I now have rich content from Guyton & Hall directly. Let me now deliver the complete, structured teaching session.
🏛️ GUYTON & HALL PHYSIOLOGY MASTERCLASS
SESSION 1 - TOPIC: THE CELL AND ITS FUNCTIONS
(Guyton & Hall, Chapter 2 - Unit I)
Your Professor's Opening Note: Before we memorize anything, we must understand the cell the way Guyton intended - not as a list of organelles, but as a living, intelligent factory that maintains life. Every disease you will ever treat is ultimately a cell behaving abnormally. Master the cell, and you master medicine.
━━━━━━━━━━━━━━━━━━━━
STAGE 1: BIG PICTURE
━━━━━━━━━━━━━━━━━━━━
1. Why Does the Cell Exist in the Human Body?
Think of the human body as a country. The country runs because of millions of individual citizens (cells) each doing a specific job. No citizen = country collapses. No cell = organism dies.
The cell is the smallest unit capable of life. It can:
- Take in raw materials (nutrients, oxygen)
- Generate energy (ATP)
- Build products (proteins, hormones)
- Respond to signals (receptors, messengers)
- Reproduce itself
- Maintain its internal environment
The human body contains approximately 35 to 40 trillion cells (Guyton), each adapted for a specific function, yet all sharing a common blueprint.
2. Its Role in Maintaining Homeostasis
Homeostasis = the maintenance of a stable internal environment.
Every single cell contributes to homeostasis:
Each cell maintains its OWN internal environment
↓
Billions of cells together maintain the EXTRACELLULAR FLUID
↓
The ECF is the "internal environment" of the body
↓
= HOMEOSTASIS (Claude Bernard's concept, expanded by Guyton)
If even one cell type fails (e.g., pancreatic beta cells), the whole body suffers (diabetes).
3. How It Connects to Other Systems
| System | How Cells Are the Core |
|---|
| Nervous | Neurons are specialized cells that transmit electrical signals |
| Cardiovascular | Cardiomyocytes contract; endothelial cells line vessels |
| Respiratory | Pneumocytes exchange gases; ciliated cells clear debris |
| Endocrine | Gland cells secrete hormones |
| Renal | Tubular cells reabsorb, secrete, concentrate urine |
| Immune | Lymphocytes, macrophages recognize and destroy pathogens |
| GI | Enterocytes absorb nutrients; goblet cells secrete mucus |
Key insight from Guyton: "Each tissue or organ is an aggregate of many different cells held together by intercellular supporting structures." The body is nothing but cells + their products.
4. Real-Life Importance
- Cancer = cells dividing uncontrollably (loss of cell cycle regulation)
- Diabetes Type 1 = autoimmune destruction of insulin-secreting beta cells
- Alzheimer's = neurons (brain cells) dying due to protein aggregates
- Sepsis = cell membranes failing under bacterial toxin attack
- Anemia = too few red blood cells (25 trillion normally; reduced in anemia)
Every disease = cell pathology at some level. This is why we start here.
━━━━━━━━━━━━━━━━━━━━
STAGE 2: BASIC FOUNDATION
━━━━━━━━━━━━━━━━━━━━
Definitions & Terminology
| Term | Definition |
|---|
| Cell | The structural and functional unit of life; smallest living unit |
| Protoplasm | All contents of a cell (nucleus + cytoplasm) |
| Cytoplasm | Everything inside the cell membrane except the nucleus |
| Cytosol | The jelly-like fluid portion of cytoplasm (not organelles) |
| Organelle | Specialized structure within the cell with a specific function |
| Plasma membrane | The boundary membrane surrounding the cell |
| Nucleus | Control center; contains DNA |
| Nucleoplasm | Fluid within the nucleus |
| Microbiome/Microbiota | The trillions of microorganisms living in/on the body |
Components of Protoplasm (Guyton's "5 Basic Substances")
PROTOPLASM
├── Water (70-85% of most cells - the solvent of life)
├── Electrolytes (K⁺, Mg²⁺, PO₄³⁻, SO₄²⁻, HCO₃⁻ inside; Na⁺, Cl⁻ outside)
├── Proteins (10-20% of cell mass - structural + functional)
├── Lipids (mainly phospholipids + cholesterol in membranes)
└── Carbohydrates (energy + cell coating - glycocalyx)
Why water is so important: It is the medium in which ALL chemical reactions occur. Without water, biochemistry stops, and life stops.
