Glottic web and its management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"glottic web" management laryngoscopy
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, well-sourced information. Here is the full answer:
Glottic Web
Definition and Embryology
A glottic web is a membrane of varying thickness that spans the glottic opening, most commonly fusing the vocal cords anteriorly. It results from failure of complete recanalization of the larynx during embryogenesis. The laryngeal lumen is normally obliterated between weeks 7-8 of gestation and recanalized by week 10; incomplete recanalization produces a web. The vast majority involve the anterior glottis, though a rare posterior (interarytenoid) form also exists.
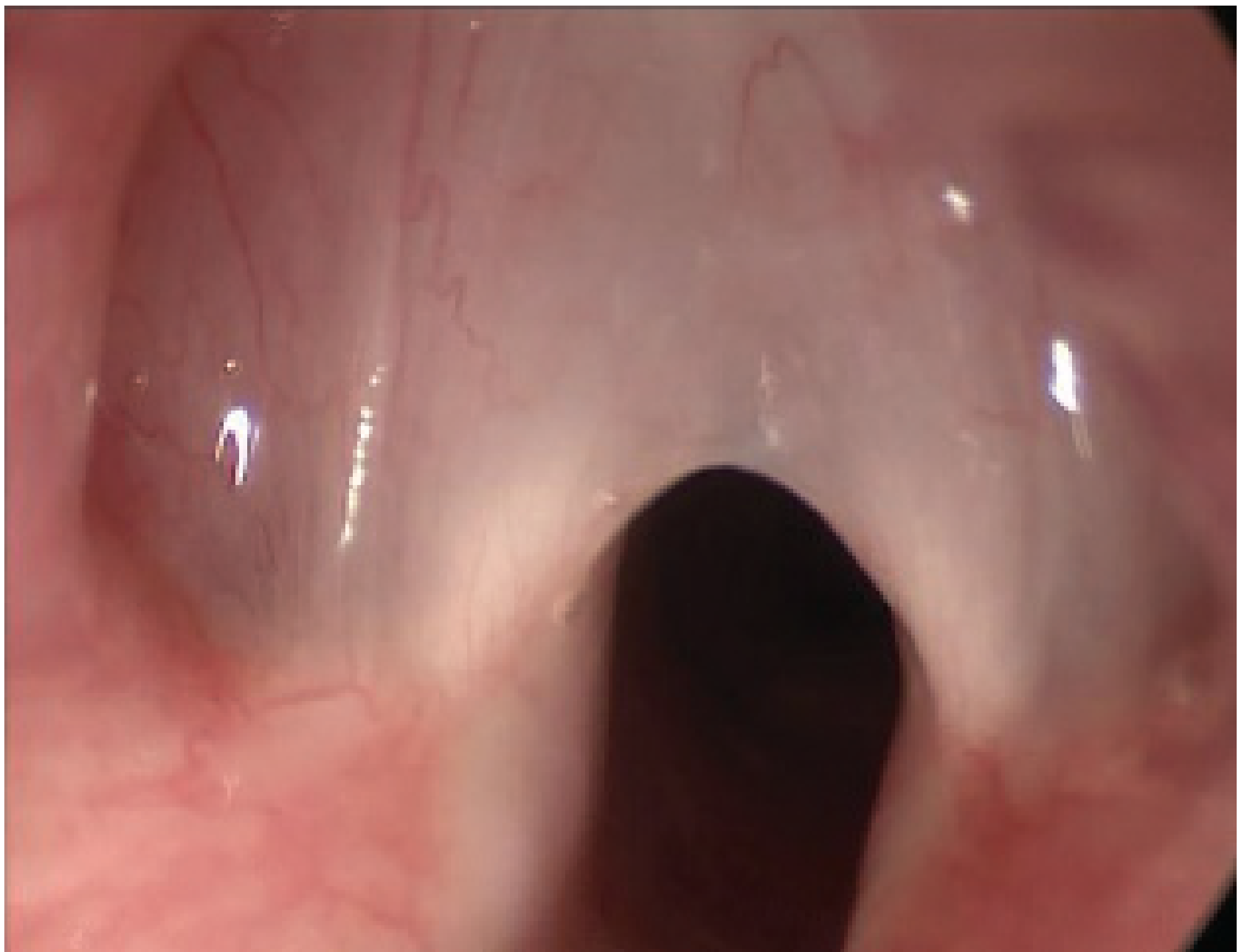
Endoscopic view of an anterior glottic web - the vocal folds are fused anteriorly with a narrow posterior airway opening (Scott-Brown's Otorhinolaryngology)
Classification
Congenital Glottic Web - Cohen Classification
| Type | Extent of Glottic Obstruction | Subglottic Involvement | Symptoms |
|---|---|---|---|
| Type 1 | <35% | None or little | Mild hoarseness |
| Type 2 | 35%-50% | Thin anterior web with little subglottic extension | Hoarse, weak cry, stridor with exertion |
| Type 3 | 50%-75% | Thin-thick web, extends to lower border of cricoid | Severe hoarseness, moderate airway obstruction |
| Type 4 | 75%-90% | Thick web, extends to lower cricoid | Aphonic, severe airway obstruction, requires tracheotomy |
(Cohen SR, Ann Otol Rhinol Laryngol Suppl, 1985)
Types
1. Congenital Glottic Web
- The most common form
- Anterior location in nearly all cases; the web is thin posteriorly near its free border but becomes progressively thicker anteriorly with variable subglottic extension
- Concomitant subglottic stenosis (SGS) is frequent with larger webs (Types 3-4) - the thick anterior component extends inferiorly forming a subglottic "sail" configuration
- Associated with 22q11.2 deletion (velocardiofacial/DiGeorge syndrome) - found in up to 65% of patients with anterior glottic webs
