Hyperkalemia treatment
Reading File
Finding Sources
Searching PubMed
hyperkalemia treatment management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive overview of hyperkalemia treatment, organized by urgency.
Hyperkalemia Treatment
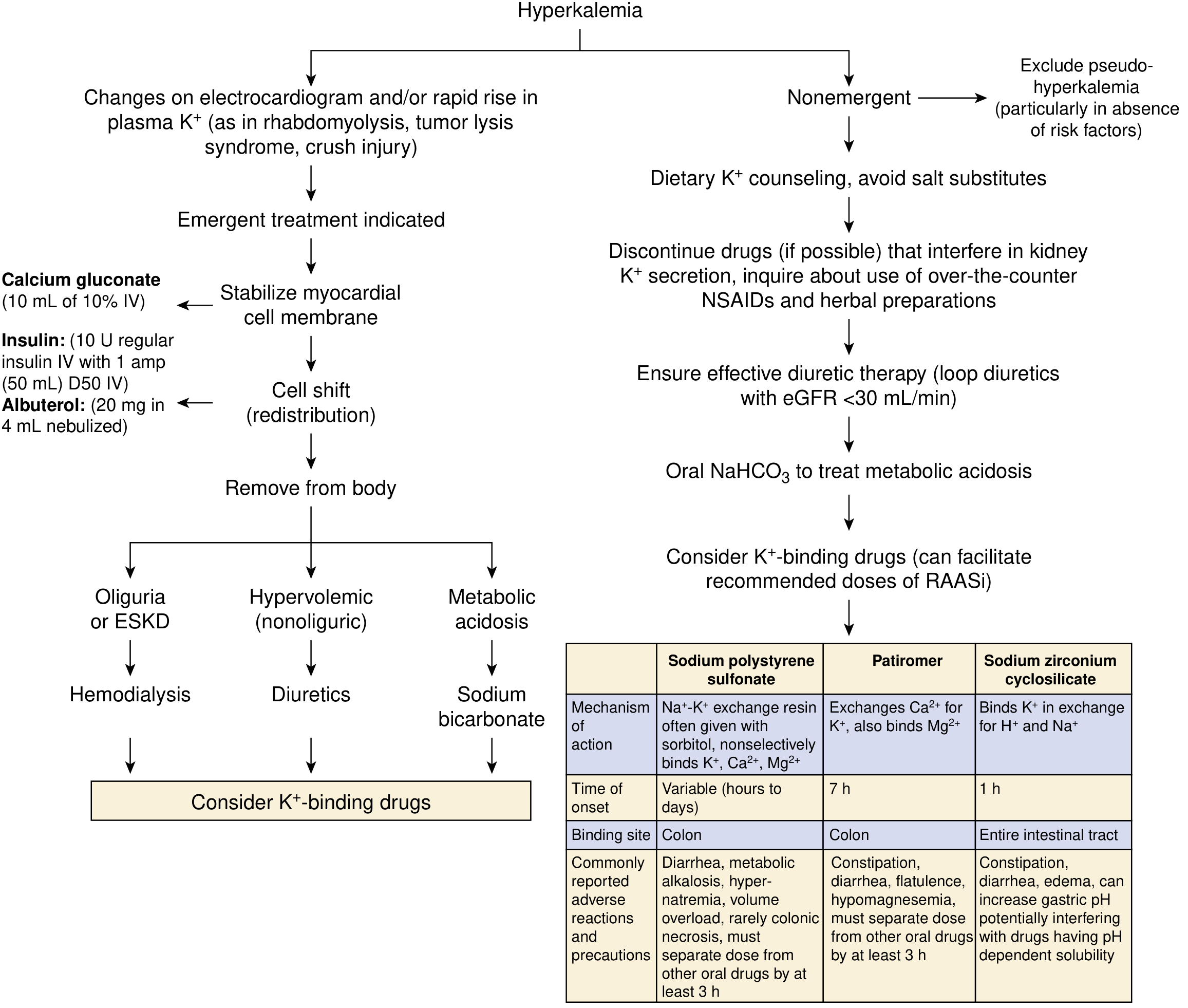
Step 1 — Stabilize the Cardiac Membrane (Emergent, if ECG changes present)
ECG changes (peaked T waves → widened QRS → loss of P wave → sine wave) at any K⁺ level constitute an emergency.
