amount of glandular tissue) |
| Upper inner quadrant | ~15% |
| Lower outer quadrant | ~10% |
| Lower inner quadrant | ~5% |
| Central (subareolar) | ~10% |
3. Lymphatic Drainage of the Breast - By Quadrant
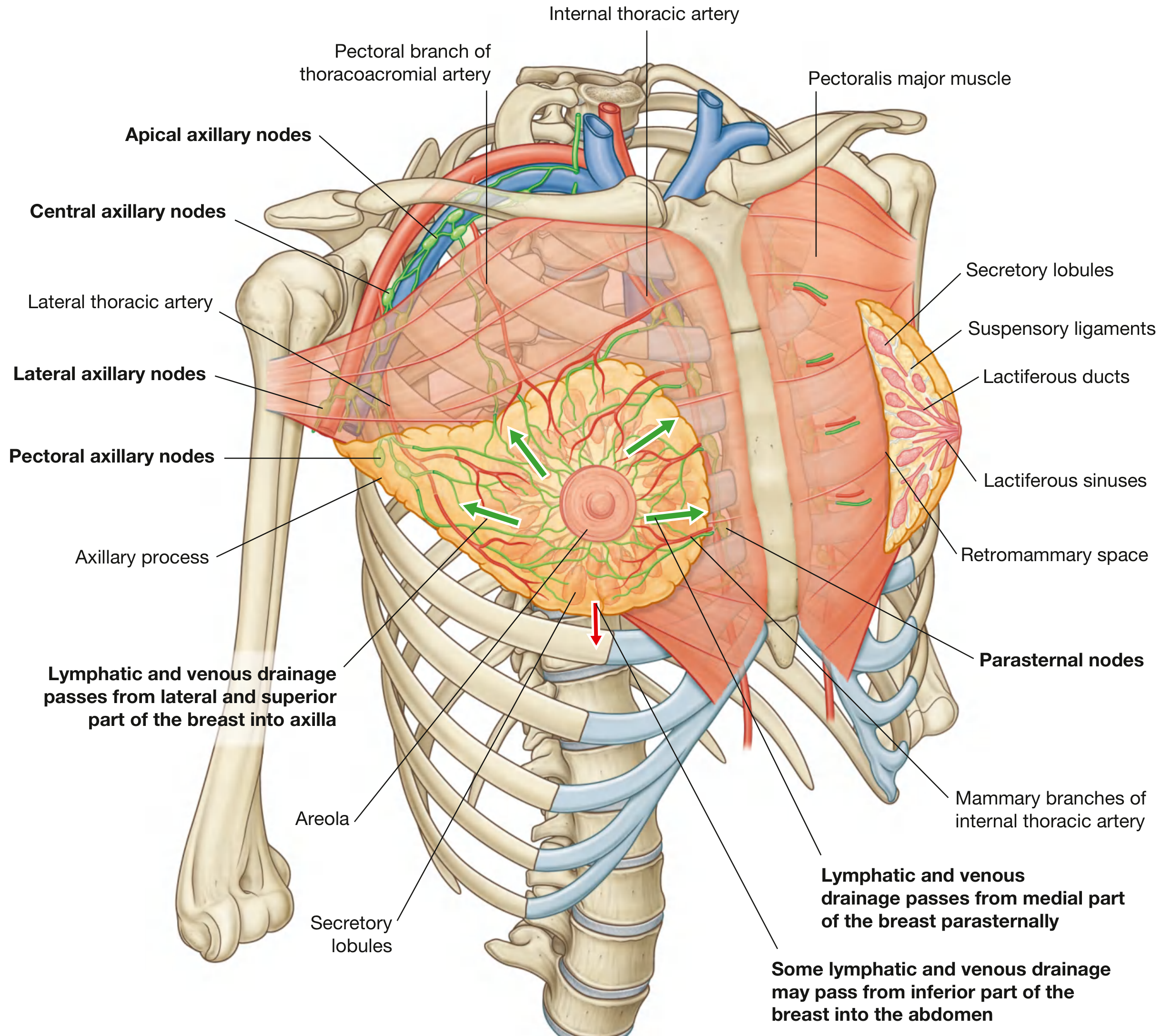
General Principle
All lymph from the breast first drains into the subareolar lymphatic plexus of Sappey (beneath the areola). From there, it spreads to regional nodes.
By Quadrant
| Quadrant | Primary Lymph Nodes | Secondary Nodes |
|---|---|---|
| Upper outer (UOQ) | Anterior/Pectoral axillary nodes (Level I) --> Central nodes (Level II) --> Apical nodes (Level III) | Deltopectoral nodes |
| Upper inner (UIQ) | Parasternal (internal mammary) nodes | Apical axillary, contralateral breast |
| Lower outer (LOQ) | Anterior/Pectoral axillary nodes | Central, apical |
| Lower inner (LIQ) | Parasternal (internal mammary) nodes | Subperitoneal plexus --> liver, pelvis |
| Central/Nipple | Subareolar plexus --> Axillary (mainly pectoral group, ~75%) | Parasternal, supraclavicular |
S Das Manual on Clinical Surgery: "Lymphatic drainage from the subareolar plexus of Sappey and outer quadrant of the breast takes place first to the pectoral (P), then central (C) and lastly to the apical (A) group of axillary lymph nodes. The upper quadrant of the breast drains partly to the delto-pectoral node but mainly to the apical group. From the inner quadrant the lymph spread occurs to the internal mammary group and to the other breast. From the lower and inner parts of the breast, the lymph vessels form a plexus over the rectus sheath and pierce the costal margin to communicate with the subperitoneal lymph plexus."
Axillary Node Levels (Surgically Important)
| Level | Location | Groups |
|---|---|---|
| Level I | Lateral to pectoralis minor | Pectoral, subscapular, lateral axillary nodes |
| Level II | Behind pectoralis minor | Central axillary, interpectoral (Rotter's) nodes |
| Level III | Medial to pectoralis minor | Apical axillary nodes |
- Lymph flows sequentially: Level I --> Level II --> Level III --> Subclavian trunk --> Thoracic duct (left) or Right lymphatic duct
- Parasternal nodes drain via bronchomediastinal trunk
Clinical Significance (Oncology)
- 75% of all breast lymph drains to axillary nodes - the most common site of early metastasis
- The remaining ~25% drains to parasternal nodes - mainly from the medial quadrants
- Sentinel lymph node = first node to receive lymph from the primary tumor; detected by technetium-99m sulfur microcolloid scintigraphy
- 5-year survival with axillary metastasis: Level I = ~65%, Level II = ~31%, Level III approaches 0%
- From the lower inner quadrant, cancer can track via the subperitoneal plexus to the pelvis/ovary, causing a Krukenberg tumor
THIEME Atlas of Anatomy: "The approximately 30 to 60 axillary lymph nodes receiving most of the lymphatic drainage are the first nodes to be affected by metastasis and therefore have major oncological significance."
Sources: Gray's Anatomy for Students (4th ed.) | Robbins & Kumar Basic Pathology | S Das Manual on Clinical Surgery (13th ed.) | THIEME General Anatomy Atlas | Fischer's Mastery of Surgery (8th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.