The Two Types of Proteins in Cells
CELL PROTEINS
├── STRUCTURAL PROTEINS
│ ├── Form long filaments (polymers)
│ ├── Make microtubules, cytoskeleton
│ ├── Collagen, elastin (extracellular)
│ └── Job: Give shape, support, movement
│
└── FUNCTIONAL PROTEINS (Enzymes)
├── Globular shape, mobile in cytoplasm
├── Adhere to membranes
├── Catalyze specific reactions
└── Job: Run the chemistry of life
(e.g., split glucose + combine with O₂ → CO₂ + H₂O + ATP)
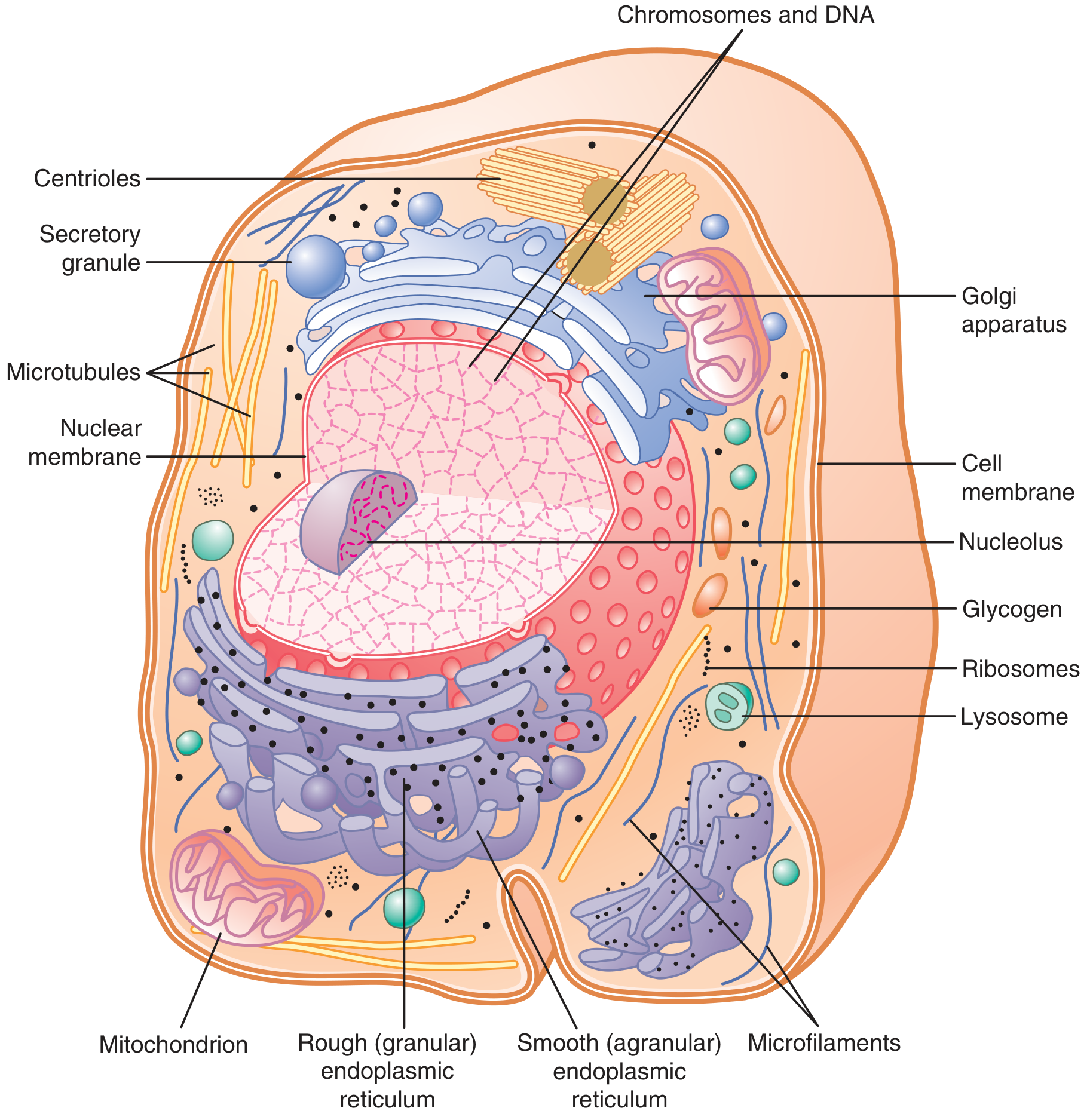
Anatomical Basis
The cell has two major divisions:
- Nucleus - separated from cytoplasm by the nuclear membrane (double membrane with pores)
- Cytoplasm - everything outside the nucleus, inside the plasma membrane
Figure 2.2 from Guyton & Hall - Study every organelle labeled here. This diagram is your foundation.
