Explain chapter 14 from Scott brown volume 1 allergy mechanism similarly like previous chapter
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed to write a thorough, chapter-style explanation. Here is the full breakdown of Chapter 14 from Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Volume 1.
Chapter 14 - Allergy: Basic Mechanisms
Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1
Introduction
Allergy is defined as a hypersensitivity reaction initiated by specific immunologic mechanisms. More precisely, it describes objectively reproducible symptoms or signs triggered by exposure to a defined stimulus at a dose that normal (non-atopic) persons tolerate without reaction.
Two terms to distinguish upfront:
- Hypersensitivity = an altered immune response to an antigen that causes tissue damage
- Allergy = the disease manifestation of sensitization (not everyone who is sensitized becomes symptomatic)
An allergen is an antigen - usually a protein - that causes allergic disease. Inhaled allergens (pollen, house dust mite, mould spores, pet dander, cockroach) are the main drivers of allergic airway diseases like rhinitis.
Atopy is the tendency to become sensitized and produce allergen-specific IgE (sIgE) in response to ordinary everyday exposures. It is confirmed clinically by positive skin prick tests and/or raised serum sIgE to one or more allergens.
Aetiology of Sensitization
Type I (IgE-mediated) hypersensitivity only occurs in a sensitized individual. Sensitization is multifactorial, involving:
Host (Genetic) Factors
Up to 40% of people in industrialized countries carry atopic tendency. An atopic person typically has:
- Elevated total IgE
- Strong family history of allergic disease
- Increased susceptibility to allergic rhinitis, asthma, and atopic dermatitis
Key genetic loci associated with allergic disease include:
