Osteomyelitis from basics to clinical
Reading File
Finding Sources
Searching PubMed
"osteomyelitis"[MeSH Terms] AND "diagnosis OR treatment"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
I have all the content I need. Now I'll compose the comprehensive answer.
Osteomyelitis: From Basics to Clinical
1. Definition
Osteomyelitis is inflammation of bone and bone marrow, virtually always secondary to infection. It may arise as a complication of systemic bacteremia or manifest as a primary solitary focus of infection in bone. - Robbins & Kumar Pathologic Basis of Disease, p. 1092
2. Classification
By Duration
| Type | Duration | Key Features |
|---|---|---|
| Acute | Days to weeks | Fever, pain, neutrophilic exudate, bacteremia possible |
| Subacute | Weeks to months | Brodie abscess; less systemic toxicity |
| Chronic | Months to years | Sequestrum, involucrum, sinus tracts, periodic flares |
By Route of Infection
- Hematogenous - most common in children; bacteremia seeds the metaphysis
- Contiguous spread - from adjacent soft tissue infection, septic arthritis, or pressure ulcer
- Direct inoculation - open fractures, surgery, puncture wounds, prosthetic implants
By Host/Anatomy: Cierny-Mader Classification (chronic osteomyelitis)
- Stage 1 (Medullary) - infection limited to the endosteum
- Stage 2 (Superficial) - cortical surface involvement only
- Stage 3 (Localized) - full-thickness cortical sequestrum, stable bone
- Stage 4 (Diffuse) - through-and-through instability; most complex
Combined with host class: A (normal), B (compromised locally, systemically, or both), C (treatment worse than disease)
3. Pathogenesis & Microbiology
How Hematogenous Infection Starts
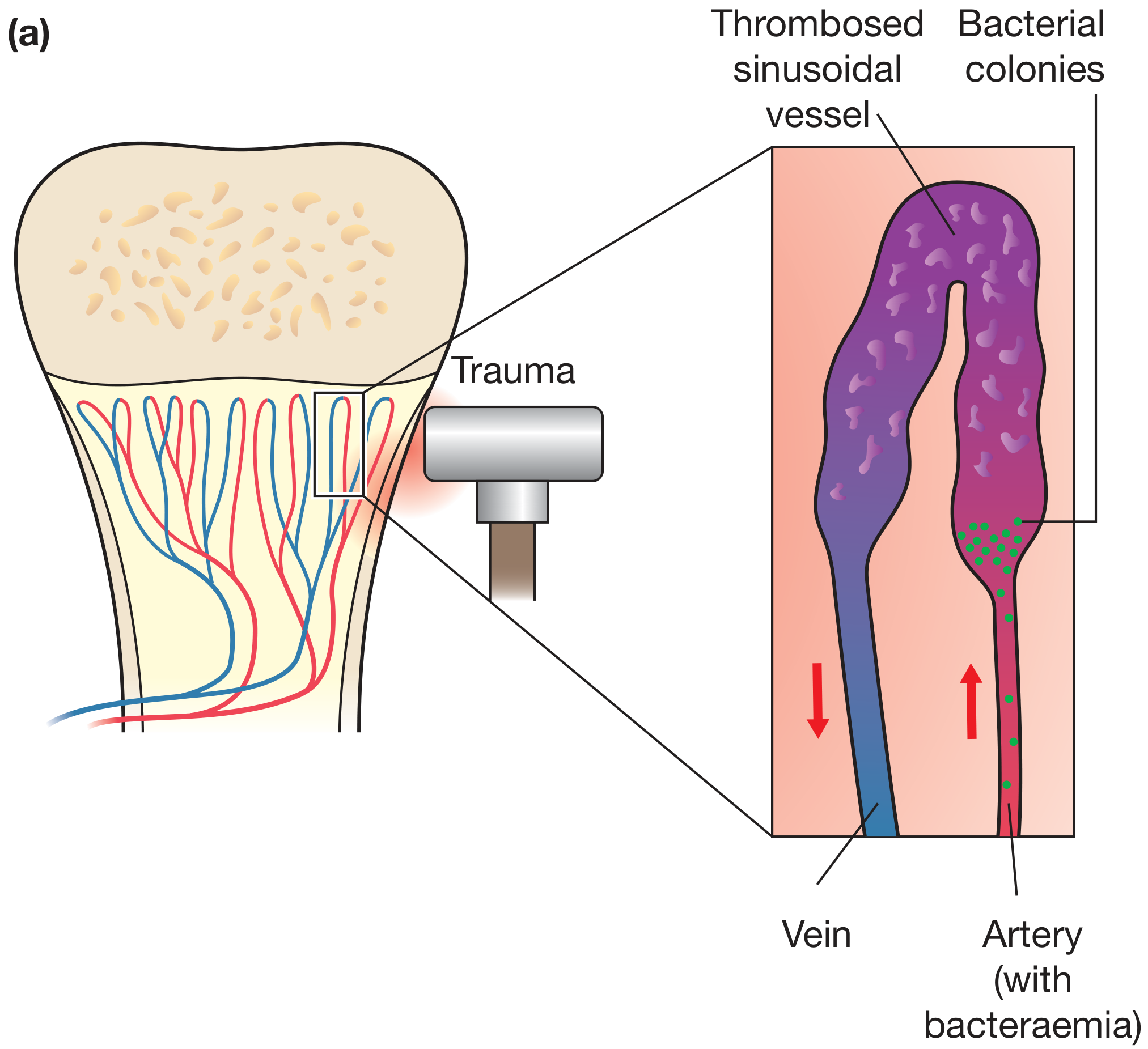
The metaphysis of long bones is particularly vulnerable because:
- Blood flow is sluggish in the looped sinusoidal vessels
- Phagocytic activity is reduced in this region
- Microtrauma (common in active children) disrupts the vascular endothelium
S. aureus binds actively to bone matrix components such as collagen via cell wall proteins (fibronectin-binding proteins, MSCRAMM family), which facilitates and explains its dominance as the causative pathogen. - Robbins Pathologic Basis, p. 1092
Pathogens by Clinical Context
| Setting | Common Organisms |
|---|---|
| Children (all ages) | S. aureus (80-90%), MRSA increasingly common |
| Neonates | Group B Streptococcus, E. coli, S. aureus |
| Adults (hematogenous) | S. aureus, gram-negative bacilli |
| Sickle cell disease | Salmonella spp., S. aureus |
