Operative Surgery: Stomach, Colon, Appendix, MAS ( Incl postop complications)
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a comprehensive, exam-ready note on Operative Surgery: Stomach, Colon, Appendix, MAS, and Postoperative Complications.
Operative Surgery: Stomach, Colon, Appendix & Minimally Access Surgery (MAS)
I. OPERATIVE SURGERY OF THE STOMACH
A. Gastrectomy-Based Procedures
1. Billroth I (Gastroduodenostomy)
- Lower half of the stomach is resected; cut stomach anastomosed to the first part of the duodenum
- Standard operation for gastric ulcer (ulcer excised to exclude malignancy)
- Preferred reconstruction after partial gastrectomy for distal gastric cancer
2. Billroth II / Pólya (Gastrojejunostomy)
- Two-thirds of the stomach removed; duodenal stump closed; stomach anastomosed to jejunum
- Removes the gastric antrum → reduces acid load
- Diverts gastric secretions away from duodenum (Pólya)
- Still occasionally needed for complex emergency ulcer disease (e.g., giant perforated duodenal ulcer where Billroth I anastomosis under tension)
- No longer has an elective role for duodenal ulceration
3. Total Gastrectomy (for Gastric Cancer)
-
Approach: Long upper midline incision
-
Stomach removed en bloc with entire greater and lesser omentum
-
Steps:
- Transverse colon separated from greater omentum
- Subpyloric nodes dissected; duodenum divided with surgical stapler
- Hepatic nodes cleared along hepatic artery; right gastric artery divided at origin