- Also associated with cardiac anomalies, Richieri-Costa Pereira syndrome, and other chromosomal anomalies
2. Acquired Glottic Web
Less common; always post-traumatic in origin. Two main causes:
- Iatrogenic - bilateral mucosal disruption at the anterior commissure (most commonly from laser treatment of laryngeal papillomatosis)
- External trauma - anterior neck trauma with laryngeal fracture
- Prolonged intubation rarely causes anterior glottic stenosis unless SGS is also present
Key distinction from congenital webs: acquired webs are associated with fibrosis and scarring, unlike the normal mucosa seen in congenital webs.
Clinical Presentation
Congenital:
- Weak, high-pitched, squeaky voice or cry from birth
- Inspiratory stridor (variable severity based on web type)
- Recurrent croup in infancy - the combination of a weak cry and recurrent croup should always raise suspicion
- Severe types: near-complete obstruction, aphonia, require emergency airway management
Acquired:
- History of prior laryngeal surgery or trauma
- Progressive dysphonia, hoarseness
- Variable airway compromise depending on web extent
- May be discovered incidentally on endoscopy
Investigations
- Flexible nasopharyngoscopy - initial assessment of web extent and vocal fold mobility
- Direct laryngoscopy / microlaryngoscopy - definitive assessment, allows precise sizing
- Rigid bronchoscopy - critical to assess subglottic involvement (co-existing SGS)
- Genetic screening - all patients with a laryngeal web should be screened for 22q11.2 deletion
- Cardiovascular evaluation - assess for aortic arch anomalies and other cardiac defects (a vascular ring diagnosis may be delayed if stridor is attributed solely to the web)
- Prenatal ultrasound/MRI - for severe cases presenting as CHAOS (Congenital High Airway Obstruction Syndrome), characterized by enlarged echogenic lungs, inverted diaphragms, massive ascites, and dilated fluid-filled lower airways
Management
Management is guided by web type (congenital vs. acquired), severity (Cohen grade), degree of subglottic involvement, and patient age/size.