- Chromosome 11q12-13 - encodes the beta subunit of the high-affinity IgE receptor (FcεRI)
- Chromosome 5 - encodes Th2-promoting cytokines (IL-4, IL-13), the TIM gene family (regulates Th1/Th2 balance), the p40 subunit of IL-12, and the β2 adrenergic receptor
Polymorphisms in the IL-4 gene receptor (chromosome 16p12) and the FcεRI β subunit are also implicated.
Environmental Factors
- Allergen exposure (dose and duration)
- Air pollution (diesel exhaust, SO₂, ozone)
- Hygiene hypothesis: reduced exposure to infections in early childhood (due to improved sanitation, antibiotics, smaller family size) may shift the immune balance toward Th2 responses, predisposing to allergy
- Route of sensitization: respiratory sensitization is more likely to produce airway disease
Basic Mechanisms - The Four Types of Hypersensitivity
Allergic and autoimmune disorders share similar mechanisms of tissue damage. These are organized into four types of hypersensitivity (Coombs and Gell Classification):
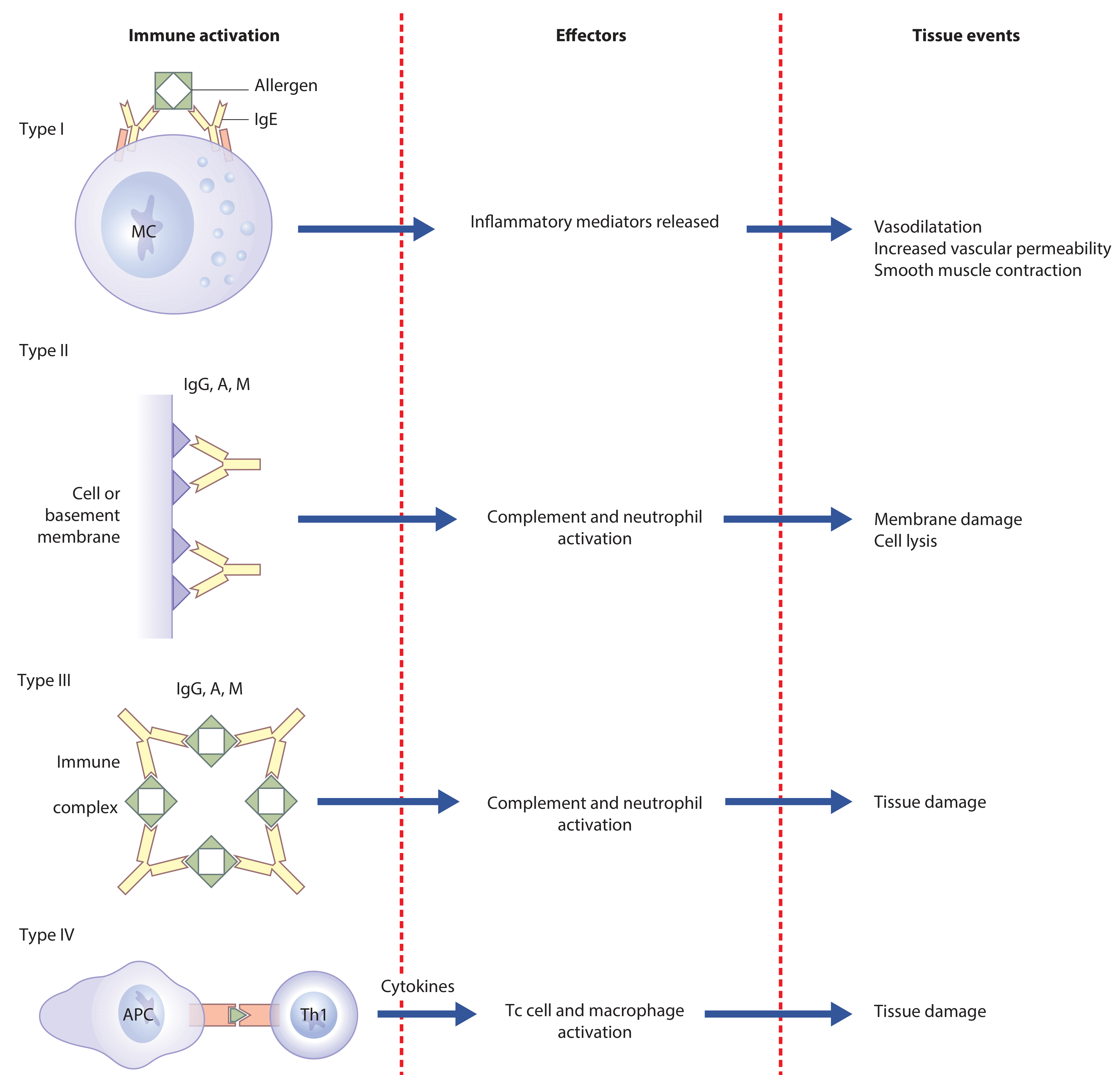
| Type | Name | Mechanism | Effector | Tissue Effect |
|---|---|---|---|---|
| I | Immediate / Reaginic | Allergen cross-links IgE on mast cells | IgE + Mast cell | Vasodilatation, increased permeability, smooth muscle contraction |
| II | Cytotoxic | Antibody (IgG/IgA/IgM) binds cell surface or basement membrane | Complement + Neutrophils | Membrane damage, cell lysis |
| III | Immune complex | Ag-Ab complexes deposit in tissues | Complement + Neutrophils | Tissue damage |
| IV | Cell-mediated (Delayed) | T cells + macrophages; no antibody | Cytokines (IL-2, IFN-γ) activating Tc cells + macrophages | Tissue damage |
In allergic rhinitis and asthma, all four types can be involved at different phases. Chronic allergic inflammation is essentially a Type IV pattern in nature.