- Left gastric artery divided at origin; nodes along splenic artery removed
- Spleen preserved if possible; oesophagus divided with right-angled clamp (>5 cm clearance from tumour)
- Frozen section of resection margins if in doubt
-
Reconstruction: Roux-en-Y oesophagojejunostomy
- Alimentary (Roux) limb ≥ 50 cm to prevent bile reflux oesophagitis
- Circular stapler used via purse-string in oesophageal stump
- End-to-side jejunojejunostomy at a convenient point
-
Lymph node dissection:
- D1: Perigastric nodes (N1 stations)
- D2: Major arterial trunks cleared — standard at specialist centres, spleen and pancreas conserved, station 10 nodes spared
4. Subtotal Gastrectomy (Distal Tumours)
- Proximal stomach preserved; blood supply from short gastric arteries
- Reconstruction: Roux-en-Y jejunogastrostomy preferred over Billroth II (less enterogastric reflux and bile reflux oesophagitis)
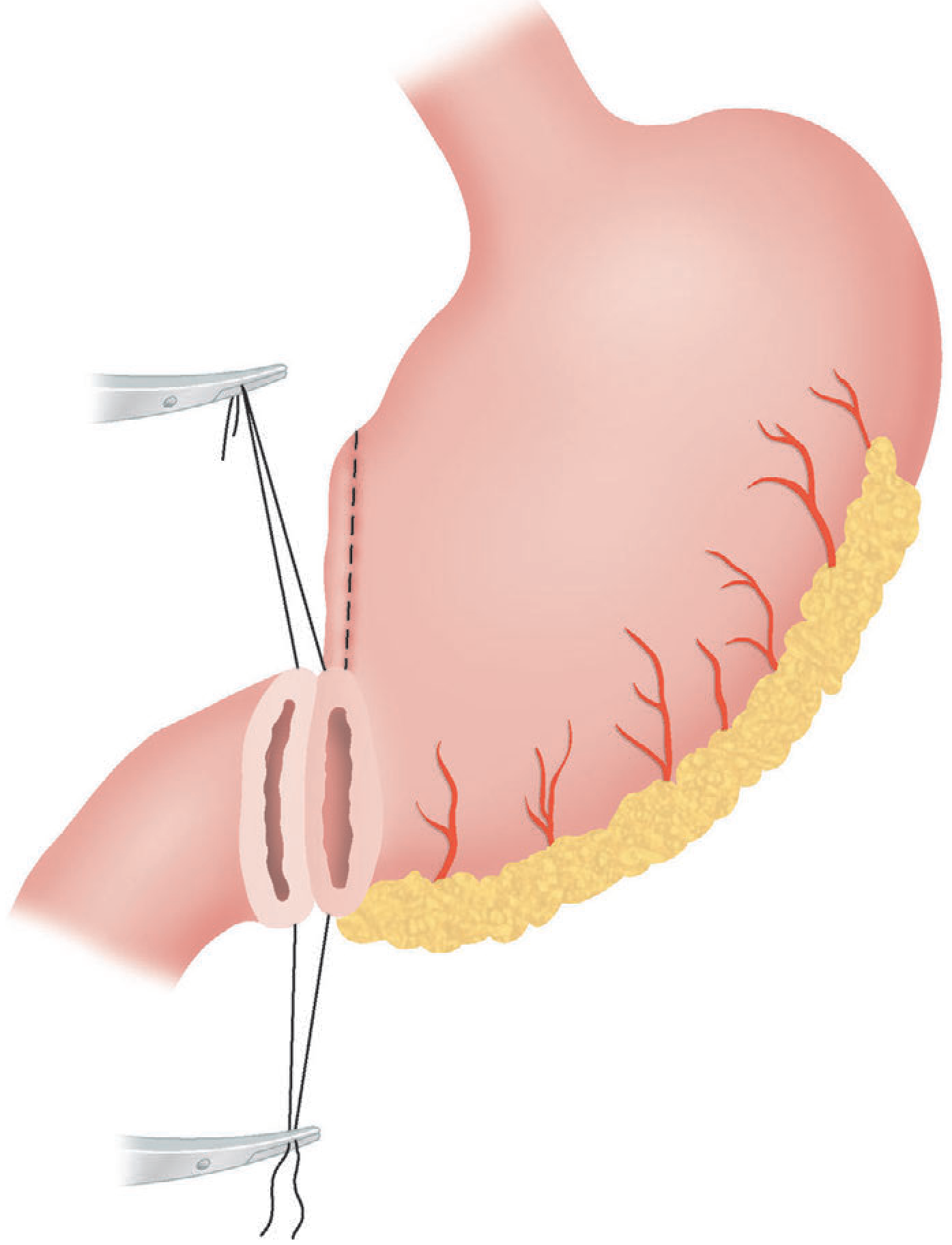
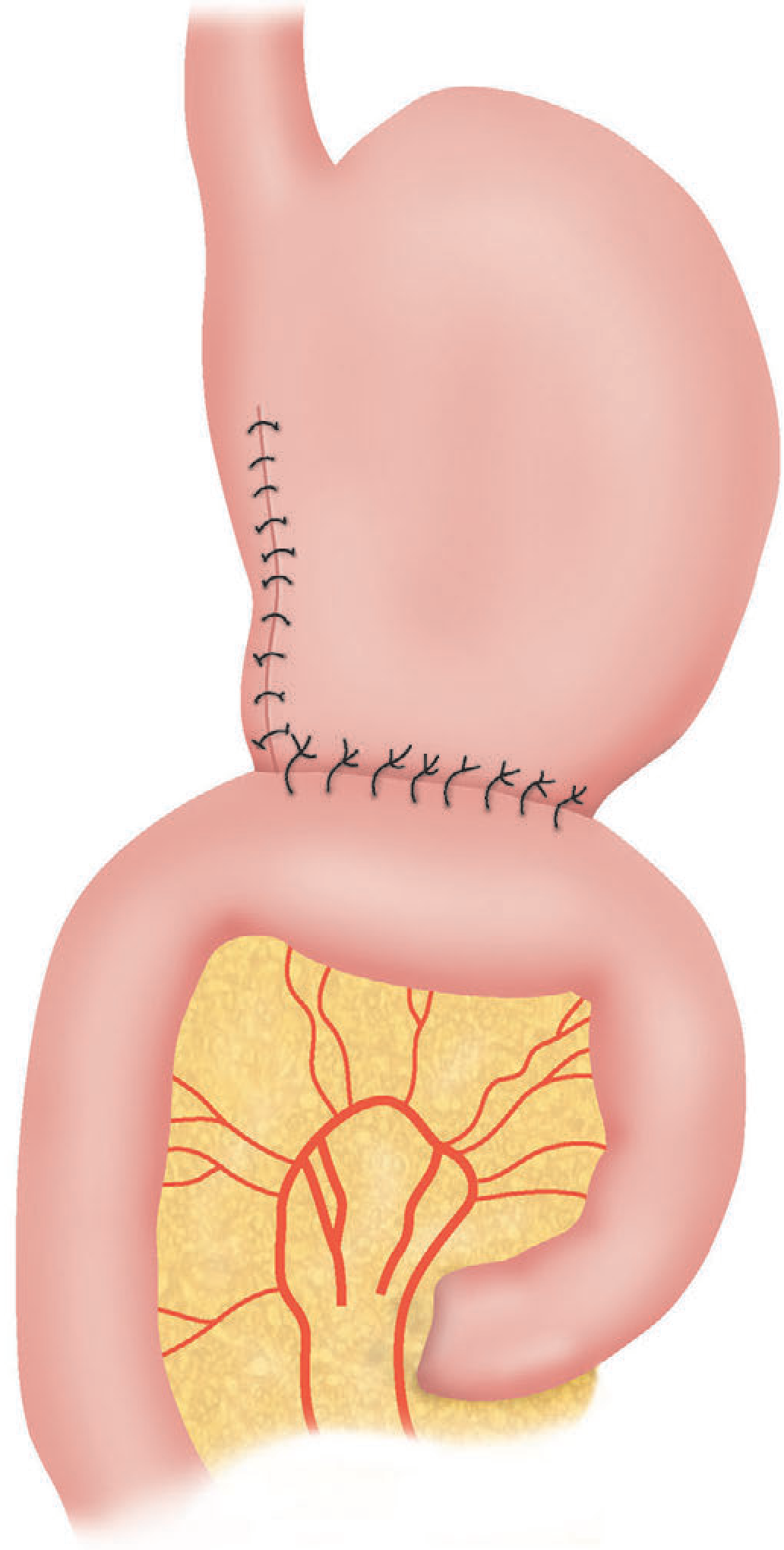
5. Gastrojejunostomy (Bypass)
- Jejunum anastomosed to posterior, dependent wall of antrum — isoperistaltic
- Used for bypass of malignant obstruction (distal stomach, duodenum, pancreatic tumours)
- Poor results when used for duodenal ulcer alone (→ stomal ulceration from acid exposure)
B. Vagotomy-Based Procedures
1. Truncal Vagotomy + Drainage
- Principle: Section of vagus at lower oesophagus → reduces maximal acid output by ~50%