| IV drug users | S. aureus, Pseudomonas aeruginosa, Candida spp. |
| Diabetic foot / contiguous | Polymicrobial (gram-positive + gram-negative + anaerobes) |
| Postoperative / prosthetic | S. aureus, coagulase-negative Staphylococci |
| Open fractures | Polymicrobial, Pseudomonas, Acinetobacter |
| Spinal (vertebral) | S. aureus, gram-negative bacilli |
| Immunocompromised | Fungi (Candida, Aspergillus, Coccidioides), mycobacteria |
4. Pathology: Stages and Key Terms
Acute Phase (first 48 hours onward)
- Bacteria proliferate → neutrophilic infiltration
- Bone cell necrosis and marrow necrosis occur within 48 hours
- Bacteria spread through Haversian canals → reach the periosteum
- In children: periosteum loosely attached → subperiosteal abscess forms
- Periosteal lifting → impaired cortical blood supply → more necrosis
- Soft tissue abscess → may rupture to skin as draining sinus
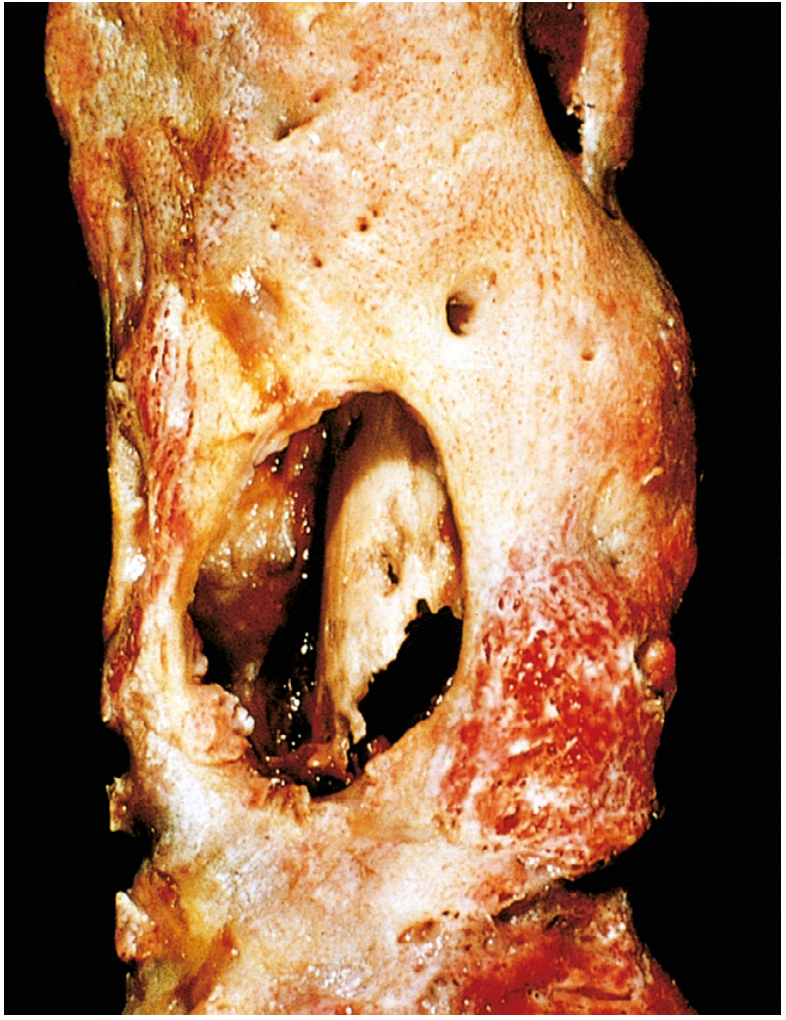
Subacute - Chronic Transition
- Chronic inflammatory cells (lymphocytes, plasma cells) recruited
- Cytokines stimulate bone resorption and fibrous tissue ingrowth
- Dead avascular bone fragment = sequestrum
- Reactive periosteal new bone that encases the sequestrum = involucrum
- This creates the classic "bone-within-a-bone" radiographic appearance
- Gaps in the involucrum (called cloacae) allow pus to track to skin
- Subacute variant: Brodie abscess - a well-defined lytic cavity with a sclerotic rim; represents a contained focus of subacute infection
5. Age-Related Anatomical Differences
The location of infection is dictated by the vascular anatomy of bone, which changes with age:
| Age | Vascular Anatomy | Typical Site |
|---|---|---|
| Neonate (<1 yr) | Metaphyseal vessels penetrate the growth plate | Metaphysis AND epiphysis; joint involvement common |
| Child (1-16 yr) | Terminal metaphyseal vessels loop back; growth plate acts as barrier | Metaphysis predominantly |
| Adult | Growth plate closure creates metaphyseal-epiphyseal anastomoses | Epiphysis, subchondral regions, vertebral bodies |
In neonates, this anatomy means proximal femoral osteomyelitis and septic arthritis are essentially the same condition - the infection readily crosses the growth plate. - Bailey & Love, p. 657
6. Clinical Features
Acute Osteomyelitis
- Fever, rigors, malaise - systemic sepsis signs
- Point tenderness over the infected bone segment (the single most reliable physical finding)
- Localized warmth, swelling, erythema - variable
- Limb guarding / refusal to bear weight - especially in children
- Sympathetic joint effusion - adjacent joint may have sterile effusion even without septic arthritis
