
inbound517580238839761324.jpg
Please give proper answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive, well-structured answer. Here is the full response:
Clinical Case: Mitral Stenosis
Diagnosis
Mitral Stenosis (MS) - most likely rheumatic in origin.
The clinical triad that clinches this diagnosis:
- Gradual-onset dyspnea + orthopnoea + PND - classic features of left-sided heart failure from elevated left atrial pressure
- Young female (30 years) - rheumatic MS has a 3:1 female preponderance and presents in the 3rd-4th decade in developing countries
- Mid-diastolic murmur at the mitral area - the pathognomonic auscultatory finding of MS (low-pitched rumbling murmur, best heard at the apex with the bell in left lateral position, breath held in expiration)
Pathophysiology
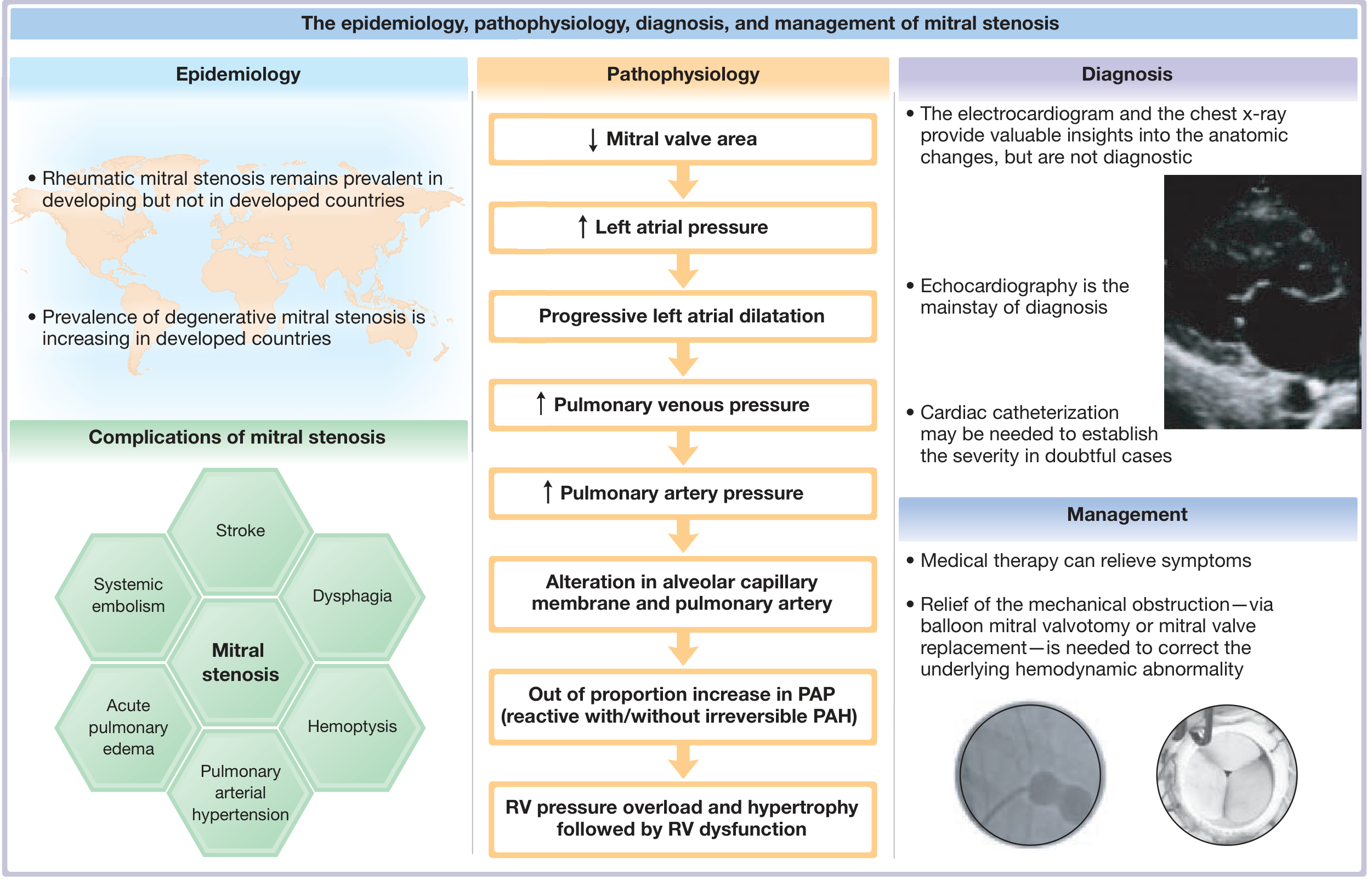
Central illustration from Fuster and Hurst's The Heart, 15th Edition
Step 1 - Structural Valve Changes
Rheumatic fever causes inflammation of the mitral valve. The main pathology is commissural fusion, leaflet thickening, chordal fusion, and shortening, producing the classic "fish-mouth" appearance on surgery (arrows in the image below):
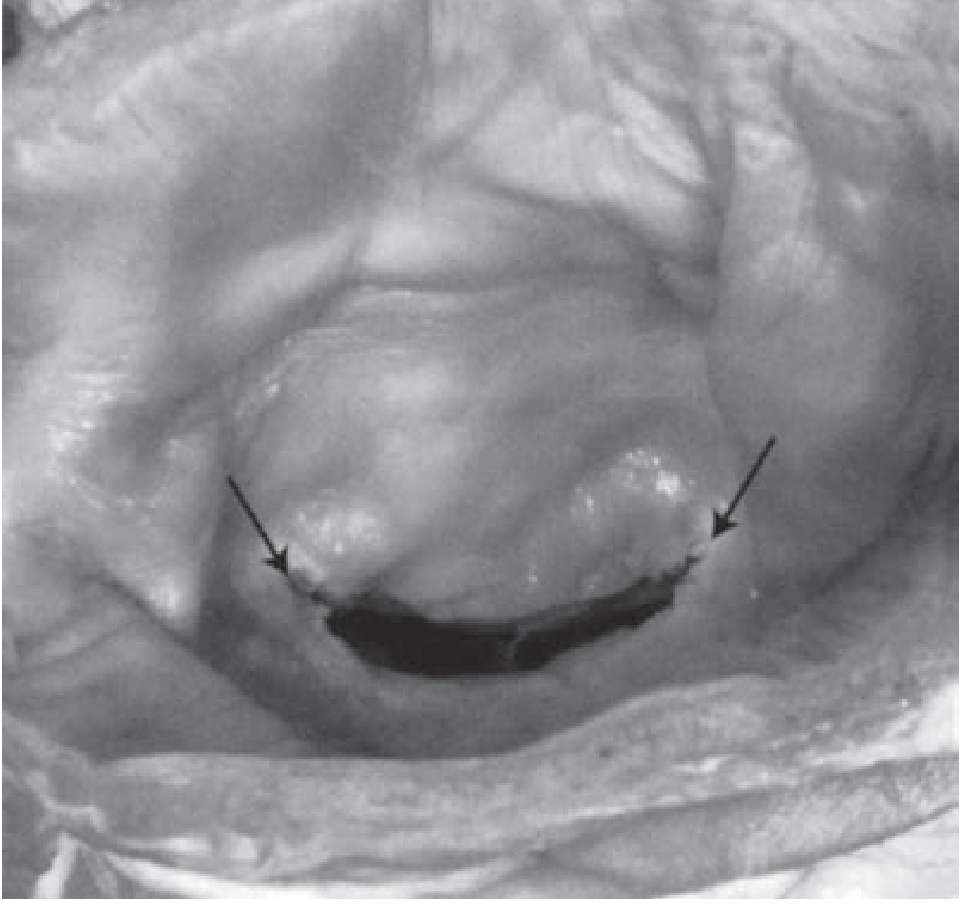
The normal mitral valve area (MVA) is 4-6 cm². As the valve narrows progressively, a persistent diastolic pressure gradient develops between the left atrium (LA) and left ventricle (LV).