- Gastric drainage procedure needed due to gastric stasis (vagal denervation of antropyloroduodenal segment)
- Drainage options:
- Heineke–Mikulicz pyloroplasty (most popular): longitudinal incision through pylorus closed transversely
- Gastrojejunostomy: alternative drainage
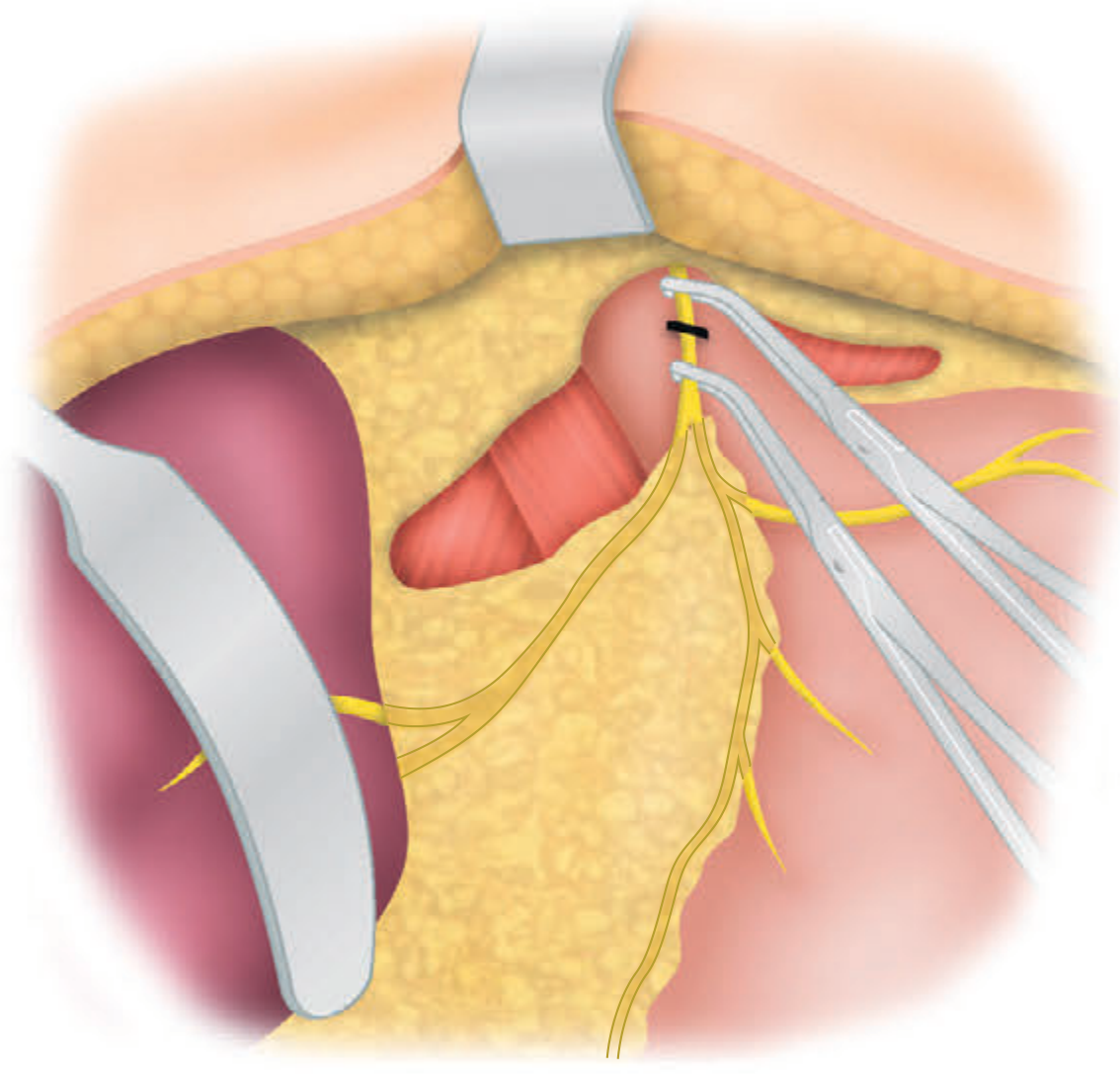
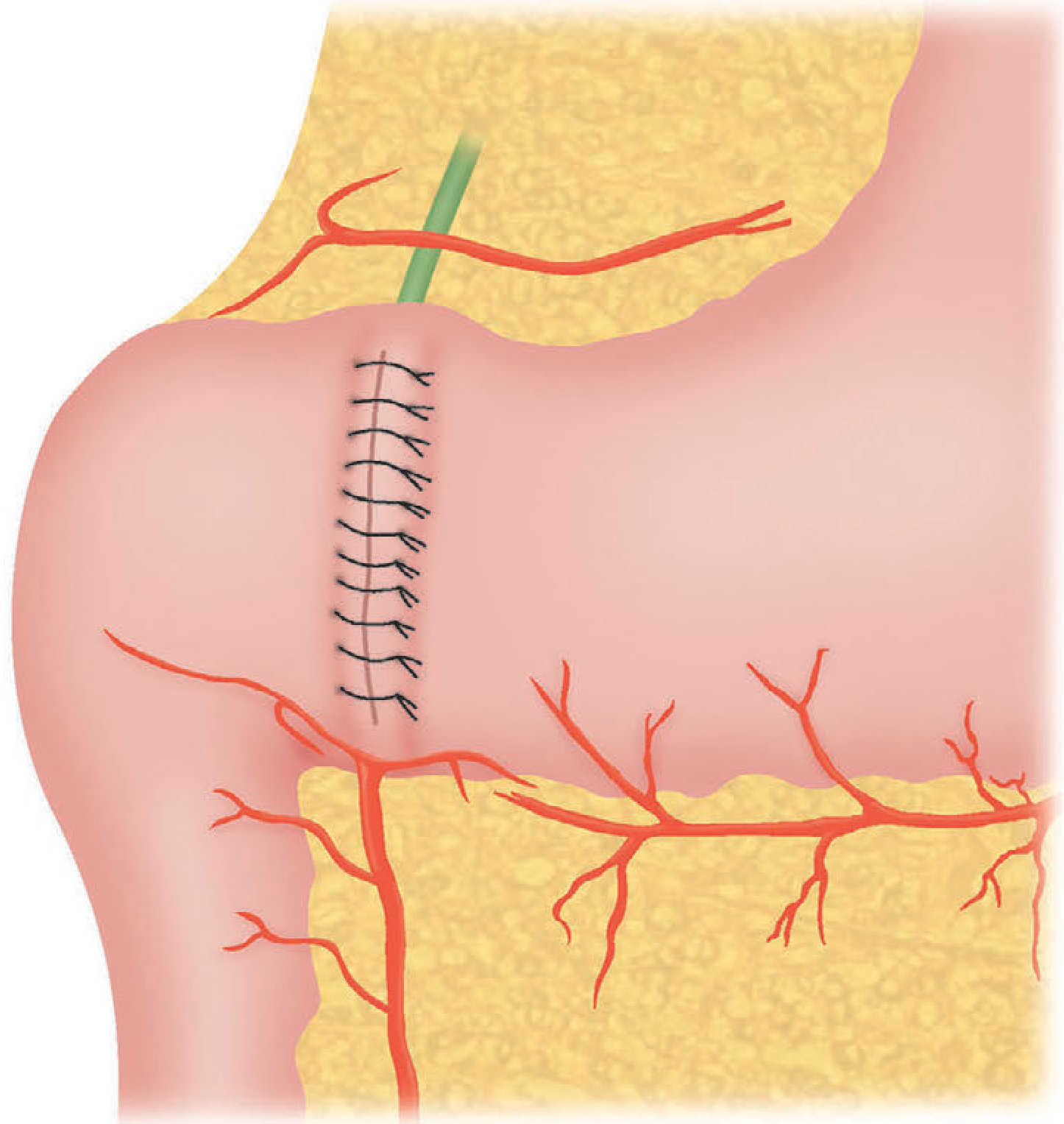
2. Highly Selective Vagotomy (HSV) / Parietal Cell Vagotomy
- Only the parietal cell mass is denervated; nerves to antrum (crow's foot of Latarjet) preserved
- No drainage procedure required (antropyloroduodenal innervation preserved)
- Lowest operative mortality (<0.2%), lowest side effects (<5%), but higher recurrence (2–10%)
- Does NOT increase risk of long-term gastric cancer (unlike other operations)
3. Selective Vagotomy + Drainage
- Vagotomy of the gastric branches only (preserving hepatic and coeliac fibres)
- Similar side effects to truncal vagotomy
Comparison Table (Bailey & Love, p. 1183)
| Operation | Operative mortality | Significant side effects | Recurrent ulceration |
|---|---|---|---|
| Gastrectomy | 1–2% | 20–40% | 1–4% |
| Gastroenterostomy alone | <1% | 10–20% | 50% |
| Truncal vagotomy + drainage | <1% | 10–20% | 2–7% |
| Selective vagotomy + drainage | <1% | 10–20% | 5–10% |
| Highly selective vagotomy | <0.2% | <5% | 2–10% |
| Truncal vagotomy + antrectomy | 1% | 10–20% | 1% |
II. POSTOPERATIVE COMPLICATIONS OF GASTRIC SURGERY
~30% of patients suffer some degree of dysfunction; ~5% have intractable symptoms.