Chronic Osteomyelitis
- Systemic signs may be absent or minimal
- Palpable involucrum or sequestrum may be felt
- Draining sinus tracts to skin
- Periodic acute flares after years of dormancy
- Chronic pain and functional limitation
Special Presentations
Vertebral Osteomyelitis (Spondylodiscitis)
- Lumbar and cervical vertebrae most common in adults
- Back pain + fever (fever often absent in elderly/immunocompromised)
- Paravertebral or epidural abscess in many cases
- Red flags requiring emergency evaluation: radicular pain, sensory loss, lower extremity weakness, urinary retention, bowel/bladder incontinence (signs of cord compression) - Goldman-Cecil Medicine, p. 3146
- MRI is the modality of choice for showing intraspinal complications
Diabetic Foot Osteomyelitis
- Extension from contiguous soft tissue infection (ulcer → fascia → bone)
- Insidious; foot may be neuropathic with minimal pain
- "Probe-to-bone" test: if a sterile probe through an ulcer reaches bone, osteomyelitis is highly likely (PPV ~89%)
- Polymicrobial
Osteomyelitis in Sickle Cell Disease
- Areas of bone infarction from vaso-occlusion serve as nidus
- Loss of splenic function impairs antibody-mediated immunity
- Salmonella is classically the pathogen; however S. aureus remains common
7. Investigations
Laboratory
| Test | Comment |
|---|---|
| WBC | Elevated in acute; may be normal in chronic |
| ESR | Elevated in >90% of hematogenous cases; follows treatment response |
| CRP | More sensitive; rises and falls faster than ESR; useful monitoring tool |
| Blood cultures | Positive in ~40% of children with AHO; positive in ~50% of adults with vertebral osteomyelitis |
| Bone biopsy & culture | Gold standard for pathogen identification; positive in ~50% of cases; PCR-based assays improving yield |
| Procalcitonin | Less sensitive than CRP but elevated in bacteremic osteomyelitis |
Microbiological cultures identify a specific organism in only approximately 50% of patients. PCR assays identifying microbe-specific DNA sequences are increasingly used. - Robbins Pathologic Basis, p. 1092
Imaging
Plain Radiograph (X-ray)
- First-line, readily available
- Changes lag 10-21 days behind clinical onset - initial X-ray often normal
- Early signs: soft tissue swelling, periosteal reaction
- Late signs: lytic destruction, cortical irregularity, sclerosis, periosteal new bone, sequestrum
- Radiolucency requires 30-50% bone mineral loss to be visible
Ultrasound
- Useful in infants and children (simple, no radiation)