Step 2 - Left Atrial Pressure Rise
Because blood cannot flow freely from LA to LV during diastole, LA pressure rises progressively. This is the hemodynamic hallmark of MS. The elevated LA pressure causes:
- Left atrial dilatation (hypertrophy of atrial muscle + interstitial fibrosis)
- Atrial fibrillation (AF) - the most common complication, seen in ~40% of patients
- LA thrombus formation (especially in the left atrial appendage) - risk of systemic embolism
Step 3 - Pulmonary Venous Hypertension
Raised LA pressure is transmitted backward into the pulmonary veins and capillaries, causing:
- Pulmonary congestion and interstitial oedema - this produces dyspnoea on exertion, orthopnoea, and PND
- Haemoptysis (from rupture of dilated bronchial veins)
- Pulmonary oedema in severe cases
Step 4 - Pulmonary Arterial Hypertension (PAH)
Initially, pulmonary artery pressure (PAP) rises due to passive retrograde transmission of elevated LA pressure (pulmonary vascular resistance is normal). In severe MS, PAP rises disproportionately - this is reactive PAH, caused by:
- Pulmonary arteriolar vasoconstriction (largely reversible after relief of MS)
- Morphologic changes in the pulmonary vasculature - intimal thickening, medial hypertrophy (fixed component; may or may not reverse post-intervention)
Step 5 - Right Ventricular Failure
Reactive PAH causes RV pressure overload → RV hypertrophy → eventual RV failure (due to afterload excess, not contractile dysfunction). Since RV and LV are in series, reduced RV output further reduces LV filling, lowering cardiac output and causing systemic hypotension. This manifests as JVP elevation, hepatomegaly, ascites, and peripheral oedema.
Summary Chain:
↓ MVA → ↑ LA pressure → LA dilatation + AF + thrombus → ↑ pulmonary venous pressure → pulmonary congestion (SOB, orthopnoea, PND) → ↑ PAP (reactive PAH) → RV pressure overload → RV hypertrophy → RV failure → ↓ cardiac output
Auscultatory Signs (Relevant to This Case)
| Sign | Mechanism |
|---|---|
| Loud S1 | Transmitral gradient holds valve fully open; LV systole closes it forcefully from open position |
| Opening snap (OS) after S2 | Stiff but pliable leaflet snaps open; shorter S2-OS interval = more severe MS |
| Mid-diastolic rumble | Blood passing through narrow valve orifice in diastole |
| Presystolic accentuation | Atrial contraction (only in sinus rhythm) |
| Loud P2 | If pulmonary hypertension has developed |
Management
Management is guided by symptom status, MVA, and valve morphology (Wilkins score).
1. General Measures
- Activity restriction in symptomatic patients
- Salt restriction and weight management
- Antibiotic prophylaxis against Group A Streptococcus (penicillin monthly/daily) to prevent further rheumatic attacks - this is especially important for secondary prevention
2. Medical Therapy
Medical therapy relieves symptoms but does not correct the underlying haemodynamic obstruction.
| Drug | Indication | Purpose |
|---|---|---|
| Diuretics (furosemide) | Congestion (SOB, orthopnoea) | Reduce preload, relieve pulmonary oedema |
| Beta-blockers (metoprolol/bisoprolol) | Sinus rhythm or AF | Slow heart rate → prolong diastolic filling time → better LV filling |
| Digoxin | AF with rapid ventricular rate | Rate control |
| Anticoagulation (warfarin, target INR 2-3) | AF, previous embolism, LA thrombus | Prevent systemic thromboembolism |
| Diuretics + nitrates | Acute pulmonary oedema | Emergency symptom relief |
| Sildenafil / nitric oxide (select cases) | Reactive PAH | Reduce pulmonary vascular resistance |
3. Interventional Treatment - Relieving the Mechanical Obstruction
This is the definitive treatment and the only way to correct the haemodynamic abnormality.