A. Early Complications (Post-Radical Gastrectomy)
- Oesophagojejunal anastomotic leak — mainly saliva and food; often managed conservatively (Roux-en-Y limits contamination); drain placement if fistula develops
- Duodenal stump leakage — usually due to distal obstruction; drained radiologically → controlled fistula; Foley catheter placed in duodenum to establish controlled fistula if bile peritonitis requires laparotomy
- Secondary haemorrhage — septic collections + vascular dissection → catastrophic bleeding from exposed vessels; managed by re-operation or interventional radiology
B. Sequelae / Long-Term Complications
1. Dumping Syndrome
| Feature | Early Dumping | Late Dumping |
|---|---|---|
| Incidence | 5–10% | 5% |
| Timing | Almost immediate after meal | 1–2 hours after meal |
| Duration | 30–40 min | 30–40 min |
| Relief | Lying down | Food |
| Aggravated by | More food | Exercise |
| Precipitant | Carbohydrate-rich, wet food | Same |
| Symptoms | Epigastric fullness, sweating, light-headedness, tachycardia, colic, diarrhoea | Tremor, faintness, prostration |
| Mechanism | Hyperosmolar load → fluid sequestration into gut → circulatory effects | Rapid gastric emptying → hyperglycaemia → reactive hypoglycaemia |
| Treatment | Small fat/protein meals; avoid high-carbohydrate fluids; octreotide | Same; octreotide very effective |
2. Postvagotomy Diarrhoea
- Most devastating sequela; ~5% intractable
- Cause: rapid gastric emptying + denervation + exaggerated GI peptide response
- Management: dietary manipulation, antidiarrhoeals; octreotide NOT effective; revisional surgery results unpredictable
3. Bilious Vomiting / Bile Reflux Gastritis
- Follows operations diverting alkaline bile into gastric remnant
- Treatment: Roux-en-Y reconstruction (≥50 cm limb); first choice revisional surgery after Billroth I
4. Small Stomach Syndrome
- Reduced capacity → early satiety; managed with frequent small meals
5. Recurrent Ulceration & Gastrocolic Fistula
- Anastomotic ulcer at gastrojejunostomy penetrates transverse colon
- Presents with: profuse post-prandial diarrhoea, foul breath, faeculent vomiting, severe weight loss
- Diagnosis: CT with oral contrast, barium enema; endoscopy often non-diagnostic
- Caused largely by jejunal bacterial contamination, not direct colonic communication
6. Malignant Transformation
- Partial gastrectomy and vagotomy + drainage are independent risk factors for gastric cancer (bile reflux → intestinal metaplasia)
- Lag phase: minimum 10 years
- HSV not associated with increased cancer risk
7. Nutritional Consequences
- Weight loss common; vitamin B12 deficiency (loss of parietal cell mass/intrinsic factor) — requires routine replacement
- Other deficiencies: iron (poor absorption), folate, fat-soluble vitamins
- Advice: small, frequent meals; jejunum/small gastric remnant adapts over time
III. OPERATIVE SURGERY OF THE COLON
A. Total Abdominal Colectomy (TAC)
Indications:
-
2 colonic segments involved with rectal sparing, where anastomosis is unsafe
- Patient in extremis with pancolitis (where total proctocolectomy not indicated)
- Indeterminate colitis (Crohn's vs. UC not established)
Laparoscopic TAC Technique:
- Begin with ileocolic pedicle division; mobilise caecum off right iliac vessels (medial to lateral)
- Continue clockwise to hepatic flexure; divide gastrocolic ligament
- Splenic flexure: antegrade (right to left) preferred; retrograde if severely inflamed
- Caution: arc of Riolan / IMV branches; avoid splenic capsule injury
- Left colon: divide lateral attachments; protect left ureter (stents if severe inflammation)
- Medial approach to sigmoid / left colon avoids inflammatory adhesions
- Distal transection: rectosigmoid junction — preserves adequate rectal length
- Extract through Pfannenstiel or ileostomy site incision
- End ileostomy or ileorectal anastomosis depending on clinical scenario
Key Note: For malignancy, vascular ligation at origin required; for IBD, ligation can be closer to colon (mesentery often friable and thickened).
B. Right Hemicolectomy / Colectomy for Colon Cancer
- Medial-to-lateral dissection; high vascular ligation at origin of feeding vessels (ileocolic, right colic, middle colic)
- Duodenum protected during hepatic flexure mobilisation
- Ileocolic anastomosis (hand-sewn or stapled, end-to-end, end-to-side or side-to-side)
C. Colostomy / Ileostomy
- Stoma may be definitive, covering/diverting, or salvage
- Slow-transit constipation: ileostomy preferred over colostomy as definitive procedure
- If ileostomy output is unsatisfactorily high → avoid colectomy
IV. OPERATIVE SURGERY OF THE APPENDIX
A. Laparoscopic Appendicectomy (Appendectomy)
Position: Supine; left arm fixed; Foley catheter considered
Access:
- Veress needle technique or Hasson open technique through umbilicus
- CO₂ insufflation to 12–15 mmHg
- Umbilical camera port + working ports in RLQ/LLQ
Steps:
- Reverse Trendelenburg with right side up
- Follow caecum to convergence of taenia coli to locate appendix base
- Retrocaecal appendix: divide white line of Toldt to mobilise caecum
- Create window through mesoappendix; divide with linear stapler (white load) or ligasure/cautery
- Divide appendix at base with blue load stapler or Endoloop
- Place in retrieval bag; extract through umbilical port
- Inspect staple line; achieve haemostasis
- If turbid fluid: send sample for culture and sensitivities
B. Open Appendicectomy (McBurney's Approach)
Incision: Grid-iron incision centred on McBurney's point (junction of outer and middle third of line from ASIS to umbilicus), within a natural skin crease
Layers of dissection (grid-iron/muscle-splitting):
- External oblique aponeurosis — split in direction of fibres
- Internal oblique — bluntly split
- Transversus abdominis — split
- Peritoneum — elevated and sharply incised
Steps:
- Caecum identified and delivered into wound
- Appendiceal base at convergence of taenia coli
- "Classic" technique: divide mesoappendix between Kelly clamps + ligate with 3-0 silk
- Crush appendix at base with Kelly clamp → relocate clamp 1 cm distal to crush zone (CZ)
- Ligate at CZ with 0 chromic suture; divide just proximal to clamp
- Stump: cauterise or invaginate with purse-string / Z-stitch
Closure:
- Peritoneum + transversus: running absorbable suture
- Internal + external oblique: interrupted absorbable sutures
- Skin: subcuticular absorbable suture
- If perforated: skin left open or loosely approximated
C. Management of Perforated/Complicated Appendicitis
Occurs in up to 40% of appendicitis cases
Management based on clinical picture:
| Clinical State | Management |
|---|---|
| Diffuse peritonitis, haemodynamically unstable | Resuscitate → urgent laparotomy/laparoscopy |