IV Calcium — does NOT lower potassium; directly antagonizes myocardial membrane excitability.
- Calcium gluconate: 10 mL of 10% solution IV over 1–3 min (preferred peripherally; safer if extravasation occurs)
- Calcium chloride: 10 mL of 10% solution over 10 min — more elemental calcium per ampule but causes skin necrosis if it infiltrates; use only via central line
- Effect is almost immediate; if no ECG improvement in 3–5 min, repeat the dose
- ⚠️ Use with caution in patients on digoxin (may precipitate toxicity)
Step 2 — Shift K⁺ into Cells (Temporizing, 15–60 min onset)
These measures reduce plasma K⁺ temporarily (1–4 hours); they do not remove K⁺ from the body.
| Agent | Dose | Onset | Notes |
|---|---|---|---|
| Regular insulin + dextrose | 10 U IV + 50 mL D50W bolus, then D5W at 100 mL/hr | 15 min | Fastest transcellular shift; monitor glucose closely — hypoglycemia common, especially in renal failure. If glucose >300 mg/dL, may omit dextrose |
| Nebulized albuterol | 20 mg in 4 mL nebulized over 10 min | 30 min | Additive to insulin; ~30% of patients are resistant. IV albuterol (0.5 mg) available in Europe gives equivalent effect |
| Sodium bicarbonate | 50–100 mEq IV over 10–20 min | Variable | Useful only if severe metabolic acidosis (HCO₃⁻ <10 mmol/L); does NOT enhance insulin/albuterol effect; limited benefit in anuric patients |
Step 3 — Remove K⁺ from the Body
Diuretics
- Loop and thiazide diuretics are effective when adequate renal function is present.
Potassium-Binding Resins (GI excretion)
| Agent | Dose | Time of Onset | Notes |
|---|---|---|---|
| Sodium polystyrene sulfonate (SPS / Kayexalate) | 15–50 g PO in sorbitol; or 50 g retention enema | Hours to days | Rectal route faster; rarely causes colonic necrosis (FDA black-box warning when combined with sorbitol); not approved for chronic use |
| Patiromer (Veltassa) | 8.4 g PO once daily | ~7 hours | Exchanges Ca²⁺ for K⁺ in colon; approved for chronic management; separate from other oral drugs by ≥3 h; monitor Mg²⁺ |
| Sodium zirconium cyclosilicate (Lokelma) | Standard protocol | ~1 hour | Binds K⁺ in exchange for H⁺/Na⁺ throughout GI tract; 9× higher binding capacity than SPS per gram; approved for chronic management |
Hemodialysis
- Most effective method; indicated in anuric patients (severe AKI or ESKD) or when conservative measures fail.
- Rarely initiates fast enough to preclude the above emergency measures.
Non-Emergent / Chronic Management
For biochemical hyperkalemia without ECG changes:
- Dietary K⁺ restriction — avoid high-K⁺ foods, salt substitutes
- Discontinue offending drugs — ACE inhibitors, ARBs, potassium-sparing diuretics, NSAIDs, heparin, TMP-SMX
- Loop diuretics — especially if eGFR <30 mL/min
- Oral sodium bicarbonate — for concomitant metabolic acidosis
- Fludrocortisone — if mineralocorticoid deficiency (hypoaldosteronism, e.g., Type IV RTA)
- Long-term K⁺ binders (patiromer or ZS-9) — to facilitate continued use of RAASi in CKD/heart failure
Key Points
- Calcium — membrane stabilizer only; acts in seconds; repeat if no response in 3–5 min
- Insulin ± albuterol — fastest intracellular shift; always cover with dextrose
- Never give dextrose alone without insulin in insulin-deficient patients (can paradoxically worsen hyperkalemia via osmotic shift)
- Bicarbonate — limited acute role; reserve for severe acidosis (HCO₃⁻ <10)
- Dialysis — definitive therapy in renal failure
- Newer binders (patiromer, ZS-9) are preferred over Kayexalate for chronic management due to better safety profiles
— National Kidney Foundation Primer on Kidney Diseases, 8e | Schwartz's Principles of Surgery, 11e | Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.