A. Percutaneous Balloon Mitral Valvotomy (PBMV / BMV)
- Procedure of choice for suitable anatomy
- A balloon catheter is advanced across the interatrial septum (transseptal puncture) and inflated across the mitral valve to split the fused commissures
- Indication: Symptomatic MS (NYHA class II-IV) with MVA ≤1.5 cm² AND favourable valve anatomy (Wilkins score ≤8)
- Contraindications: Significant MR (≥2+), LA thrombus, severe subvalvular disease, heavily calcified valves
- Results in immediate doubling of MVA, substantial reduction in transmitral gradient and LA pressure
- Long-term results: 5-year event-free survival of 60-90%
B. Surgical Options
When PBMV is contraindicated or has failed:
- Open Mitral Commissurotomy (OMC) - surgical splitting of fused commissures on cardiopulmonary bypass; preferred when anatomy is borderline
- Mitral Valve Replacement (MVR) - for severely distorted, calcified valves or when significant MR coexists
- Mechanical valve (St. Jude's bileaflet): requires lifelong anticoagulation; preferred in young patients
- Bioprosthetic valve: no long-term anticoagulation needed; but limited durability (~15 years); preferred in elderly or those who cannot take anticoagulants
4. Management of Complications
| Complication | Management |
|---|---|
| Atrial fibrillation | Rate control (beta-blocker/digoxin), anticoagulation; cardioversion if recent onset |
| Systemic embolism | Warfarin (lifelong if permanent AF), INR 2-3 |
| Pulmonary oedema | IV furosemide, oxygen, morphine, sitting position |
| Haemoptysis | Rest, diuretics; rule out pulmonary embolism |
| Infective endocarditis | Prophylaxis for dental procedures; treat with appropriate antibiotics |
Severity Assessment (ACC/AHA Classification)
| Severity | MVA | Mean Gradient | PASP |
|---|---|---|---|
| Mild | >1.5 cm² | <5 mmHg | <30 mmHg |
| Moderate | 1.0-1.5 cm² | 5-10 mmHg | 30-50 mmHg |
| Severe | <1.0 cm² | >10 mmHg | >50 mmHg |
Severe MS is now defined (2014 ACC/AHA) as MVA ≤1.5 cm² in symptomatic patients.
Key Investigations to Order
- Echocardiography (TTE) - mainstay of diagnosis; measures MVA (planimetry, pressure half-time), transmitral gradient, LA size, Wilkins score, pulmonary pressures, LV function
- ECG - P-mitrale (bifid P in lead II, biphasic in V1), RVH, AF
- Chest X-ray - straightening of left heart border (LA enlargement), double atrial shadow, Kerley B lines, pulmonary plethora
- Cardiac catheterization - when echo inconclusive; measures transmitral gradient directly via simultaneous LA and LV pressures (or PCWP as surrogate)
- TEE - rule out LA thrombus before PBMV or cardioversion
Sources: Fuster and Hurst's The Heart, 15th Edition (Chapter 32) | Braunwald's Heart Disease, 11th Edition (Chapter 69)

inbound1064371894066886296.jpg
Please give detail answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the detail needed. Let me compose the comprehensive answer:
Clinical Case: 65-Year-Old Male with Acute Severe Retrosternal Chest Pain + Sweating x 3 Hours
Diagnosis: Acute ST-Elevation Myocardial Infarction (STEMI) - Until Proven Otherwise
This is a time-critical medical emergency. The presentation - acute-onset severe retrosternal chest pain with diaphoresis (sweating) lasting 3 hours in a 65-year-old male - is the classic presentation of STEMI. Mortality is directly proportional to total ischemia time. Every minute counts.
Differential Diagnoses to Consider (and Exclude Rapidly)
| Condition | Distinguishing Features |
|---|---|
| STEMI (most likely) | Retrosternal pressure/pain, radiation to arm/jaw, diaphoresis, ST elevation on ECG |
| NSTEMI/Unstable Angina | Similar presentation, no ST elevation, positive troponins |
| Aortic Dissection | Tearing pain radiating to back, BP difference between arms, wide mediastinum on CXR |
| Pulmonary Embolism | Pleuritic chest pain, dyspnoea, hypoxia, haemoptysis, DVT history |
| Acute Pericarditis | Sharp, positional chest pain, worse lying down, pericardial rub, saddle-shaped ST elevation |
| Oesophageal rupture | Preceded by vomiting, subcutaneous emphysema, hydropneumothorax |
STEP 1: IMMEDIATE APPROACH ON ARRIVAL (First 10 Minutes)
A. Simultaneous Assessment and Action - "TIME = MYOCARDIUM"
The moment the patient arrives, do all of these simultaneously:
- IV access - two large-bore peripheral lines
- Monitoring - continuous cardiac monitor + pulse oximetry + blood pressure
- 12-lead ECG - must be obtained and interpreted within 10 minutes of arrival (AHA/ACC guideline)
- Brief targeted history - pain character, onset, duration, radiation, associated symptoms, risk factors, medications, contraindications to thrombolysis
- Rapid physical examination - vitals (both arms BP to exclude aortic dissection), JVP, lung auscultation, heart sounds, peripheral pulses, neurological status
B. History to Obtain Rapidly
OPQRST of chest pain:
- Onset: Sudden? Activity-related?
- Provocation/Palliation: Nothing relieves it (unlike angina)
- Quality: Pressure, heaviness, tightness, crushing ("elephant sitting on chest")
- Radiation: Left arm, jaw, neck, epigastrium (inferior MI), back (dissection)
- Severity: Usually severe, 8-10/10
- Time: Duration ≥ 20 minutes suggests MI
Associated symptoms: Sweating (diaphoresis), nausea, vomiting, dyspnoea, palpitations, syncope, sense of impending doom
Risk factors for CAD: Hypertension, diabetes mellitus, smoking, dyslipidaemia, family history of IHD, obesity, physical inactivity
Contraindications to thrombolysis (assess if PCI not available):
- Prior intracranial haemorrhage, recent stroke within 3 months, major surgery within 3 weeks, active bleeding, SBP >180 mmHg, aortic dissection, acute pericarditis, pregnancy
STEP 2: IMMEDIATE INVESTIGATIONS
A. ECG (Most Critical - Do First)
Diagnostic ECG criteria for STEMI (2 or more contiguous leads):
| ST Elevation Location | Myocardial Territory | Culprit Artery |
|---|---|---|
| V1-V6 or new LBBB | Anterior + septal walls | Proximal LAD or Left Main |
| V2-V4 | Anterior wall | LAD |
| V5-V6 | Lateral wall | LCX |
| II, III, aVF | Inferior wall | RCA or LCX |
| I, aVL | High lateral wall | Diagonal or proximal LCX |
Thresholds for STEMI diagnosis:
- Men >40 years: ≥2 mm in V2-V3, ≥1 mm in all other leads
- Right-sided leads (V3R, V4R): must be obtained in inferior MI to rule out RV infarction (treated differently - avoid nitrates and diuretics)
ECG evolution of STEMI:
- Hyperacute peaked T waves (earliest sign, minutes)
- ST elevation (within hours)
- Q wave development (transmural necrosis, hours to days)
- T wave inversion
- ST normalisation
Get serial ECGs if initial ECG is normal but chest pain persists - evolving STEMI may be missed on first ECG.