Phase Responses in Allergy
Immediate Phase (0-60 minutes)
- Allergen cross-links IgE already bound to FcεRI on mast cells and basophils
- Degranulation releases preformed mediators (histamine, tryptase, heparin)
- Rapid synthesis of lipid mediators (prostaglandins, leukotrienes, PAF)
- Clinical result: sneezing, itch, rhinorrhoea within minutes
Late Phase Response (2-24 hours)
- Involves Th2 cytokines (IL-4, IL-5, IL-13)
- Activation and recruitment of eosinophils and other leucocytes
- Nasal blockage predominates
Chronic Allergic Inflammation
- Characterized by tissue destruction and remodelling
- Driven by persistent eosinophilic infiltration and Th2 skewing
- This phase is essentially Type IV (cell-mediated) hypersensitivity in nature
Effector Cells of Allergic Disease
Mast Cells
Mast cells are haemopoietic stem cell derivatives that mature locally in tissues. They reside near body surfaces exposed to allergens (mucosal mast cells and tissue mast cells), often close to blood vessels.
- Express FcεRI (high-affinity IgE receptor) - tightly binds sIgE even at very low serum concentrations
- Also express FcεRII (CD23) - low affinity IgE receptor; exact role in allergy not fully understood
- Granules contain preformed mediators responsible for immediate symptoms
On allergen exposure → allergen cross-links FcεRI-bound IgE → intracellular signalling → degranulation
Basophils
- Develop from bone marrow granulocyte-monocyte progenitors (unlike mast cells)
- Respond to multiple stimuli: cytokines, antibodies, proteases, antigens
- Cross-linking of IgE-bound FcεRI on basophils produces mediators similar to mast cells
- Found in nasal washes of allergic rhinitis patients - their role is increasingly recognized
Eosinophils
- Recruited by IL-5 and eotaxin
- Express FcεRI at low levels
- Release major basic protein (MBP), eosinophil peroxidase, eosinophil-derived neurotoxin
- Responsible for late-phase mucosal damage and remodelling
Dendritic Cells (DCs)
- Professional antigen presenting cells that capture allergen in the mucosa
- Migrate to draining lymph nodes to present allergen peptides to naive T cells
- Myeloid DCs induce Th2 differentiation (pro-allergic)
- Plasmacytoid DCs (CD123+) increase dramatically after repeated allergen challenge and can also induce Th2 development in vitro
- DC recruitment to bronchial mucosa occurs within the time frame of late asthmatic responses
IgE: Central Mediator of Allergy
IgE is the lowest concentration immunoglobulin in human serum (approximately 100-400 ng/mL). Most IgE is tissue-bound (half-life ~2 days in circulation but months when bound to FcεRI on mast cells).
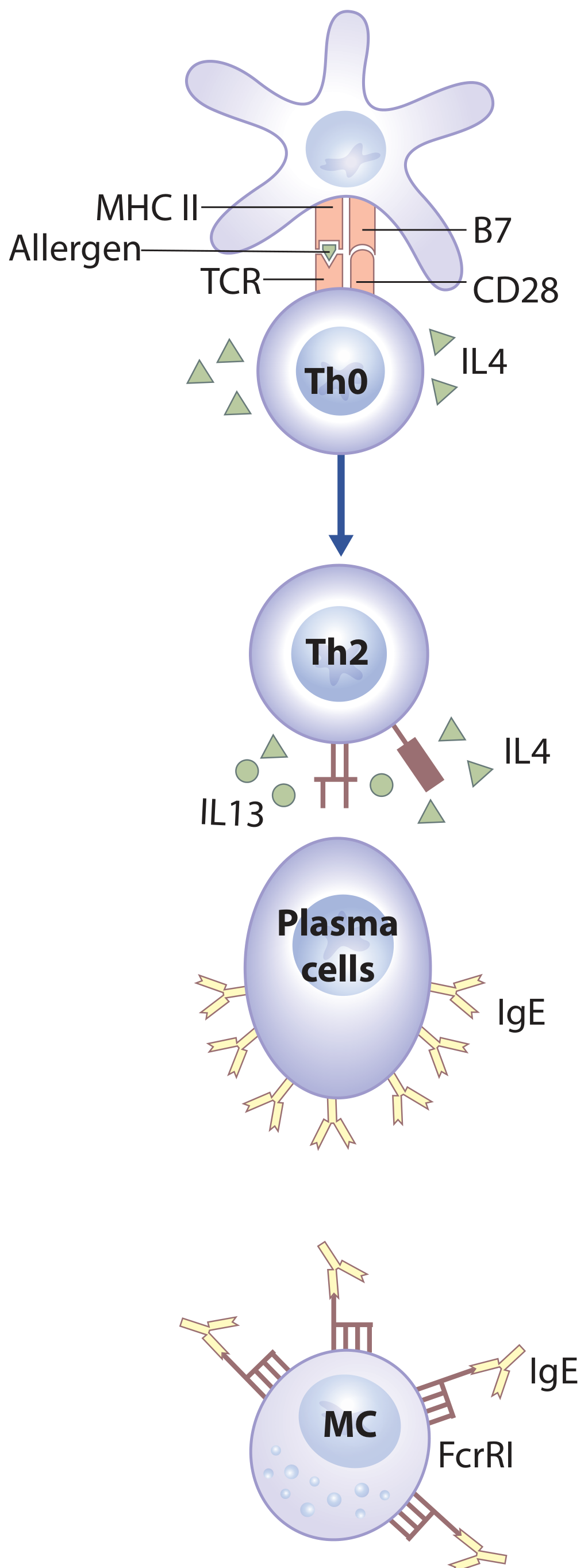
How IgE Is Produced:
- Allergen is taken up by a dendritic cell (APC) and presented via MHC II to a naive Th0 cell via TCR, with co-stimulation through B7-CD28