Conservative Management
- Small webs (Type 1) causing minimal symptoms - observation is appropriate
- Thin webs lysed inadvertently during intubation at birth are unlikely to reform
Endoscopic Management
Simple Endoscopic Division
- Suitable for Type 1 and select Type 2 congenital webs with minimal subglottic extension
- Division along the margin of one vocal cord using a cold knife (sickle knife) or CO2 laser
- If the web is very thin, division alone followed by endoscopic dilatation may allow stable healing without reformation
- CO2 laser is the traditional endoscopic tool; KTP (532 nm) laser has emerged as an option, including in-office awake procedures for adults
Endoscopic Division + Laryngeal Keel Placement
- Used for webs that are thick anteriorly or have subglottic extension that precludes simple division alone
- After web division, a keel (typically Montgomery Keel or a custom silastic sheet) is placed to separate the divided raw mucosal surfaces and prevent re-adhesion
- Keel placement technique (endoscopic approach):
- Web divided with sickle knife or laser under suspension microlaryngoscopy
- Silastic sheeting fashioned into a keel shape, sutured in the anterior midline
- The keel is placed "like the leaves of a book" over the divided mucosa
- Suture placement: "inside-out" technique (Lichtenberger needle driver) or "outside-in" technique (Keith needle + hollow angiocath)
- Keel is left in situ for 10 days to 4 weeks, then removed
- In young children with small larynges, a covering tracheostomy is necessary for the duration of keel placement
Open Surgical Management
Laryngotracheal Reconstruction (LTR) with Anterior Cartilage Grafting
- Required when the web is large with associated SGS that cannot be adequately addressed endoscopically
- Anterior cartilage graft (typically costal cartilage) widens the subglottis
- Can be performed as:
- Single-stage LTR - post-operative endotracheal intubation as a stent for 5-7 days
- Double-stage LTR - performed after tracheostomy, usually deferred to age 1-2 years when the larynx is larger and mucosal dissection can be more precise
Open Laryngofissure + Keel (for Acquired Webs)
- The standard approach for acquired anterior glottic webs, which have fibrotic/scarred mucosa
- Steps:
- Complete laryngofissure (ideally performed with endoscopic guidance)
- Assessment of demucosalized scar at anterior vocal folds
- Attempt mucosal pexing sutures from cut edges toward thyroid ala
- Mandatory keel placement (Montgomery Keel) - sized to fit without impinging on posterior commissure or disrupting the epiglottic petiole insertion
- Laryngofissure closed with keel in situ
- Keel removed at 10 days to 4 weeks via open approach; midline defect closed with mattress sutures
- Antibiotic coverage and antireflux measures are recommended while the keel is in place and for a few days after removal
- In congenital webs, if mucosa is normal, a pexing suture may occasionally reconstruct the anterior commissure without a keel
Emergency/Neonatal Management
- Tracheostomy - performed for severe (Type 4) webs with critical airway compromise; often the first-line measure in a neonate with a life-threatening obstruction
- EXIT procedure (Ex utero Intrapartum Treatment) - for prenatally diagnosed CHAOS; emergency tracheostomy is performed while the neonate remains on placental support (via elective Caesarean section)
Management Summary by Grade
| Cohen Type | Approach |
|---|---|
| Type 1 | Conservative or simple endoscopic division ± dilation |
| Type 2 (thin) | Endoscopic division ± keel |
| Type 2-3 (thick, +/- subglottis) | Endoscopic division + keel; tracheostomy cover in young children |
| Type 4 / severe SGS | Tracheostomy + staged LTR with anterior cartilage graft |
| Acquired web (any) | Open laryngofissure + keel (mandatory due to fibrosis) |
| Prenatal diagnosis / CHAOS | EXIT procedure at delivery |
Outcomes and Special Considerations
- Voice: Even after successful airway rehabilitation, voice quality is often less favorable in complex webs, particularly after multiple procedures. This must be counseled pre-operatively.
- Recurrence: The main challenge with web repair is re-formation; keel placement dramatically reduces this risk but does not eliminate it.
- Genetic workup: All patients should be screened for 22q11.2 deletion and assessed for cardiac anomalies before elective surgery.
- Novel approaches: In-office KTP laser lysis for thin adult acquired webs has been reported (PMID: 39613704), and a bi-layered microflap technique (2025) offers a refined approach to prevent web recurrence (PMID: 40926048).
Sources:
- Cummings Otolaryngology Head and Neck Surgery, pp. 3895-3896
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2, pp. 379, 402
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (main volume), p. 1162
- Cohen SR. Congenital glottic webs in children. Ann Otol Rhinol Laryngol Suppl, 1985
This is a shared conversation. Sign in to Orris to start your own chat.