Causes of hypothyroidism symptoms and treatment Harrison textbook
Reading File
Finding Sources
Finding Sources
Searching PubMed
hypothyroidism treatment levothyroxine
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the material needed for a comprehensive answer. Let me compile it.
Hypothyroidism - Harrison's Principles of Internal Medicine, 22nd Edition (2025)
Chapter 395 - Weetman, Mandel & Jameson
Causes of Hypothyroidism
Primary Hypothyroidism (TABLE 395-1)
Iodine deficiency remains the most common cause worldwide. In iodine-sufficient areas, the leading causes are autoimmune disease and iatrogenic factors.
Autoimmune (most common in iodine-sufficient regions):
- Hashimoto's thyroiditis (goitrous form)
- Atrophic thyroiditis (end-stage autoimmune destruction)
Iatrogenic:
- Radioiodine (¹³¹I) treatment for hyperthyroidism
- Subtotal or total thyroidectomy
- External neck irradiation (for lymphoma or cancer)
Drugs:
- Iodine excess (including iodine-containing contrast media)
- Amiodarone
- Lithium
- Antithyroid drugs
- p-aminosalicylic acid
- Interferon-α and other cytokines
- Aminoglutethimide
- Tyrosine kinase inhibitors (e.g., sunitinib)
- Immune checkpoint inhibitors (e.g., ipilimumab, nivolumab, pembrolizumab)
Congenital hypothyroidism (~1 in 2000-4000 newborns):
- Thyroid dysgenesis (65%)
- Inborn errors of thyroid hormone synthesis/dyshormonogenesis (30%)
- TSH-R antibody-mediated (5%)
Infiltrative disorders: amyloidosis, sarcoidosis, hemochromatosis, scleroderma, cystinosis, Riedel's thyroiditis
Other: Iodine deficiency, overexpression of type 3 deiodinase in infantile hemangioma and other tumors
Transient causes:
- Silent thyroiditis (including postpartum thyroiditis)
- Subacute thyroiditis
- Withdrawal of thyroxine treatment in a euthyroid patient
- After ¹³¹I treatment or subtotal thyroidectomy for Graves' disease
Central (Secondary/Tertiary) Hypothyroidism:
- Pituitary or hypothalamic disease causing TSH or TRH deficiency
Pathogenesis of Autoimmune Hypothyroidism
The autoimmune process involves marked lymphocytic infiltration (CD8+ cytotoxic T cells predominate), local cytokine production (TNF, IL-1, IFN-γ), and complement-mediated cytotoxicity. TSH-receptor blocking antibodies are found in a minority. Genetic risk factors include HLA-DR3, DR4, DR5 and polymorphisms in PTPN22 and CTLA-4. Associated autoimmune conditions include type 1 diabetes, Addison's disease, pernicious anemia, and vitiligo. High iodine intake, low selenium, and early childhood hygiene ("hygiene hypothesis") increase risk.
Clinical Features / Symptoms (TABLE 395-3)
Onset is typically insidious - patients may not notice symptoms until euthyroidism is restored.
Skin and Appendages:
- Dry skin, decreased sweating, thinning of epidermis
- Nonpitting myxedema (due to glycosaminoglycan accumulation)
- Puffy face with edematous eyelids, pretibial nonpitting edema
- Pallor with yellow tinge (carotene accumulation)
- Dry, brittle hair; diffuse alopecia; thinning of outer third of eyebrows
- Retarded nail growth
Metabolic/GI:
- Weight gain (modest, mainly fluid retention)
- Constipation
- Poor appetite
Cardiovascular:
- Bradycardia, reduced stroke volume
- Diastolic hypertension (increased peripheral resistance)
- Pericardial effusion (up to 30% of patients)
- Cool extremities (blood diverted from skin)
Neurological/Psychiatric:
- Fatigue, lethargy, slow thinking
- Depression, dementia (in severe/prolonged cases)
- Cerebellar ataxia, peripheral neuropathy
- Delayed deep tendon reflexes ("hung-up" reflexes)
- Carpal tunnel syndrome
Respiratory:
- Dyspnea (pleural effusion, impaired respiratory muscles, sleep apnea)
Reproductive:
- Oligomenorrhea, amenorrhea, or menorrhagia (early stage)
- Decreased libido, infertility, increased miscarriage risk
- Elevated prolactin - may cause galactorrhea
Other:
- Conductive or sensorineural deafness
- Anemia (normocytic or macrocytic)
- Elevated creatine phosphokinase, cholesterol, triglycerides
In children: slow growth, delayed facial/dental maturation, myopathy with muscle swelling, delayed puberty (or rarely precocious puberty).