B. Blood Tests (Send Simultaneously - Do NOT Wait for Results Before Starting Treatment)
| Test | Purpose |
|---|---|
| Cardiac Troponin I/T (serial at 0h and 3h) | Confirms myocardial necrosis; may be normal in first 3-6 hours |
| CK-MB | Rises at 3-6h, peaks 12-24h; useful for re-infarction |
| CBC | Baseline, anaemia can precipitate ACS |
| Renal function, electrolytes, Mg²⁺ | Guides drug dosing; hypokalaemia/hypomagnesaemia → arrhythmias |
| Coagulation (aPTT, PT/INR) | Baseline before anticoagulation and thrombolysis |
| Blood glucose | Hyperglycaemia worsens outcomes; insulin infusion if >180 mg/dL |
| Lipid profile | Secondary prevention planning |
| Type and screen | Pre-PCI/CABG preparation |
Important: Initial troponins may be normal within the first 3 hours. Do NOT withhold treatment if the ECG shows STEMI - do not wait for biomarkers.
C. Chest X-Ray (Portable)
- Pulmonary oedema (Kerley B lines, perihilar haziness, cardiomegaly)
- Wide mediastinum (aortic dissection)
- Pneumothorax (alternative diagnosis)
- Cardiomegaly
D. Echocardiography (Bedside TTE)
- If diagnosis is unclear after ECG and history
- Identifies regional wall motion abnormalities confirming ischemia
- Assesses LV function (EF), RV function, pericardial effusion, mechanical complications (MR, VSD)
STEP 3: IMMEDIATE MANAGEMENT ("MONA-B" + Reperfusion)
Initial Stabilisation
- Oxygen - only if SpO₂ <90%; routine oxygen in normoxaemic patients is not beneficial and may be harmful
- IV access - two large-bore lines
- Continuous ECG monitoring - ready for defibrillation (VF causes 50% of early STEMI mortality, often in the first hour)
- Position - sitting position or semi-recumbent if breathless
A. Antiplatelet Therapy (Immediate, Dual Antiplatelet - DAPT)
| Drug | Dose | Notes |
|---|---|---|
| Aspirin | 162-325 mg chewed/crushed | Non-enteric coated; give immediately; fastest platelet inhibition |
| Ticagrelor (preferred) | 180 mg loading, then 90 mg BD | Better than clopidogrel; shown mortality benefit; use if PCI planned |
| OR Prasugrel | 60 mg loading, then 10 mg/day | More potent; do NOT give if age >75 years, weight <60 kg, or prior stroke/TIA |
| OR Clopidogrel | 600 mg loading, then 75 mg/day | Use if fibrinolysis planned or if ticagrelor/prasugrel not available |
B. Anticoagulation
| Drug | Dose | Notes |
|---|---|---|
| UFH (preferred for PCI) | 60 units/kg IV bolus, then 12 units/kg/h (max bolus 4000 units) | Real-time monitoring with ACT in cath lab |
| Enoxaparin (for thrombolysis) | 30 mg IV bolus, then 1 mg/kg SC BD | Reduce dose in age >75 years (no loading dose, 0.75 mg/kg SC BD) |
| Fondaparinux | 2.5 mg IV bolus, then 2.5 mg SC daily | Superior to UFH with thrombolysis; do not use alone for PCI |
C. Anti-ischaemic Therapy
| Drug | Dose | Notes |
|---|---|---|
| Nitroglycerin (GTN) | 0.4 mg SL every 5 min x 3 doses; or 10-200 μg/min IV infusion | Reduces preload and coronary vasospasm; AVOID if: SBP <90 mmHg, HR <50 or >100 bpm, RV infarct, phosphodiesterase inhibitor use in past 48h |
| Morphine | 2-4 mg IV (titrate) | For refractory pain not responding to nitrates; causes vasodilation; use cautiously - may mask ischaemic symptoms |
| Beta-blocker (oral) | Metoprolol 25-50 mg oral | Start within 24h if: no signs of HF, not in cardiogenic shock, SBP ≥120 mmHg, HR 60-110 bpm, no advanced heart block; Reduces infarct size, prevents arrhythmias, limits remodelling |
D. Reperfusion Therapy - THE PRIORITY
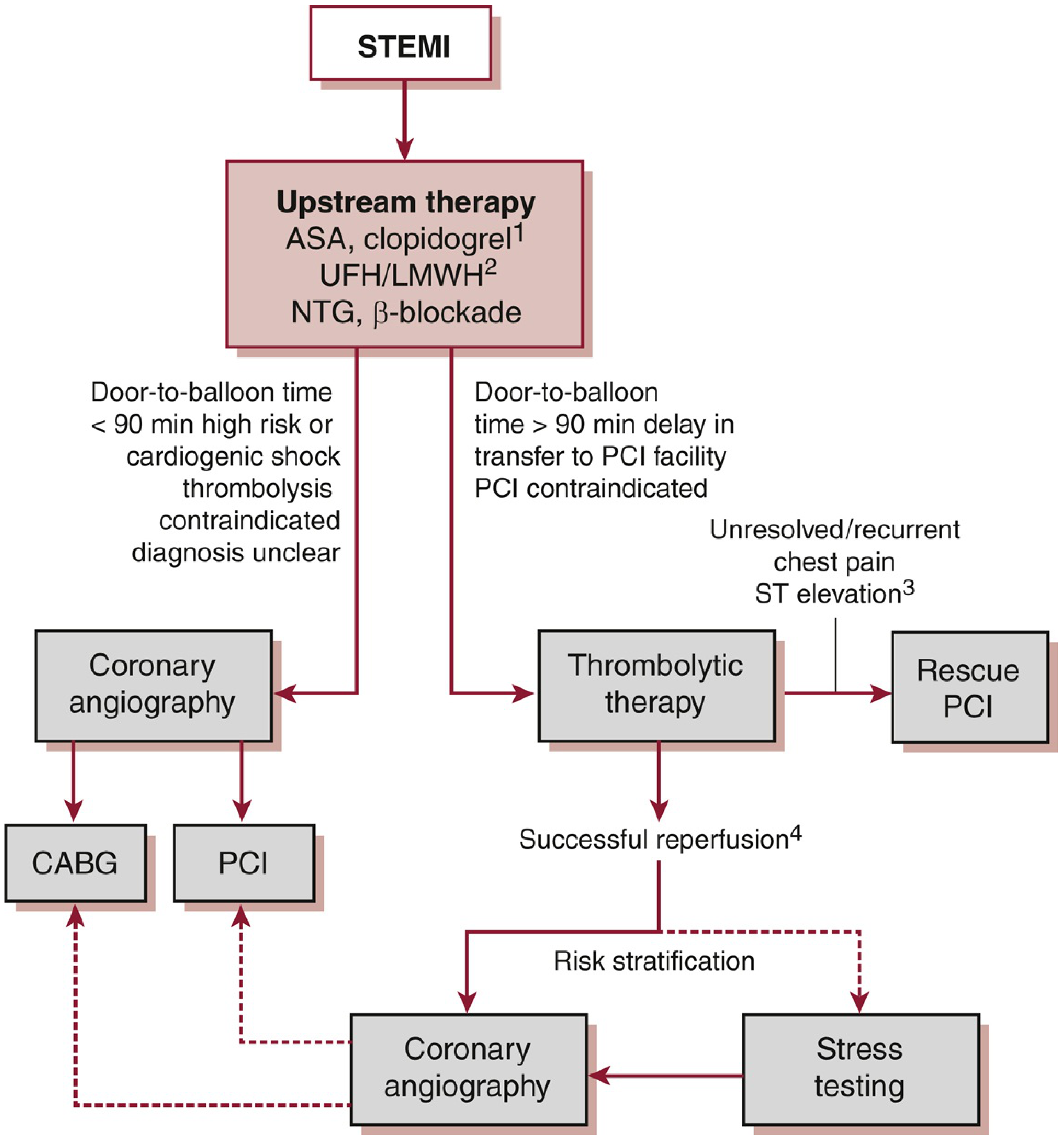
The single most important treatment is rapid restoration of coronary blood flow.