- Detects subperiosteal fluid/abscess, periosteal lifting, soft tissue edema
- Guides aspiration/drainage procedures
CT
- Superior for defining cortical destruction and sequestrum
- Guides biopsy/aspiration (especially vertebral)
- Limited soft tissue contrast compared to MRI
MRI (modality of choice)
- Highest sensitivity and specificity for early osteomyelitis
- T1: decreased signal in infected marrow (fat replacement by edema/pus)
- T2 / STIR: increased signal in infected marrow and adjacent soft tissue
- Gadolinium contrast: highlights abscess walls, reveals devascularized bone
- Penumbra sign in subacute osteomyelitis (Brodie abscess): peripheral high-signal ring (granulation tissue) surrounding low-signal central cavity on T1
- Whole-body MRI or skeletal scintigraphy useful in neonates with possible multifocal disease
Bone Scintigraphy (Tc-99m MDP three-phase scan)
- Sensitive but not specific; positive early (before X-ray changes)
- Useful when MRI is unavailable or for whole-body survey
- False-negative in neonates (poor periosteal reaction)
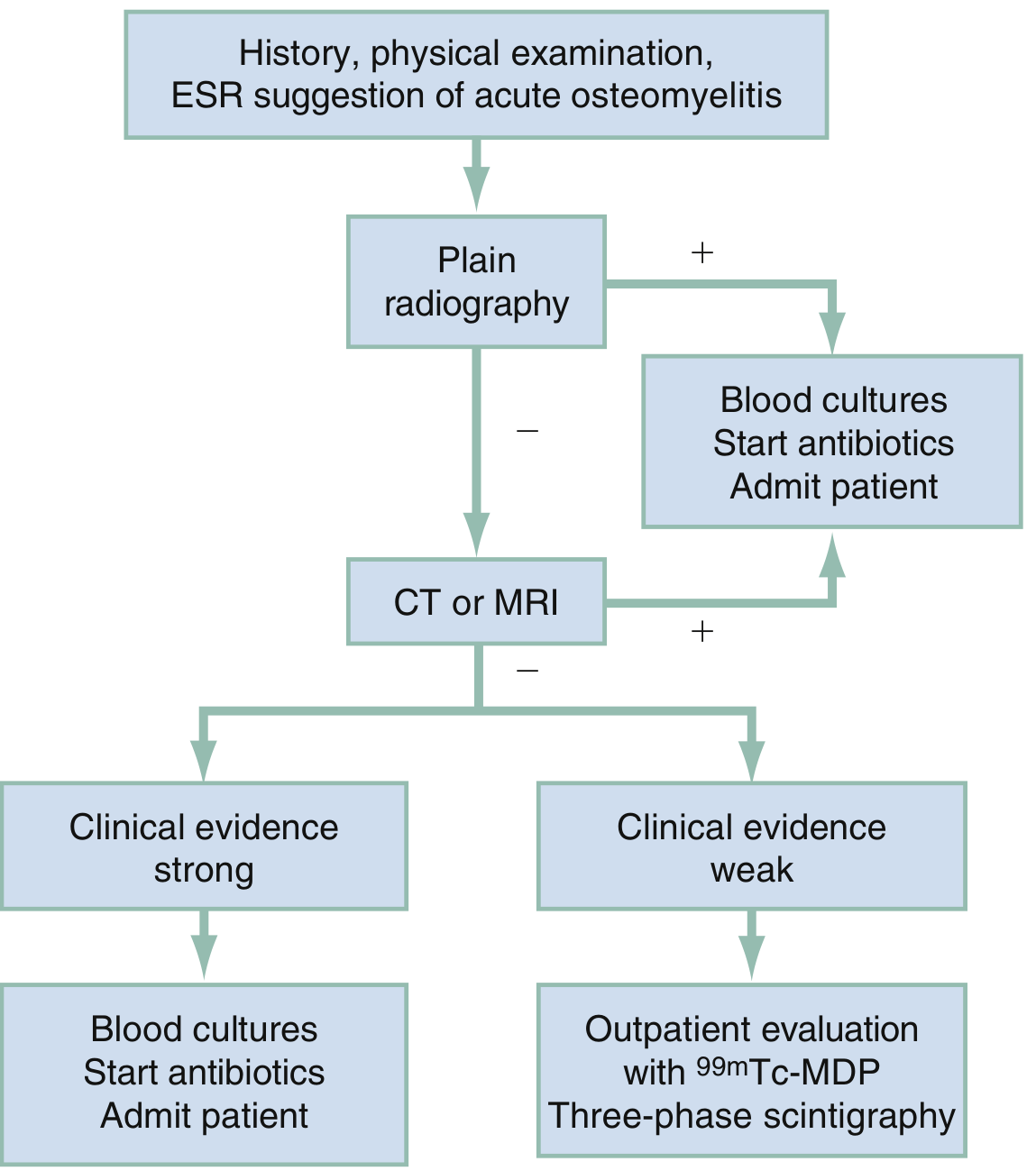
Diagnostic Algorithm
8. Management
General Principles
- Identify the organism before starting antibiotics whenever possible (culture blood, aspirate, biopsy)
- Drain pus when present
- Appropriate and often prolonged antibiotic therapy: parenteral then oral
- Rest and splintage of the affected limb
- Treat the underlying condition (diabetes, sickle cell disease, malnutrition, immunodeficiency)
Antibiotic Therapy
Empirical regimens (before culture results)
| Clinical Setting | Empirical Coverage |
|---|---|
| Child, community, no MRSA risk | Anti-staphylococcal beta-lactam (nafcillin, oxacillin, or flucloxacillin) |
| Child or adult, MRSA risk or community-acquired | Vancomycin (target trough 15-20 mg/L or AUC-guided) |
| Neonatal | Vancomycin + cephalosporin (cover GBS, E. coli, S. aureus) |
| Diabetic foot / polymicrobial | Broad-spectrum: vancomycin + beta-lactam/beta-lactamase inhibitor or carbapenem |
| Sickle cell | Cover both Salmonella (fluoroquinolone or 3rd-gen cephalosporin) and S. aureus |
| IV drug user | Vancomycin + gram-negative coverage (consider MRSA + Pseudomonas) |
Duration of therapy
- Acute uncomplicated (children): historically 4-6 weeks IV; evidence now supports early switch to oral after clinical/CRP improvement (after ~3-5 days IV if responding)
- Adults, hematogenous: 6 weeks total (IV + oral step-down)
- Vertebral osteomyelitis: 6-8 weeks minimum
- Chronic osteomyelitis / prosthetic: often months, especially with biofilm organisms; requires surgery