| Phlegmon or abscess (drainable) | IV antibiotics + percutaneous CT-guided drainage |
| Phlegmon (non-drainable) | IV antibiotics + nutritional support; interval appendicectomy |
- Antibiotic choice: Piperacillin-tazobactam alone OR ceftriaxone + metronidazole
- Once tolerating diet: oral amoxicillin/clavulanate for 5-day total course (equally effective to 7 days)
Nonoperative Management of Uncomplicated Appendicitis (Controversial):
- Antibiotics-only viable alternative; ~25% failure rate requiring appendicectomy
- Appendicectomy remains the treatment of choice
V. MINIMALLY ACCESS SURGERY (MAS)
A. Definition & Philosophy
- MIS / MAS: Major operations through small incisions using miniaturised imaging systems, minimising access trauma without compromising surgical quality
- Term "minimal access surgery" (Wickham) emphasises small incisions; "minimally invasive surgery" (MIS) is more widely used
B. Types of MAS
| Type | Key Feature |
|---|---|
| Laparoscopy | CO₂ pneumoperitoneum + port-based instruments |
| SILS (Single-Incision Laparoscopic Surgery) | All trocars at umbilicus; reduces to 1 scar |
| NOTES (Natural Orifice Transluminal Endoscopic Surgery) | Flexible endoscope through mouth/anus/vagina/urethra; scar-free |
| Robotic Surgery (da Vinci) | Computer-enhanced; tremor removal; 7 degrees of freedom; superior for urologic/colorectal/complex reconstructions |
| Hand-Assisted Laparoscopy | Hand port for difficult dissection while maintaining pneumoperitoneum |
C. Physiology of CO₂ Pneumoperitoneum
Two categories of effects:
Gas-specific effects:
- CO₂ rapidly absorbed into circulation → carbonic acid → respiratory acidosis
- Body buffers (largest reserve in bone) absorb up to 120 L CO₂
- Once buffers saturated: hypercarbia develops; anaesthesiologist must increase ventilation
- Risk of barotrauma if excessive tidal volumes used
Pressure-specific effects (intra-abdominal pressure 12–15 mmHg):
- Reduced venous return (inferior vena cava compression)
- Reduced cardiac output
- Increased systemic vascular resistance
- Caval compression → risk of DVT/PE (combined with reduced lower limb perfusion)
- Raised diaphragm → reduced FRC, atelectasis
Clinical implications:
- Hypercarbia masked by adequate ventilation
- Cardiac patients at risk of decompensation
- Pregnancy: use lowest effective pressure; second trimester safest
D. Access Techniques
Veress Needle (Closed Technique)
- Umbilical skin elevated; stab incision made
- Veress needle inserted perpendicular to skin until two clicks (fascial + peritoneal entry)
- Drop test confirms entry into peritoneal cavity
- Insufflate to 12–15 mmHg
- Insert trocar (blind or optical — Optiview / Visiport)
Hasson (Open) Technique
- Infra- or supraumbilical incision down to external oblique
- Vertical incision through fascia (elevated with retention sutures)
- Peritoneum entered bluntly; Hasson port inserted under direct vision
- Anchored with stay sutures; insufflation begun
E. Laparoscopic Advantages vs Open Surgery
| Parameter | Laparoscopic | Open |
|---|---|---|
| Pain | Less | More |
| Recovery | Faster | Slower |
| Hospital stay | Shorter | Longer |
| Wound complications | Fewer | More |
| Visualisation | Magnified (10×) | Direct |
| Port-site metastasis | Possible (cancer) | N/A |
| Cost | Higher initially | Lower |
F. Special Considerations
- Laparoscopy in pregnancy: Best performed in 2nd trimester; lowest effective intra-abdominal pressure; fetal monitoring required; left lateral tilt to avoid aorto-caval compression
- Cancer surgery: Appropriate if good tissue-handling maintained; avoid tumour morcellation; N₂O pneumoperitoneum avoided (unknown effect on port-site metastasis)
- Robotic surgery: Most valuable in urologic, gynaecologic, colorectal, and complex abdominal wall reconstruction
- Cirrhosis/Portal hypertension: Increased risk of haemorrhage; reduced pneumoperitoneum tolerance
VI. GENERAL POSTOPERATIVE COMPLICATIONS (Abdominal Surgery)
A. Early (<72 hrs)
| Complication | Timing | Key Features |
|---|---|---|
| Reactionary haemorrhage | <24 hrs | Slipped ligature; vasodilaton; management: re-exploration |
| Paralytic ileus | 2–3 days | Absent bowel sounds; abdominal distension; manage with NGT, NPO, IV fluids |
| Atelectasis/chest | 24–48 hrs | Most common early respiratory complication; treated with physiotherapy |
| Urinary retention | <24 hrs | Especially post-inguinal/pelvic/anorectal surgery |
| DVT | Any time | Virchow's triad; prophylaxis: LMWH + TED stockings |
B. Intermediate (3–10 days)
| Complication | Timing | Key Features |
|---|---|---|
| Wound infection | 5–7 days | Most common SSI; Streptococcal (<3 days); mixed organisms (5–7 days) |
| Anastomotic leak | 5–7 days | Fever, peritonism, sepsis; confirm with CT/contrast study |
| Pulmonary embolism | 7–10 days | Pleuritic chest pain, dyspnoea, tachycardia; confirm V/Q scan or CTPA |
| Intra-abdominal abscess | 7–10 days | Swinging pyrexia, ileus, leucocytosis; CT-guided drainage |
C. Late (>10 days)
| Complication | Key Features |
|---|---|
| Incisional hernia | Long-term; midline > transverse; associated with infection, obesity |
| Adhesive small bowel obstruction | Previous abdominal surgery; manage conservatively initially; obstruction persists → surgery |
| Port-site metastasis (laparoscopic) | Especially with pneumoperitoneum during cancer surgery |
| Nutritional deficiencies | After gastrectomy: B12, iron, folate, fat-soluble vitamins |
D. Specific Postoperative Complications by Operation
| Surgery | Specific Complication |
|---|---|
| Total gastrectomy | Oesophagojejunal leak; duodenal stump blow-out; vitamin B12 deficiency; dumping |
| Colectomy | Anastomotic leak; ureter injury; wound infection; ileus |
| Appendicectomy | Pelvic/subphrenic abscess (if perforated); stump appendicitis; faecal fistula |
| Vagotomy | Diarrhoea; dumping; gastric stasis; bile reflux |
| Laparoscopy | Port-site hernia; CO₂ gas embolism; visceral/vascular injury at access; subcutaneous emphysema |
Sources: Bailey and Love's Short Practice of Surgery 28th Edition, pp. 1182–1185, 1197; Current Surgical Therapy 14e; Schwartz's Principles of Surgery 11th Edition, pp. 453–475; Mulholland and Greenfield's Surgery 7e
Do surgery operation 101
Asking for Preferences
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Transplantation and Immunosuppression, AIDS & Universal precautions
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
I've exhausted my DB queries. I have sufficient foundational content from the textbooks and my core medical knowledge to now deliver a comprehensive, exam-ready note. Let me compile it all.