Option 1: Primary PCI (Percutaneous Coronary Intervention) - PREFERRED
- Goal: Door-to-balloon time ≤90 minutes from first medical contact
- Superior to thrombolysis in all outcomes: better vessel patency (TIMI 3 flow), less re-infarction, less intracranial haemorrhage, improved survival
- Preferred in ALL of these situations:
- PCI available within 90 min
- Cardiogenic shock / Killip class III-IV (even if transfer required)
- Contraindications to thrombolysis
- Late presentation (>3h from symptom onset)
- Prior CABG or PCI
Procedure: Emergency coronary angiography → identify culprit artery → balloon angioplasty → stent placement (drug-eluting stent preferred) → consider complete revascularisation of non-culprit vessels
Option 2: Fibrinolytic (Thrombolytic) Therapy
- When: Primary PCI not available within 120 minutes (transfer time >120 min)
- Goal: Door-to-needle time ≤30 minutes
- Most effective in first 3 hours of symptom onset; benefit tapers after 3h but still given up to 12h
- Transfer to PCI-capable centre after fibrinolysis for routine angiography within 24 hours
| Drug | Dose | Notes |
|---|---|---|
| Tenecteplase (TNK-tPA) | Weight-based single IV bolus | Agent of choice - single bolus, less bleeding, similar efficacy |
| Alteplase (rt-PA) | 15 mg IV bolus, then 0.75 mg/kg over 30 min, then 0.5 mg/kg over 60 min | Fibrin-specific |
| Streptokinase | 1.5 million units IV over 60 min | Cheapest; widely available worldwide; causes allergic reactions; do not repeat |
Signs of successful reperfusion (watch for at 60-90 min):
- Chest pain relief
- ≥50% reduction in ST elevation
- Idioventricular rhythm (accelerated idioventricular rhythm)
- Peak CK-MB at 12h (earlier than expected)
Rescue PCI if thrombolysis fails (no symptom relief, <50% ST resolution at 60-90 min) - urgent transfer for PCI.
Absolute Contraindications to Thrombolysis:
- Prior intracranial haemorrhage
- Ischaemic stroke within 3 months
- Known intracranial structural lesion (AVM, aneurysm)
- Aortic dissection
- Active bleeding / bleeding diathesis
- Acute pericarditis
- Closed head injury within 3 months
- Severe uncontrolled hypertension (SBP >180 mmHg, DBP >110 mmHg)
STEP 4: SUBSEQUENT MANAGEMENT (In-Hospital)
E. Additional Medications
| Drug | Indication | Timing |
|---|---|---|
| ACE inhibitor (ramipril, lisinopril) | All STEMI patients, especially with reduced EF, anterior MI, HF, hypertension | Within 24h, if haemodynamically stable |
| Statin (high-intensity: atorvastatin 80 mg) | All STEMI patients regardless of cholesterol | Immediately |
| Aldosterone antagonist (eplerenone) | LVEF ≤40% + HF symptoms or diabetes | After 3-7 days |
| SGLT2 inhibitor (empagliflozin) | HFrEF post-MI, diabetics | Before discharge |
F. Monitoring and Complications to Watch For
| Complication | Signs | Management |
|---|---|---|
| Ventricular fibrillation (VF) | Most common cause of early death | Immediate DC defibrillation (200 J biphasic) |
| Cardiogenic shock | SBP <90 mmHg, cold extremities, oliguria | IV fluids (if RV infarct), vasopressors (noradrenaline), intra-aortic balloon pump, urgent revascularisation |
| Acute pulmonary oedema | Breathlessness, pink frothy sputum, bilateral crepitations | O2, morphine, IV furosemide, GTN infusion, CPAP |
| Complete heart block (inferior MI) | Bradycardia, hypotension | Temporary pacing |
| Papillary muscle rupture | New loud pansystolic murmur, flash pulmonary oedema | Emergency surgery |
| Ventricular septal defect | New harsh systolic murmur at LSE, step-up in O2 saturation | Emergency surgery |
| Free wall rupture | Sudden haemodynamic collapse, tamponade | Emergency surgery |
Killip Classification (Risk Stratification)
| Class | Features | In-Hospital Mortality |
|---|---|---|
| I | No HF | ~6% |
| II | S3 gallop, basal crepitations, JVP elevated | ~17% |
| III | Frank pulmonary oedema | ~38% |
| IV | Cardiogenic shock | ~67% |
STEP 5: SECONDARY PREVENTION (Before Discharge)
- DAPT for 12 months (aspirin lifelong)
- Beta-blocker (metoprolol/bisoprolol) - long-term
- High-intensity statin (atorvastatin 80 mg) - lifelong
- ACE inhibitor/ARB - especially if LVEF ≤40%
- Cardiac rehabilitation programme
- Risk factor modification: Smoking cessation, blood pressure control, diabetes management, weight loss, exercise
- Echocardiography before discharge to assess LV function
Summary Timeline (AHA/ACC Targets)
| Event | Target Time |
|---|---|
| First ECG after arrival | ≤10 minutes |
| Door-to-balloon (primary PCI) | ≤90 minutes |
| Door-to-needle (thrombolysis) | ≤30 minutes |
| Transfer to PCI-capable facility after thrombolysis | Within 24 hours |
Key message: Left untreated, STEMI mortality exceeds 30%. With primary PCI, in-hospital mortality is now 6-10%. The single most effective intervention is rapid reperfusion - every 30-minute delay in treatment increases 1-year mortality by approximately 7.5%.