- MRSA osteomyelitis: vancomycin or daptomycin; consider rifampicin combination in biofilm-associated disease
Note on MRSA: The Panton-Valentine leukocidin (PVL)-positive S. aureus strains significantly increase morbidity. Community-acquired MRSA (CA-MRSA) is now the most common organism in acute hematogenous osteomyelitis in children in many regions. - Bailey & Love, p. 657
Surgical Management
Indications for surgery:
- Failure to respond to antibiotics within 24-48 hours (especially in children)
- Abscess (subperiosteal or soft tissue) requiring drainage
- Chronic osteomyelitis with sequestrum, sinus tract, or Brodie abscess
- Infected hardware or prosthetic joint
- Vertebral osteomyelitis with spinal instability or cord compression
Surgical principles in chronic osteomyelitis (Cierny-Mader approach):
- Radical debridement - remove all sequestrum, infected/necrotic tissue, scar, and biofilm
- Dead space management - fill the cavity left by debridement:
- Antibiotic-impregnated PMMA beads (gentamicin or tobramycin)
- Muscle flap coverage (rotational or free flap)
- Cancellous bone graft (after infection controlled)
- Skeletal stabilization - external fixation or internal fixation as appropriate
- Wound coverage - local or free tissue transfer when soft tissue deficient
Prosthetic joint infection:
- Early (<3 months): debridement, irrigation, prosthesis retention (DAIR) + antibiotics
- Late (>3 months) or biofilm-established: two-stage revision (implant removal → spacer + antibiotics → reimplantation) - Rosen's Emergency Medicine, p. 3854
9. Special Forms
Tuberculosis Osteomyelitis (Pott's Disease)
- Bloodborne from primary pulmonary focus; approximately 1-3% of all TB cases develop osseous infection
- Typically solitary in immunocompetent; disseminated in immunocompromised
- Most commonly affects the thoracolumbar spine (Pott's disease) - intervertebral discs and adjacent vertebral bodies
- Presentation: insidious - malaise, weight loss, low-grade fever, localized pain
- Classic complication: paraplegia from gibbus deformity and cord compression
- Spina ventosa: TB dactylitis - cyst-like expansion of metacarpal/metatarsal bones ("windy bone")
- Treatment: standard anti-TB regimen (HRZE x 2 months then HR x 10 months); surgery for cord compression or spinal instability - Grainger & Allison's Diagnostic Radiology, p. 1638; Bailey & Love, p. 657
Fungal Osteomyelitis
- Candida (especially in IV drug users, ICU patients, neonates)
- Coccidioides immitis, Blastomyces dermatitidis (endemic mycoses)