Transplantation, Immunosuppression, AIDS & Universal Precautions
PART I: TRANSPLANTATION
A. Definitions & Types of Grafts
| Term | Definition |
|---|---|
| Autograft | Graft from same individual (e.g., skin graft, saphenous vein CABG) |
| Isograft (Syngeneic) | Graft between genetically identical individuals (identical twins) |
| Allograft | Graft between members of the same species but different genotype (most transplants) |
| Xenograft | Graft between different species (e.g., porcine heart valves, pig-to-human) |
B. The Immunological Basis of Rejection
Major Histocompatibility Complex (MHC) / HLA System
- HLA antigens (Human Leukocyte Antigens) are the main alloantigens responsible for rejection
- Encoded on chromosome 6 (short arm)
- Class I (HLA-A, B, C): expressed on all nucleated cells; recognised by CD8+ cytotoxic T cells
- Class II (HLA-DR, DP, DQ): expressed on APCs (dendritic cells, B cells, macrophages); recognised by CD4+ helper T cells
- ABO blood group antigens: also expressed on endothelium; mismatch → hyperacute rejection
Allorecognition Pathways
| Pathway | Mechanism |
|---|---|
| Direct | Recipient T cells recognise intact donor MHC on donor APCs (early; acute rejection) |
| Indirect | Recipient APCs process donor peptides → present to recipient T cells (chronic rejection) |
| Semi-direct | Recipient T cells acquire donor MHC from donor APCs |
C. Types of Rejection
| Type | Timing | Mechanism | Histology | Treatment |
|---|---|---|---|---|
| Hyperacute | Minutes to hours | Pre-formed antibodies against ABO or HLA class I antigens → complement activation → thrombosis | Fibrin thrombi, neutrophil infiltration, haemorrhagic necrosis | None effective; organ must be removed; prevented by cross-matching |
| Accelerated Acute | 2–5 days | Reactivation of sensitised T cells (previously sensitised recipient) | Similar to acute | High-dose steroids; may reverse |
| Acute | Days to 3 months | T cell-mediated (cellular) or antibody-mediated (humoral) | Lymphocytic infiltration, tubulitis (kidney); endothelialitis | Pulse IV methylprednisolone; anti-thymocyte globulin (ATG); plasmapheresis for humoral |
| Chronic | Months to years | Indirect allorecognition; fibrosis; intimal smooth muscle proliferation | Obliterative vasculopathy; fibrosis; tubular atrophy | No effective reversal; optimise immunosuppression |
Graft-versus-Host Disease (GvHD):
- Occurs when donor immunocompetent T cells attack a relatively immunocompromised host
- Seen in: bone marrow / haematopoietic stem cell transplantation (HSCT), small bowel transplant, blood transfusion in immunocompromised
- Acute GvHD (<100 days): skin rash, diarrhoea, hepatitis
- Chronic GvHD (>100 days): resembles autoimmune disease (scleroderma-like)
- Treatment: high-dose corticosteroids, ciclosporin, mycophenolate
D. Tissue Matching / Pre-Transplant Workup
| Test | Purpose |
|---|---|
| ABO typing | Compatibility essential to prevent hyperacute rejection |
| HLA typing | Match at HLA-A, B, DR reduces rejection risk (especially renal) |
| Crossmatch | Recipient serum + donor lymphocytes → if +ve (pre-formed antibodies present) → contraindication (hyperacute rejection risk) |
| Panel Reactive Antibody (PRA) | % of panel cell population against which recipient has antibodies; high PRA = highly sensitised |
| Mixed lymphocyte reaction (MLR) | In vitro test of T cell response; used mainly in bone marrow transplant |
E. Brain Death & Organ Donation
Brain Death Criteria (UK/most guidelines):
- Irreversible structural brain damage from known cause
- No sedatives/metabolic cause
- Tests performed by 2 senior doctors on 2 separate occasions:
- Absent brainstem reflexes (pupillary, corneal, oculovestibular/caloric, gag, cough, oculocephalic)
- Apnoea test: PaCO₂ rises to ≥6.65 kPa with no respiratory effort
Types of donors:
- DBD (Donation after Brain Death): heart-beating donor; optimal oxygenation of organs
- DCD (Donation after Circulatory Death): controlled (Maastricht III) or uncontrolled; higher rates of primary non-function (ischaemia)
Cold Ischaemia Times (approximate maximums):
| Organ | Maximum Cold Ischaemia Time |
|---|---|
| Heart | 4–6 hours |
| Lung | 6–8 hours |
| Liver | 12–24 hours |
| Pancreas | 12–18 hours |
| Kidney | 24–36 hours |
| Small bowel | 8–12 hours |
F. Individual Organ Transplants
1. Renal Transplantation
- Most common solid organ transplant
- Recipient's native kidneys NOT removed (unless symptomatic - hypertension, recurrent infection, polycystic disease)
- Site: Heterotopic - iliac fossa (extraperitoneal)
- Anastomoses: Renal artery to external iliac artery; renal vein to external iliac vein; ureter to bladder (ureteroneocystostomy)
- Early complications: acute tubular necrosis (ATN), acute rejection, renal artery thrombosis, ureteric obstruction/fistula
- Late complications: chronic rejection, calcineurin inhibitor nephrotoxicity, opportunistic infections, post-transplant lymphoproliferative disorder (PTLD), recurrent original disease
2. Liver Transplantation
- Indications: cirrhosis (alcoholic, viral, NAFLD), acute liver failure, cholestatic disease (PBC, PSC), hepatocellular carcinoma (Milan criteria: 1 lesion ≤5 cm or 3 lesions ≤3 cm, no vascular invasion, no extrahepatic spread)
- Orthotopic (native liver removed); caval replacement or piggy-back technique
- MELD score used to prioritise allocation
- Split liver / living donor (right lobe)
- Complications: primary non-function, hepatic artery thrombosis (most feared early complication), biliary leak/stricture, acute/chronic rejection
3. Heart Transplantation
- Indications: end-stage heart failure (NYHA class IV), ischaemic/dilated cardiomyopathy, refractory arrhythmias
- Orthotopic; bicaval technique now preferred
- Denervated heart: resting HR ~100 bpm; no angina with ischaemia; relies on Frank-Starling and circulating catecholamines
- Complications: primary graft failure, acute rejection (Rx: OKT3/ATG), cardiac allograft vasculopathy (chronic rejection - obliterative coronary disease; diagnosed by annual coronary angiography), accelerated atherosclerosis
4. Lung Transplantation
- Indications: COPD, IPF, cystic fibrosis, pulmonary hypertension
- Single or bilateral sequential
- Primary graft dysfunction (reperfusion injury): most common early cause of death
- Bronchiolitis obliterans syndrome (BOS): manifestation of chronic rejection; progressive airflow obstruction; azithromycin may slow progression
5. Pancreas Transplantation
- Usually combined with kidney (SPK - simultaneous pancreas kidney)