Sources: The Washington Manual of Medical Therapeutics (Chapter 4 - STEMI) | Goldman-Cecil Medicine, International Edition (Chapter 58 - ST-Elevation Acute MI) | Fuster and Hurst's The Heart, 15th Edition

IMG_20260712_220549_687.jpg
Interpret and give proper review of the test.
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the detail needed. Here is the full, comprehensive interpretation:
Lab Report Interpretation: High Sensitivity C-Reactive Protein (hs-CRP)
Patient Details
- Name: Debashree Mandal
- Age/Sex: 19 years / Female
- Sample: Serum (Barcode: 0F097971)
- Test Package: Aarogyam C Pro Package (Thyrocare)
- Method: Immunoturbidimetry (Fully Automated Latex Agglutination - Beckman Coulter)
- Report Date: 21 Jun 2026
Result at a Glance
| Test | Value | Units | Risk Category |
|---|---|---|---|
| hs-CRP | 2.78 | mg/L | Average Risk (1.00 - 3.00) |
What Does This Result Mean?
The hs-CRP value of 2.78 mg/L places this patient in the "Average Risk" category per the lab's reference intervals:
| Range | Risk Classification |
|---|---|
| < 1.00 mg/L | Low Risk |
| 1.00 - 3.00 mg/L | Average Risk ← Patient is here (2.78) |
| 3.00 - 10.00 mg/L | High Risk |
| > 10.00 mg/L | Possibly non-cardiac inflammation |
The value is within the average-risk bracket but sitting at the upper end of it (2.78 out of 3.00). This means she is approaching, but not yet crossing into, the high-risk zone.
What is hs-CRP? Understanding the Test
C-Reactive Protein (CRP) is an acute-phase reactant protein produced by the liver, first isolated in 1930. It is released in response to:
- Acute infection or tissue injury (rises 100-1000x)
- Chronic low-grade systemic inflammation (small but measurable rise)
High-Sensitivity CRP (hs-CRP) is a more precise version of the standard CRP test, designed to detect the small elevations associated with chronic vascular inflammation and cardiovascular disease risk - even when standard CRP appears "normal."
The key insight is that atherosclerosis (plaque buildup in arteries) involves chronic, low-grade inflammation. CRP is a marker of this process. Epidemiologic studies including the landmark Women's Health Study and Physicians Health Study found that individuals with higher baseline hs-CRP - even within the "normal" range - had significantly increased risk of heart attack and stroke.
The AHA/CDC Joint Committee established the widely used three-tier risk classification:
- <1 mg/L = Low cardiovascular risk
- 1-3 mg/L = Intermediate/Average cardiovascular risk
- >3 mg/L = High cardiovascular risk
(Per Henry's Clinical Diagnosis and Management by Laboratory Methods)
How to Interpret This Result in Context: A 19-Year-Old Female
Is this concerning?
The result needs to be interpreted carefully in this patient's specific context:
1. Age consideration:
At 19 years, the baseline expected hs-CRP is low (typically <1 mg/L in healthy young adults). A value of 2.78 mg/L - while technically in the "average risk" band - is above what would normally be expected in a healthy 19-year-old female. In young people, most clinicians would want to investigate why it is elevated.
2. What could cause a 2.78 mg/L hs-CRP in a 19-year-old?
A value in the 1-3 mg/L range in a young person is unlikely to reflect established atherosclerosis. Far more common causes include:
| Cause | Notes |
|---|---|
| Subclinical infection | Viral or bacterial (including dental, UTI, upper respiratory) |
| Obesity | Adipose tissue produces IL-6 → triggers CRP; even "normal weight" but high body fat percentage can elevate hs-CRP |
| Polycystic Ovarian Syndrome (PCOS) | Very common in young females; associated with chronic low-grade inflammation and elevated hs-CRP |
| Insulin resistance / prediabetes | Even without overt diabetes |
| Hormonal factors | Oral contraceptive pill use increases CRP |
| Autoimmune diseases | Rheumatoid arthritis, SLE, thyroiditis (early/subclinical) |
| Menstrual cycle | Slight physiological variation |
| Sedentary lifestyle / poor diet | Inflammation from metabolic causes |
| Smoking | Even passive smoking |
| Psychological stress | Chronic stress can mildly elevate inflammatory markers |
3. Is she truly at cardiovascular risk?
As shown in the Framingham Heart Study data and the graph from Robbins Pathology - CRP adds prognostic value at all levels of traditional Framingham risk. However, for a 19-year-old female:
- Traditional 10-year cardiovascular risk is essentially very low regardless
- The hs-CRP here is more likely signalling underlying low-grade inflammation rather than established atherosclerotic disease
The 2019 ACC/AHA Primary Prevention Guideline states that hs-CRP ≥ 2.0 mg/L is an "ASCVD risk enhancer" - a finding that may influence decisions about preventive therapy in borderline-risk patients. For a 19-year-old, this should primarily prompt identifying and correcting the underlying cause of inflammation.
One Important Caveat: Single Test Limitation
The lab report itself correctly states:
"A coronary artery disease risk assessment should be based on the average of two hs-CRP tests, ideally taken two weeks apart."
Per AHA/CDC recommendations:
- If hs-CRP >10 mg/L - discard the result; look for acute infection or inflammation, repeat in 2 weeks
- For the 1-3 mg/L range - a second measurement 2 weeks later is recommended to confirm the finding before drawing conclusions
This single result of 2.78 mg/L should ideally be confirmed with a second test 2 weeks later, especially if the patient had any recent illness, dental procedure, or physical stress at the time of testing.
Recommended Next Steps
Given that this is a young 19-year-old female with hs-CRP 2.78 mg/L (upper end of average risk), the following should be considered:
Immediate
- Repeat hs-CRP in 2 weeks (standard recommendation before drawing any clinical conclusion)
- Correlate with clinical symptoms - any fever, fatigue, joint pains, skin rash, pelvic symptoms?