- Cryptococcus (immunocompromised)
Chronic Recurrent Multifocal Osteomyelitis (CRMO)
- Rare, non-infectious, autoinflammatory condition mimicking osteomyelitis
- Children and adolescents; symmetrical multifocal lesions
- No pathogen identified; responds to NSAIDs/bisphosphonates
10. Complications
| Complication | Details |
|---|---|
| Chronic osteomyelitis | In 5-25% of acute cases; especially with delayed diagnosis or immunocompromise |
| Septic arthritis | Adjacent joint seeding; more common in neonates where metaphysis is intracapsular |
| Pathologic fracture | Through weakened, infected bone |
| Growth disturbance | Physeal damage in children → limb length discrepancy, angular deformity |
| Bacteremia / sepsis | Hematogenous dissemination from focus |
| Spinal cord compression | From vertebral osteomyelitis / epidural abscess |
| Secondary amyloidosis (AA) | Chronic suppuration triggers SAA → amyloid deposition in kidneys, liver |
| Squamous cell carcinoma | Malignant transformation of chronic sinus tract (Marjolin's ulcer) |
| Sarcoma | Very rare; transformation of chronically infected bone |
11. Key Differentials
- Ewing's sarcoma - can closely mimic acute osteomyelitis radiologically and clinically (fever, pain, onion-skin periosteal reaction)
- Osteosarcoma - periosteal reaction, Codman's triangle; usually no fever
- Septic arthritis - primary joint infection; sympathetic effusion in osteomyelitis can confuse the picture
- Bone infarct (sickle cell) - difficult to distinguish from osteomyelitis on imaging and clinically
- Stress fracture - no systemic signs; localized periosteal reaction
Summary Table
| Feature | Acute Hematogenous | Subacute | Chronic |
|---|---|---|---|
| Onset | Hours-days | Days-weeks | Months-years |
| Pathology | Neutrophils, exudate | Granulation tissue, Brodie abscess | Sequestrum, involucrum, sinus tract |
| X-ray | Normal early | Brodie abscess (lytic + sclerotic rim) | Sequestrum, involucrum, sclerosis |
| MRI | T1 low / T2 high marrow signal | Penumbra sign | Heterogeneous; sinus tracts |
| Treatment | IV antibiotics ± drainage | Antibiotics ± curettage | Surgery + prolonged antibiotics |
Sources: Bailey & Love's Short Practice of Surgery 28th Ed. | Robbins & Kumar Pathologic Basis of Disease (10th Ed.) | Rosen's Emergency Medicine 9th Ed. | Grainger & Allison's Diagnostic Radiology | Goldman-Cecil Medicine | Campbell's Operative Orthopaedics 15th Ed. 2026
Burns every detail for standard MBBS level
Reading File
Finding Sources
Finding Sources
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.