- Indications: Type 1 diabetes with end-stage renal disease
- Exocrine drainage: bladder (older) or enteric (newer preferred)
- Monitoring rejection: serum amylase/lipase rise indicates graft pancreatitis; urinary amylase (if bladder drainage)
PART II: IMMUNOSUPPRESSION
A. Goals
- Prevent acute rejection
- Prevent chronic rejection
- Maintain adequate immune function to fight infections
- Minimise drug toxicity
B. Immunosuppressive Drugs - Mechanism & Side Effects
1. Calcineurin Inhibitors (CNIs)
| Drug | Ciclosporin (Cyclosporine) | Tacrolimus (FK506) |
|---|---|---|
| Mechanism | Binds cyclophilin → inhibits calcineurin → blocks IL-2 gene transcription → T cell suppression | Binds FKBP-12 → inhibits calcineurin → same IL-2 blockade; 10-100× more potent |
| Key toxicity | Nephrotoxicity, hypertension, hyperlipidaemia, hirsutism, gingival hyperplasia, neurotoxicity | Nephrotoxicity, neurotoxicity, diabetes mellitus (new onset), alopecia, hyperkalaemia |
| Monitoring | Trough blood levels | Trough blood levels |
| Interactions | CYP3A4 substrate: azole antifungals ↑ levels; rifampicin ↓ levels | Same |
2. Antiproliferative Agents
| Drug | Azathioprine | Mycophenolate Mofetil (MMF) |
|---|---|---|
| Mechanism | Purine analogue → inhibits DNA synthesis in rapidly dividing cells (T & B cells) | Inhibits inosine monophosphate dehydrogenase (IMPDH) → blocks de novo purine synthesis → selective T and B cell inhibition |
| Key toxicity | Bone marrow suppression, hepatotoxicity; do NOT use with allopurinol (xanthine oxidase inhibition → azathioprine toxicity) | GI upset, diarrhoea, bone marrow suppression; teratogenic |
| Use | Being replaced by MMF | Preferred antiproliferative today |
3. mTOR Inhibitors
| Drug | Sirolimus (Rapamycin) | Everolimus |
|---|---|---|
| Mechanism | Binds FKBP-12 → inhibits mTOR → blocks IL-2-driven T cell proliferation (G1→S phase block) | Same |
| Key toxicity | Hyperlipidaemia, mouth ulcers, impaired wound healing, pneumonitis, not nephrotoxic | Same |
| Advantage | CNI-sparing (useful in CNI nephrotoxicity); anti-proliferative (reduces PTLD, HCC recurrence) | Same |
4. Corticosteroids
- Mechanism: Broad anti-inflammatory and immunosuppressive; inhibit NF-κB, reduce cytokine production (IL-1, IL-2, IL-6, TNF-α), impair APC function
- Uses: Maintenance (low dose prednisolone), acute rejection (IV methylprednisolone 500 mg–1 g/day × 3 days)
- Side effects: Diabetes, osteoporosis, hypertension, weight gain, adrenal suppression, cataracts, avascular necrosis of hip, poor wound healing, susceptibility to infection
5. Biological Agents
| Agent | Class | Mechanism | Use |
|---|---|---|---|
| Basiliximab | Anti-CD25 mAb (IL-2R blocker) | Blocks IL-2 receptor on T cells | Induction immunosuppression |
| ATG (Anti-thymocyte globulin) | Polyclonal antibody | Depletes T cells | Induction; acute steroid-resistant rejection |
| Rituximab | Anti-CD20 mAb | Depletes B cells | Antibody-mediated rejection |
| Belatacept | CTLA4-Ig fusion protein | Blocks CD28-B7 co-stimulation | CNI-free maintenance |
| OKT3 (Muromonab) | Anti-CD3 mAb | Depletes/inactivates T cells | Steroid-resistant rejection (largely replaced) |
| Eculizumab | Anti-C5 mAb | Blocks complement activation | Antibody-mediated rejection; thrombotic microangiopathy |
6. Standard Triple Therapy Protocol
CNI + Antiproliferative + Corticosteroide.g., Tacrolimus + MMF + Prednisolone
Induction: Basiliximab or ATG at time of transplant
Maintenance: taper steroids over time; CNI doses reduced per trough levels
C. Complications of Immunosuppression
| Complication | Details |
|---|---|
| Opportunistic infections | CMV (most common; Rx ganciclovir), PCP (Pneumocystis jirovecii; Rx co-trimoxazole prophylaxis), candida, aspergillus, TB reactivation, BK virus nephropathy (renal transplant) |
| Malignancy | 3× increased cancer risk; PTLD (EBV-driven B-cell lymphoma), skin cancers (SCC > BCC - reversed from general population), Kaposi sarcoma, cervical/anal cancer (HPV-driven) |
| Cardiovascular disease | Accelerated atherosclerosis; hypertension (CNIs); hyperlipidaemia |
| Metabolic | NODAT (New Onset Diabetes After Transplant; tacrolimus > ciclosporin); osteoporosis (steroids) |
| Drug nephrotoxicity | CNI nephrotoxicity → chronic allograft nephropathy |
PART III: AIDS IN SURGICAL CONTEXT
A. Pathophysiology Review
- HIV (Human Immunodeficiency Virus) - RNA retrovirus; predominantly HIV-1
- Targets CD4+ T cells (also macrophages, dendritic cells) via gp120-CD4 binding + co-receptor (CCR5 or CXCR4)
- Reverse transcriptase converts RNA → DNA → integrates into host genome
- Progressive CD4+ depletion → AIDS when CD4 count <200 cells/μL (or AIDS-defining illness)
B. AIDS-Defining Conditions (Surgical Relevance)
| Category | Examples |
|---|---|
| Opportunistic infections | PCP, CMV retinitis/colitis, MAC, toxoplasmosis, cryptococcal meningitis, oesophageal candidiasis |
| AIDS-defining malignancies | Kaposi sarcoma, CNS lymphoma, invasive cervical cancer |
| Anorectal disease | Anal condylomata (HPV), anal SCC (HPV-16), anal fissure, anal ulcers (primary HIV), perianal abscess/fistula |
| GI disease | CMV colitis (bloody diarrhoea), HIV enteropathy, cryptosporidiosis |
C. Surgical Considerations in HIV/AIDS Patients
Pre-operative assessment:
- CD4 count and viral load (guide surgical risk)
- Full medication history (ARTs, interactions)
- CD4 >200/μL: most elective surgery safe
- CD4 <50/μL: high perioperative risk; consider deferring elective surgery
Surgical complications more common in HIV/AIDS:
- Poor wound healing
- Higher rates of infection (including resistant organisms)
- Higher recurrence of anorectal conditions
- Increased risk of post-op opportunistic infections
- Drug interactions between ARTs and anaesthetic agents
Common surgical indications in HIV:
- Anorectal surgery (most common): condylomata, fissures, abscesses, fistulae
- Surgery not significantly different but expect impaired healing and higher recurrence
- Splenomegaly/hypersplenism: splenectomy may be required
- Kaposi sarcoma: intestinal (bleeding, obstruction, perforation)
- Lymphoma: abdominal (obstruction, perforation, staging)
- CMV colitis: perforation → emergency surgery (high mortality)
PART IV: UNIVERSAL PRECAUTIONS
A. Definition
Universal Precautions (introduced by the CDC, 1987) - the principle that all blood and body fluids from every patient should be treated as potentially infectious for HIV, HBV, HCV and other bloodborne pathogens, regardless of the patient's known or presumed infection status.