Investigations to Consider (with clinical correlation)
| Test | Purpose |
|---|---|
| CBC with differential | Rule out infection, anaemia |
| ESR | General inflammatory marker |
| Fasting glucose + HbA1c | Insulin resistance/prediabetes |
| Fasting lipid profile | Combined with hs-CRP for overall cardiovascular risk |
| Thyroid function (TSH, T3, T4) | Thyroiditis can raise CRP |
| ANA, anti-dsDNA | Rule out SLE if symptoms suggest |
| Urine routine | Rule out subclinical UTI |
| Pelvic ultrasound | If PCOS is suspected (irregular cycles, weight gain, hirsutism) |
| BMI + waist circumference | Assess metabolic risk |
Lifestyle Interventions (Regardless of Cause)
These are proven to lower hs-CRP:
- Regular aerobic exercise (30 min/day, 5 days/week) - reduces hs-CRP by ~30%
- Dietary modification - Mediterranean diet, reduce processed foods and refined carbohydrates
- Weight loss if overweight - even modest 5-10% reduction significantly lowers hs-CRP
- Smoking cessation if applicable
- Adequate sleep (chronic sleep deprivation raises CRP)
- Stress management
Summary
| Point | Interpretation |
|---|---|
| Value | 2.78 mg/L - Upper end of "Average Risk" zone |
| Classification | Average cardiovascular risk (not high risk, not low risk) |
| Concern | Elevated for a healthy 19-year-old - needs clinical context |
| Most likely cause | Low-grade inflammation (PCOS, subclinical infection, metabolic, lifestyle) rather than atherosclerosis |
| Action needed | Repeat test in 2 weeks; evaluate for underlying cause; lifestyle modification |
| Cardiovascular concern at age 19? | Low immediate concern, but worth addressing the underlying inflammation early |
Bottom line: This is not alarming but should not be dismissed - especially in a young woman. The result should be repeated and correlated with clinical examination, symptoms, and other metabolic markers. Identifying and correcting the underlying cause of this low-grade inflammation now is the best long-term cardiovascular health investment.
Sources: Henry's Clinical Diagnosis and Management by Laboratory Methods, 24th Edition | Tietz Textbook of Laboratory Medicine, 7th Edition | Robbins, Cotran & Kumar Pathologic Basis of Disease, 10th Edition
IMG_20260712_220549_687.jpg
Interpret the test report and give proper review
This is the same report I just fully interpreted in my previous response. Here is a complete, detailed review for your reference:
Lab Report Interpretation: hs-CRP (High Sensitivity C-Reactive Protein)
Patient Summary
| Field | Details |
|---|---|
| Patient | Debashree Mandal, 19 years / Female |
| Lab | Thyrocare Technologies Ltd. (NABL Accredited) |
| Sample Type | Serum |
| Collected | 20 Jun 2026, 12:38 |
| Reported | 21 Jun 2026, 06:25 |
| Test Package | Aarogyam C Pro Package |
| Method | Immunoturbidimetry (Fully Automated Latex Agglutination - Beckman Coulter) |
Test Result
| Test | Value | Unit | Risk Category |
|---|---|---|---|
| hs-CRP | 2.78 | mg/L | Average Risk |
Reference Intervals (as per report)
| Range (mg/L) | Category |
|---|---|
| < 1.00 | Low Risk |
| 1.00 - 3.00 | Average Risk ← Patient is here |
| 3.00 - 10.00 | High Risk |
| > 10.00 | Possibly Non-Cardiac Inflammation |
Interpretation
1. Where Does 2.78 mg/L Fall?
The result is in the "Average Risk" zone, but importantly it sits at the very upper edge - just 0.22 mg/L below the High Risk threshold. This is clinically significant and warrants attention.
Per the AHA/CDC Joint Committee classification (the universally accepted standard):
- < 1 mg/L = Low cardiovascular risk
- 1-3 mg/L = Intermediate/Average risk
- > 3 mg/L = High cardiovascular risk
- The 2019 ACC/AHA Primary Prevention Guideline additionally designates hs-CRP ≥ 2.0 mg/L as an "ASCVD risk enhancer" - a finding that should prompt closer attention and possible therapeutic decisions.
At 2.78 mg/L, this patient exceeds the 2.0 mg/L risk-enhancer threshold set by AHA/ACC.
2. Is This Expected for a 19-Year-Old Female?
No. In healthy young adults, hs-CRP is typically < 1 mg/L. A value of 2.78 mg/L is above normal for her age, even though it technically falls within the "average risk" band of the lab's adult reference range.
This does not mean she has cardiovascular disease. At 19, atherosclerosis is very unlikely. But an elevated hs-CRP at this age almost always indicates underlying low-grade systemic inflammation that needs to be identified and addressed.
3. What Could Cause This Elevation?
The most likely causes in a 19-year-old female, in order of probability:
| Cause | Why It Matters |
|---|---|
| PCOS (Polycystic Ovarian Syndrome) | Most common endocrine disorder in women of this age; causes chronic low-grade inflammation; hs-CRP is often elevated |
| Obesity / High Body Fat % | Adipose tissue secretes IL-6 and TNF-α → triggers CRP production in the liver |
| Insulin Resistance / Prediabetes | Even without frank diabetes; metabolic inflammation |
| Subclinical or recent infection | Dental infection, UTI, upper respiratory infection - CRP rises even in mild infections |
| Oral Contraceptive Pill (OCP) use | Oestrogen-containing pills are known to raise CRP |
| Autoimmune conditions | Subclinical SLE, thyroiditis, early rheumatoid arthritis |
| Sedentary lifestyle + poor diet | Processed foods, high sugar intake, lack of exercise - all raise CRP |