Histological Basis
Under the light microscope you can see:
- Nucleus (darkly stained with hematoxylin - H&E stain)
- Nucleolus (dark spot within nucleus - site of rRNA synthesis)
- Cytoplasm (pink with eosin - H&E stain)
- Cell boundaries
Under the electron microscope you can see:
- All organelle ultrastructure
- Membrane bilayer detail
- Ribosomes on rough ER
Exam tip: H&E stain = Hematoxylin (blue/purple - nucleus) + Eosin (pink - cytoplasm). This is the most common stain in histology.
Biochemical Basis
Every organelle function ultimately requires:
- ATP (energy currency) - made in mitochondria
- Enzymes (protein catalysts) - made on ribosomes
- Lipids (membrane structure) - made in smooth ER
- Nucleic acids (DNA/RNA for instructions) - stored in nucleus
━━━━━━━━━━━━━━━━━━━━
STAGE 3: CORE PHYSIOLOGY - THE ORGANELLES
━━━━━━━━━━━━━━━━━━━━
THE CELL MEMBRANE (Plasma Membrane)
What is it?
A thin, pliable, elastic structure 7.5 to 10 nanometers thick (Guyton) surrounding the cell.
Composition (Guyton's exact values - HIGH YIELD):
Cell Membrane Composition:
├── Proteins: 55% (the majority!)
├── Phospholipids: 25%
├── Cholesterol: 13%
├── Other lipids: 4%
└── Carbohydrates: 3%
Memory trick: "Physiology Course Come Other Classes" = Proteins 55, Cholesterol 13, Carbohydrates 3, Other lipids 4, phosphoChospholipids 25.
Or simply remember: Proteins dominate (55%), then phospholipids.
The Lipid Bilayer - Structure
OUTSIDE of cell (extracellular)
┌─────────────────────────────────┐
│ ~~~~POLAR HEADS (hydrophilic)~~ │ ← Phospholipid heads face water
│ |||||||||||||||||||||||||||||| │ ← Fatty acid tails (hydrophobic)
│ |||||||||||||||||||||||||||||| │ ← Fatty acid tails (hydrophobic)
│ ~~~~POLAR HEADS (hydrophilic)~~ │ ← Phospholipid heads face water
└─────────────────────────────────┘
INSIDE of cell (intracellular)
- Hydrophilic heads face water (outside and inside)
- Hydrophobic tails face each other in the middle
- This arrangement is self-sealing - if you poke a hole, it heals automatically
- Cholesterol sits between phospholipids - it maintains fluidity (prevents freezing at low temps AND prevents melting at high temps) = membrane fluidity buffer
Types of Membrane Proteins (Guyton - HIGH YIELD)
MEMBRANE PROTEINS
├── INTEGRAL PROTEINS (Intrinsic)
│ ├── Span the ENTIRE thickness of membrane
│ ├── Called "transmembrane proteins"
│ ├── Functions:
│ │ ├── Ion channels (Na⁺, K⁺, Ca²⁺ channels)
│ │ ├── Carrier proteins (glucose transporters)
│ │ ├── Pumps (Na⁺-K⁺ ATPase)
│ │ ├── Receptors (insulin receptor, beta-adrenergic receptor)
│ │ └── Enzymes (adenylyl cyclase)
│ └── Cannot be extracted without disrupting the membrane
│
└── PERIPHERAL PROTEINS (Extrinsic)
├── Attached to SURFACE only (inner or outer)
├── Loosely attached, can be removed
└── Functions: Enzymes, structural support, signal transduction
Analogy: Think of the membrane as a swimming pool. The phospholipids are the water. Integral proteins are like people swimming through the pool (going all the way from one side to the other). Peripheral proteins are like people sitting at the edge, just dipping their feet in.