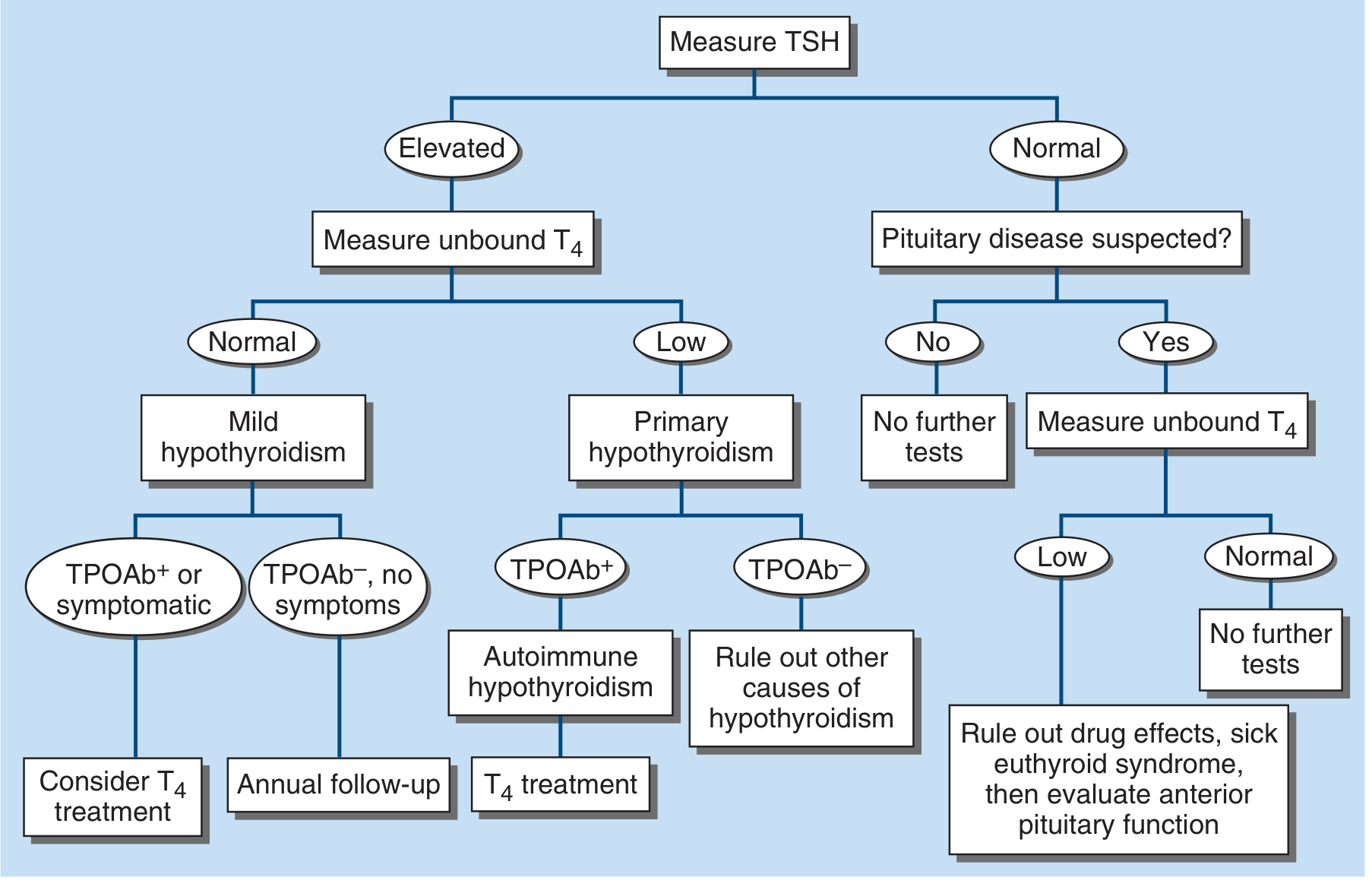
Laboratory Evaluation
- TSH is the best screening test; elevated TSH confirms primary hypothyroidism
- Free T4 (FT4) confirms clinical hypothyroidism when TSH is elevated
- Free T3 is normal in ~25% - not indicated for diagnosis
- TPO and thyroglobulin (Tg) antibodies present in >95% of autoimmune hypothyroidism
- Other findings: elevated CK, elevated cholesterol/triglycerides, normocytic or macrocytic anemia
Diagnostic Algorithm (Figure 395-2)
Treatment
Clinical (Overt) Hypothyroidism
- Standard replacement: Levothyroxine (LT4) 1.6 μg/kg body weight/day (typically 100-150 μg/day), taken at least 30 minutes before breakfast
- After Graves' disease treatment, autonomous residual function often means lower doses needed (typically 75-125 μg/day)
- Starting dose in adults under 60 without cardiac disease: 50-100 μg/day
- Goal: TSH in the normal range, ideally the lower half of the reference range
- Recheck TSH 6-8 weeks after starting or changing dose
- Adjust in 12.5-25 μg increments (upward if TSH high; downward if TSH suppressed)
- Clinical relief may take several months even after TSH normalizes
- Once stable: annual TSH monitoring
Causes of increased LT4 requirements to consider:
- Poor adherence (most common with TSH >normal on ≥200 μg/day)
- Malabsorption (celiac disease, post-bowel surgery, H. pylori gastritis)
- Oral estrogens or SERMs
- Drug interactions reducing T4 absorption/metabolism: bile acid sequestrants, ferrous sulfate, calcium carbonate, proton pump inhibitors
Note on combination therapy: About 10-15% of patients have persistent symptoms despite normal TSH on LT4. Desiccated thyroid extract (USP) is not recommended (non-physiologic T3:T4 ratio). LT4 + liothyronine (T3) combination benefit has not been confirmed in prospective studies; T3 monotherapy is not appropriate long-term due to short half-life and fluctuating levels.
Subclinical Hypothyroidism
LT4 is recommended when:
- TSH >10 mIU/L
- Patient is pregnant or wishes to conceive
Annual monitoring is appropriate for most other patients. A treatment trial may be considered in young/middle-aged symptomatic patients or those with cardiovascular risk. Confirm TSH elevation is sustained over 3 months before treating. Starting dose: LT4 25-50 μg/day.