| Smoking | Even passive exposure |
| Chronic psychological stress | Elevates inflammatory cytokines |
| Anaemia | Triggers compensatory inflammatory responses |
4. What Does This Mean for Cardiovascular Risk?
The graph from Robbins Pathology (based on the Framingham Heart Study) clearly shows that hs-CRP adds independent risk information at every level of traditional cardiovascular risk:
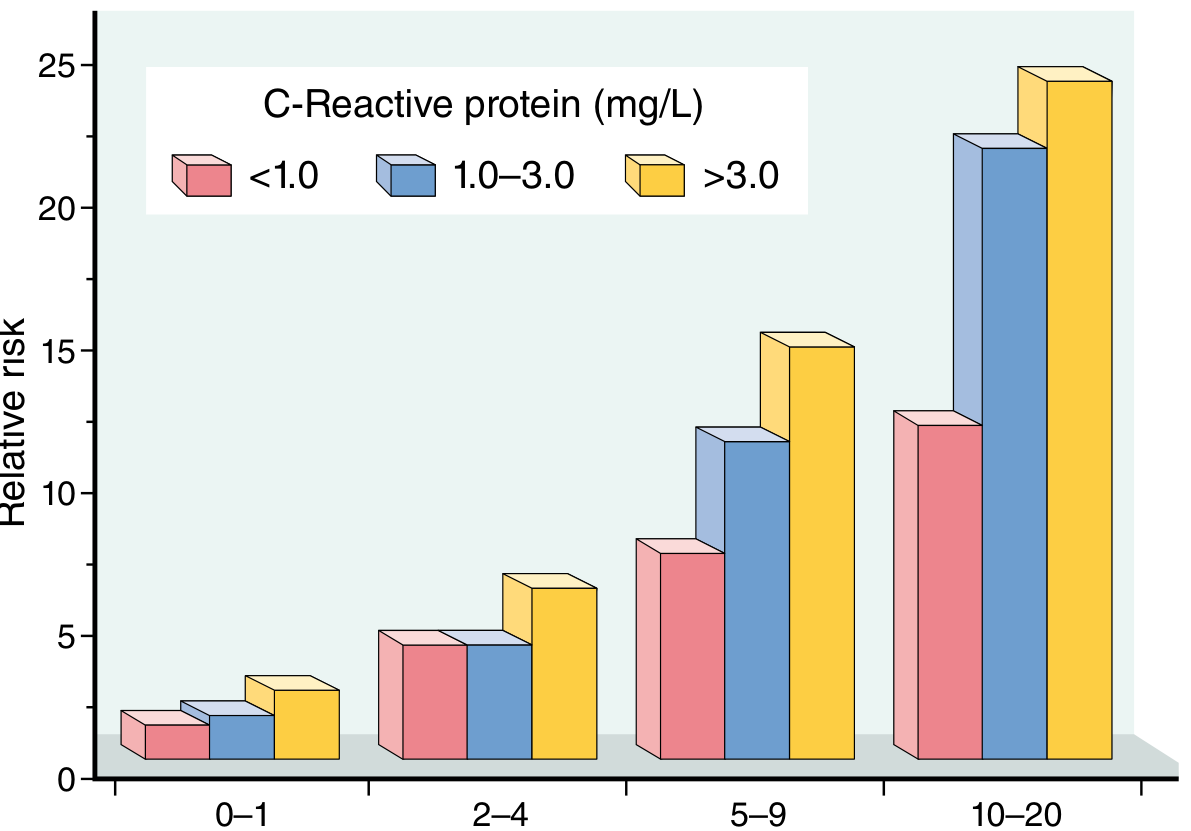
Patients with hs-CRP > 3 mg/L (yellow bars) consistently have higher relative cardiovascular risk at every Framingham risk level compared to those with hs-CRP < 1 mg/L (pink bars).
However, at age 19, absolute cardiovascular risk is very low regardless - so this finding should be used to:
- Identify reversible causes of inflammation
- Motivate early lifestyle change
- Prevent long-term risk accumulation
5. The Single-Test Limitation
The lab report itself correctly warns:
"A coronary artery disease risk assessment should be based on the average of two hs-CRP tests, ideally taken two weeks apart."
Per AHA/CDC guidelines:
- A single result can be affected by transient factors (recent illness, physical exertion, menstrual phase)
- If hs-CRP > 10 mg/L: discard, look for acute cause, repeat in 2 weeks
- For values in the 1-3 mg/L range: confirm with a second test 2 weeks later before drawing conclusions
This single result of 2.78 mg/L should be confirmed with a repeat test in 2 weeks.
Recommended Action Plan
Step 1: Repeat the Test
- Repeat hs-CRP in 2 weeks under resting, non-infected conditions
- Avoid testing during menstruation, after exercise, or if unwell
Step 2: Additional Investigations (Correlate Clinically)
| Test | Purpose |
|---|---|
| Fasting blood glucose + HbA1c | Insulin resistance, prediabetes |
| Fasting lipid profile | Overall cardiovascular risk when combined with hs-CRP |
| CBC with differential | Subclinical infection, anaemia |
| ESR | General inflammation marker |
| TSH, T3, T4 | Thyroid disease (common in young females) |
| ANA, anti-dsDNA | Screen for autoimmune disease (SLE) if symptoms suggest |
| Urine routine | Subclinical UTI |
| Pelvic ultrasound + hormonal panel (LH, FSH, testosterone) | PCOS evaluation |
| BMI, waist circumference | Metabolic risk assessment |
Step 3: Lifestyle Modifications (Evidence-Based - Lower hs-CRP)
| Intervention | Expected Effect on hs-CRP |
|---|---|
| Regular aerobic exercise (150 min/week) | Reduces hs-CRP by up to 30% |
| Mediterranean-style diet (whole grains, fish, olive oil, vegetables) | Reduces inflammation significantly |
| Weight loss if BMI > 23 (Indian cut-off) | Even 5-10% weight reduction lowers hs-CRP |
| Quit smoking / avoid passive smoke | Reduces chronic vascular inflammation |
| Adequate sleep (7-8 hours/night) | Chronic sleep deprivation raises CRP |
| Stress reduction (yoga, mindfulness) | Lowers inflammatory cytokines |
| Reduce refined carbohydrates and sugar | Reduces metabolic inflammation |
Summary
| Aspect | Assessment |
|---|---|
| Result | 2.78 mg/L - Average Risk (approaching High Risk boundary) |
| Abnormal for age? | Yes - elevated for a healthy 19-year-old |
| Immediate cardiac concern? | Low - atherosclerotic disease unlikely at 19 |
| Underlying inflammation? | Yes - needs investigation |
| Most likely causes | PCOS, obesity, insulin resistance, subclinical infection, OCP, lifestyle factors |
| Action required | Repeat test in 2 weeks + investigate underlying cause + lifestyle change |
| Long-term significance | Persistent elevation increases future cardiovascular risk - address now while young |
Overall clinical message: This result is a yellow flag, not a red flag. It should not cause panic, but it should not be ignored either. At 19 years, this is an excellent opportunity to identify and correct the underlying cause before it becomes a long-term health issue. A consultation with a physician for clinical correlation and targeted investigations is recommended.
Sources: Henry's Clinical Diagnosis and Management by Laboratory Methods, 24th Edition | Tietz Textbook of Laboratory Medicine, 7th Edition | Robbins, Cotran & Kumar Pathologic Basis of Disease, 10th Edition | AHA/CDC Joint Committee Recommendations on hs-CRP Testing
This is a shared conversation. Sign in to Orris to start your own chat.