Functions of the Cell Membrane
| Function | Mechanism | Clinical Relevance |
|---|
| Selective barrier | Controls what enters/exits | Loss → cell lysis, edema |
| Communication | Receptors bind signals | Insulin resistance = receptor dysfunction |
| Transport | Channels, carriers, pumps | Cystic fibrosis = CFTR channel mutation |
| Identity (Self-recognition) | Glycoproteins (ABO blood group) | Blood transfusion reactions |
| Structural integrity | Cytoskeleton attachment | Hereditary spherocytosis |
THE ENDOPLASMIC RETICULUM (ER)
What is it?
A massive network of tubular structures (cisternae) and flat vesicles within the cytoplasm. Its total surface area can be 30-40 times the cell membrane area in liver cells! (Guyton)
Two Types:
ENDOPLASMIC RETICULUM
│
├── ROUGH ER (Granular ER)
│ ├── Has RIBOSOMES attached on outer surface
│ ├── Continuous with nuclear membrane
│ ├── Function: PROTEIN SYNTHESIS + processing
│ ├── Makes: secretory proteins, membrane proteins, lysosomal proteins
│ └── "Rough" = rough due to ribosome bumps
│
└── SMOOTH ER (Agranular ER)
├── NO ribosomes attached
├── Less extensive than rough ER
├── Functions:
│ ├── LIPID SYNTHESIS (phospholipids, steroids, cholesterol)
│ ├── DRUG DETOXIFICATION (liver - cytochrome P450 enzymes here!)
│ ├── Ca²⁺ storage (especially in muscle cells - sarcoplasmic reticulum)
│ └── Carbohydrate metabolism
└── "Smooth" = smooth, no bumps
Clinical pearl: The liver has massive amounts of smooth ER because it detoxifies drugs via cytochrome P450 (CYP) enzymes. Alcoholics have ENLARGED smooth ER (enzyme induction) - this is why they metabolize drugs faster.
ER stress response (Unfolded Protein Response - UPR): When proteins accumulate incorrectly in the ER, it sends a signal to the nucleus to slow ribosomal translation. This is a quality control mechanism. In diseases like diabetes and neurodegeneration, chronic ER stress contributes to cell death.
THE GOLGI APPARATUS
What is it?
A series of flat, membrane-bound sacs (cisternae) stacked like a pile of pancakes. It is the "Post Office" or "Processing and Shipping Center" of the cell.
Flow through Golgi:
Proteins arrive from Rough ER (in vesicles)
↓
CIS face (receiving face - faces ER)
↓
Medial Golgi (processing: glycosylation, phosphorylation, sulfation)
↓
TRANS face (shipping face - faces cell membrane)
↓
Sorted into vesicles and sent to:
├── Cell surface (secretion - EXOCYTOSIS)
├── Lysosomes (degradation)
└── Other organelles
Memory trick: Golgi = "Gift wrapping + Going out station" - it packages and addresses proteins for their final destination.
Clinical pearl: Failure of Golgi processing = I-cell disease (mucolipidosis II) - lysosomal enzymes are not tagged with mannose-6-phosphate, so they are secreted outside instead of going to lysosomes. Cells accumulate undegraded material → "inclusion bodies" → severe storage disease.
LYSOSOMES
What are they?
Membrane-bound sacs containing digestive enzymes (hydrolases). They are the "Stomach" or "Recycling Plant" of the cell.