Special Populations
Elderly: Require ~20% less thyroxine. In elderly with coronary artery disease, start LT4 12.5-25 μg/day with increments every 2-3 months.
Pregnancy:
- Confirm thyroid function immediately after pregnancy is confirmed
- Monitor every 4 weeks during the first half of pregnancy; every 6-8 weeks after 20 weeks
- Target TSH <2.5 mIU/L (lower half of trimester-specific range)
- LT4 dose increases ~45% in athyroic women; less in Hashimoto's with residual function
- As soon as pregnancy is confirmed: increase from once-daily to 9 doses per week
- Return to pre-pregnancy dose after delivery
- Separate LT4 from prenatal vitamins and iron supplements
Myxedema Coma
A severe, life-threatening emergency with 20-40% mortality despite treatment.
Triggers: sedatives, anesthetics, antidepressants, pneumonia, heart failure, MI, GI bleeding, stroke, sepsis, cold exposure
Treatment:
- IV LT4: 200-400 μg bolus (loading dose), then 1.6 μg/kg/day IV (reduced 25% vs oral)
- Consider adding IV or NG liothyronine: loading dose 5-20 μg, then 2.5-10 μg every 8 hours
- IV hydrocortisone 50 mg every 6 hours (impaired adrenal reserve)
- Ventilatory support; glucose/hypertonic saline if hyponatremia/hypoglycemia
- Broad-spectrum antibiotics (pending exclusion of infection)
- Passive rewarming only (active external warming only if temp <30°C - risk of cardiovascular collapse)
- Avoid sedatives; reduce all medication doses (impaired drug metabolism)
Recent Evidence Note
A 2026 meta-analysis (PMID: 40579157) in J Clin Endocrinol Metab found that liothyronine-containing regimens are associated with reduced risk of dementia and mortality - this may eventually influence guidelines on combination therapy. A 2025 network meta-analysis (PMID: 39290156) reviewed patient treatment preferences. These are emerging data and do not yet supersede Harrison's recommendation that LT4 monotherapy remains the standard of care.
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025, McGraw Hill Medical), Chapter 395, pp. 3072-3075.
This is a shared conversation. Sign in to Orris to start your own chat.