- In the presence of IL-4 (from the local environment), Th0 differentiates into Th2 cells
- Th2 cells secrete IL-4 and IL-13, which drive B cell isotype switching from IgM → IgE
- Plasma cells secrete IgE
- IgE binds to FcεRI on mast cells - the cell is now sensitized and ready to react on next allergen exposure
IgE production occurs mainly in bone marrow and draining regional lymph nodes, but local IgE production has been reported in some forms of allergic rhinitis (see Local Allergic Rhinitis below).
Key cytokines in IgE production:
- IL-4 and IL-13 (from Th2 cells) - promote IgE class switching
- IL-4 and IL-13 are also released from mast cells during degranulation, creating a positive feedback loop perpetuating IgE production
High-Affinity Receptor (FcεRI) Signalling in Allergic Reaction
This is the core molecular event in Type I hypersensitivity:
- Sensitization phase: IgE (specific to an allergen) binds to FcεRI on the mast cell surface - the cell is now "primed"
- Re-exposure: The same allergen enters the tissue and cross-links two or more adjacent FcεRI-IgE complexes
- Cross-linking triggers intracellular signalling:
- Activation of tyrosine kinases (Lyn, Syk)
- Phospholipase C activation → IP3 and DAG → calcium mobilization
- Activation of protein kinase C
- This results in:
- Degranulation - release of preformed granule mediators (histamine, tryptase, chymase, heparin, carboxypeptidase A)
- Rapid synthesis of lipid mediators (prostaglandins via COX pathway; leukotrienes via lipoxygenase pathway; PAF)
- Later transcription and production of cytokines (TNF-α, IL-4, IL-13, IL-5) for late phase responses
Key Mediators and Their Actions
| Mediator | Source | Action |
|---|---|---|
| Histamine | Mast cell/basophil granules | Vasodilatation, increased vascular permeability, smooth muscle contraction, pruritus |
| Tryptase | Mast cell granules | Tissue destruction; marker of mast cell activation (elevated in 60% of anaphylaxis) |
| Chymase | Mast cell granules | Connective tissue remodelling |
| Leukotrienes (LTC4, LTD4) | Rapidly synthesized | Potent bronchoconstriction, increased mucus secretion |
| Prostaglandins (PGD2) | Rapidly synthesized | Vasodilation, mucus secretion |
| PAF (Platelet Activating Factor) | Mast cells, eosinophils | Elevated in 100% of anaphylaxis; platelet activation, bronchoconstriction |
| IL-4, IL-13 | Mast cells, Th2 cells | Amplify Th2 response, promote IgE production |
| IL-5 | Th2 cells | Eosinophil activation and survival |
| TNF-α | Mast cells | Promotes inflammation |
| Eosinophil Major Basic Protein (MBP) | Eosinophils | Toxic to parasites and epithelium; triggers histamine release from mast cells |
Histamine note: Highly soluble and rapidly diffuses - metabolized within minutes by histamine N-methyl transferase, monoamine oxidase, and diamine oxidase. Its short half-life limits its use as a laboratory marker (unlike tryptase).