Expanded to "Standard Precautions" (1996) - includes blood, all body fluids, secretions, excretions (except sweat), non-intact skin, and mucous membranes.
B. Components of Standard/Universal Precautions
| Precaution | Detail |
|---|---|
| Hand hygiene | Most important single measure; soap + water or alcohol gel before and after patient contact |
| Gloves | When touching blood, body fluids, mucous membranes, non-intact skin |
| Mask + eye protection | When there is a risk of splashing blood/body fluids |
| Gown/apron | When clothing may be contaminated |
| Safe sharps handling | Never re-sheath needles by hand; use sharps bin immediately; use blunt needles where possible |
| Safe waste disposal | Yellow bags (clinical waste), sharps containers, pharmaceutical waste |
| Decontamination | Instruments: cleaning → disinfection → sterilisation (autoclave 134°C for prions) |
C. Bloodborne Pathogen Risks to Healthcare Workers
| Pathogen | Risk per Needlestick | Prevention | Post-Exposure Prophylaxis |
|---|---|---|---|
| HBV | 6–30% | Hepatitis B vaccination (3 doses) | HBIG + vaccine booster within 48 hrs |
| HCV | 0.5–2% (1.8% average) | No vaccine | No proven PEP; monitor LFTs + HCV RNA; treat if seroconversion (SOF-based DAAs) |
| HIV | 0.3% (percutaneous); 0.09% (mucous membrane) | No vaccine; ARV PEP | PEP within 1 hour (ideally) and no later than 72 hours; 28-day course |
HIV Risk by route of exposure:
- Needlestick: 0.3%
- Mucous membrane splash: 0.09%
- Intact skin: negligible
- Risk increased by: hollow bore needle, deep puncture, visible blood on device, terminal illness in source patient (high viral load)
D. Post-Exposure Protocol (Needlestick)
IMMEDIATE actions:
- Encourage bleeding from wound; wash thoroughly with soap and water (do NOT suck wound)
- Splash to eyes/mouth: irrigate copiously with water
- Report immediately to occupational health / A&E
- Risk-assess the source patient (HIV, HBV, HCV status; consent for urgent testing)
- Assess baseline serology of exposed worker (HIV, HBV, HCV)
If HIV risk (source HIV+ve or unknown high-risk):
- Start PEP within 1 hour, no later than 72 hrs
- Standard PEP regimen: Truvada (tenofovir + emtricitabine) + raltegravir (or dolutegravir) × 28 days
- Follow-up HIV test at 6 weeks and 3 months
If HBV risk:
- If worker vaccinated and known responder → no action needed
- If unvaccinated or non-responder: HBIG + vaccine within 48 hours
E. Additional Precaution Categories (Beyond Standard)
| Category | Indications | Additional Measures |
|---|---|---|
| Contact precautions | MRSA, VRE, C. difficile, scabies, wound infections | Gloves + gown for all contact; dedicated equipment |
| Droplet precautions | Influenza, meningococcal disease, mumps, pertussis | Surgical mask within 1 metre; single room if possible |
| Airborne precautions | TB, measles, chickenpox, COVID-19 (aerosolised) | FFP3 respirator, negative pressure room, HEPA filtration |
F. Surgical Team Protection - Theatre Precautions
| Risk | Precaution |
|---|---|
| Sharps injury | No-touch technique for passing sharps; "neutral zone" on instrument trolley; blunt suture needles for fascia closure |
| Blood splash | Double gloving (reduces needlestick by 25%), face shields/visor |
| Bone fragments | Eye protection during orthopaedic / thoracic procedures |
| Electrocautery aerosol/plume | Smoke evacuators; N95 masks during laparoscopy (especially HPV/HIV patients) |
| High-risk list patients | HIV, HBV, HCV → no change in standard precautions; same care for all; Universal Precautions apply to ALL patients regardless |
G. Sterilisation & Disinfection
| Level | Method | Kills | Used for |
|---|---|---|---|
| Sterilisation | Autoclave (steam, 121°C/134°C), ethylene oxide gas, gamma radiation | All organisms including spores and prions (134°C) | Surgical instruments, implants |
| High-level disinfection | Glutaraldehyde, peracetic acid, chlorine dioxide | All except prions | Endoscopes |
| Intermediate disinfection | 70% alcohol, chlorhexidine + alcohol | Bacteria, most viruses, mycobacteria | Skin prep, surfaces |
| Low-level disinfection | Quaternary ammonium compounds | Most bacteria, some viruses | General surface cleaning |
Creutzfeldt-Jakob Disease (CJD/vCJD): prion diseases require autoclave at 134°C × 18 min or 1M NaOH/sodium hypochlorite; disposable instruments used where possible for high-risk patients.
Sources: Bailey and Love's Short Practice of Surgery 28th Ed; Mulholland and Greenfield's Surgery 7e (HIV and AIDS, p. 3589); Cellular and Molecular Immunology (Abbas); Harrison's Principles of Internal Medicine 22e; Brenner & Rector's The Kidney; CDC Standard Precautions guidelines
This is a shared conversation. Sign in to Orris to start your own chat.