Role of Sensory Nerves in Allergic Rhinitis
Neurogenic mechanisms amplify allergic inflammation:
- Mast cell mediators directly activate sensory nerve endings in nasal mucosa
- Activated sensory nerves release neuropeptides - Substance P and neurokinin
- These neuropeptides further promote vasodilation, glandular secretion, and inflammatory cell recruitment (neurogenic inflammation)
- Neurogenic inflammation is self-perpetuating - an important component of the allergen-IgE interaction
- Nerve growth factor (NGF) is detectable in nasal fluid in chronic allergic rhinitis and increases after allergen challenge
- Hyper-responsiveness of target organs (nasal mucosa) relates to a combination of chronic inflammation AND increased sensory nerve activation
Local Allergic Rhinitis (LAR)
A clinically important concept: Local Allergic Rhinitis (LAR) describes a localized nasal allergic response occurring in patients who:
- Have negative systemic skin prick tests
- Have normal serum sIgE
- Yet mount a genuine IgE-mediated local mucosal allergic response to allergens
This is explained by local IgE synthesis within the nasal mucosa itself, rather than systemic sensitization. LAR may explain why some sensitized individuals develop rhinitis while others develop asthma or eczema, and why others have sensitization with no clinical manifestation.
Clinical Features of IgE-Mediated Hypersensitivity
Lifetime prevalence of anaphylaxis is estimated at 0.05-2.0%. The clinical manifestations reflect mediator effects across multiple systems:
| System | Manifestations |
|---|---|
| Prodromal | Anxiety, paraesthetic sensations on palms and soles |
| Cutaneous | Pruritus, flushing, urticaria, angioedema |
| Respiratory | Rhinorrhoea, sneezing, bronchospasm, laryngeal oedema |
| Cardiovascular | Hypotension, tachycardia, arrhythmias (T-wave inversion, SVT, bundle branch block), myocardial infarction |
| Gastrointestinal | Nausea, vomiting, abdominal cramps, diarrhoea |
- IV allergen (e.g. drug) → anaphylaxis within seconds
- General immediate allergy → within 60 minutes of allergen exposure
- Biphasic reactions → immediate + late phase reactions occurring together
Post-mortem in fatal anaphylaxis typically shows: airway oedema, laryngeal oedema, pulmonary hyperinflation, pulmonary oedema, eosinophilic infiltration around bronchi, and swelling of liver/spleen/intestine.
Key Points Summary
| Concept | Key Fact |
|---|---|
| Allergy definition | Hypersensitivity reaction via specific immunologic mechanisms |
| Atopy prevalence | Up to 40% in industrialized countries |
| Main IgE receptor | FcεRI (high affinity) on mast cells, basophils, eosinophils |
| IgE concentration | Lowest of all immunoglobulin isotypes (100-400 ng/mL) |
| Key cytokines for IgE switching | IL-4 and IL-13 (from Th2 cells) |
| Immediate mediator | Histamine - metabolized within minutes |
| Best anaphylaxis marker | PAF elevated in 100%; tryptase in 60%; histamine in 70% |
| Neurogenic amplification | Substance P and neurokinin from sensory nerves |
| Local Allergic Rhinitis | Local IgE production without systemic sensitization |
Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1, Chapter 14 - pp. 137-148
This is a shared conversation. Sign in to Orris to start your own chat.