Key Features:
- pH inside lysosomes = 4.5-5.0 (highly acidic) - this activates hydrolases
- Cytosol pH = 7.2 (nearly neutral) - so leaking enzymes are NOT active in cytoplasm
- This pH difference is a safety mechanism
Functions:
LYSOSOMES
├── AUTOPHAGY - digesting OLD/DAMAGED organelles (self-eating)
├── HETEROPHAGY - digesting material brought IN from outside
│ ├── Endocytosis → Endosome → fuses with lysosome → digestion
│ └── Products (amino acids, glucose) released into cytosol for reuse
├── Phagocytosis - macrophages/neutrophils use lysosomes to kill bacteria
└── Apoptosis - controlled cell death (release of lysosomal enzymes)
Lysosome Storage Diseases (HIGH YIELD Clinically):
| Disease | Missing Enzyme | Accumulated Substrate | Presentation |
|---|
| Gaucher's | Beta-glucocerebrosidase | Glucocerebroside | Hepatosplenomegaly, bone pain, Gaucher cells (crinkled paper) |
| Niemann-Pick | Sphingomyelinase | Sphingomyelin | Hepatosplenomegaly, cherry-red macula |
| Tay-Sachs | Hexosaminidase A | GM2 ganglioside | Progressive neurodegeneration, cherry-red spot, no hepatosplenomegaly |
| Fabry's | Alpha-galactosidase A | Globotriaosylceramide | Neuropathic pain, angiokeratomas, renal failure |
| Pompe's | Alpha-glucosidase (acid maltase) | Glycogen | Cardiomegaly, hypotonia, death in infancy |
| Hunter's | Iduronate sulfatase | Heparan + dermatan sulfate | Coarse facies, no corneal clouding, X-linked |
| Hurler's | Alpha-L-iduronidase | Heparan + dermatan sulfate | Coarse facies, corneal clouding, gargoylism |
Memory trick for Lysosome storage diseases: "Lysosomes Store Garbage when they Can't Digest it" → Lisosomal Storage diseases = Glycolipids, Complex carbs, Dysfunction
PEROXISOMES
What are they?
Small vesicles containing oxidative enzymes, especially catalase and oxidases.
Functions:
PEROXISOMES
├── Oxidize fatty acids (VERY LONG chain fatty acids - VLCFAs)
│ Fatty acid + O₂ → CO₂ + H₂O + H₂O₂
│
├── Destroy H₂O₂ (hydrogen peroxide) using CATALASE
│ H₂O₂ → H₂O + ½O₂ (catalase reaction)
│
├── Bile acid synthesis
├── Cholesterol synthesis
└── Detoxification (alcohol → acetaldehyde)
Why is H₂O₂ destruction important? H₂O₂ is a reactive oxygen species (ROS) that damages DNA, proteins, lipids. Catalase neutralizes it. If peroxisomes fail → oxidative damage.
Clinical pearl - Zellweger Syndrome: Absence of functional peroxisomes → accumulation of VLCFAs in brain → severe neurological damage → death in infancy.
Alcohol metabolism: Ethanol → (alcohol dehydrogenase) → Acetaldehyde → (acetaldehyde dehydrogenase) → Acetate. Peroxisomes also handle some of this via catalase.
MITOCHONDRIA - "The Powerhouse of the Cell"
Structure:
MITOCHONDRION
├── OUTER MEMBRANE (smooth, permeable to small molecules)
├── INTERMEMBRANE SPACE
├── INNER MEMBRANE (highly folded into CRISTAE)
│ ├── Impermeable to most ions - this is KEY for ATP synthesis
│ ├── Contains: Electron Transport Chain (ETC) complexes
│ ├── Contains: ATP synthase (F₁F₀ ATPase)
│ └── The cristae INCREASE surface area → more ATP production
└── MATRIX (innermost fluid compartment)
├── Contains: Krebs cycle enzymes
├── Contains: Mitochondrial DNA (mtDNA - circular, like bacteria!)
├── Contains: Mitochondrial ribosomes (70S - like bacteria!)
└── Contains: Fatty acid beta-oxidation enzymes
Why do mitochondria have their own DNA? Because they evolved from engulfed bacteria (endosymbiotic theory). This explains why mitochondria are passed through the maternal line (mitochondria come from the egg, not the sperm).
Energy Production (Simplified):
GLUCOSE (6C)
↓ GLYCOLYSIS (in cytoplasm - no O₂ needed)
PYRUVATE (3C)
↓ Enter mitochondria
ACETYL-CoA (2C)
↓ KREBS CYCLE (in matrix)
CO₂ + NADH + FADH₂
↓ ELECTRON TRANSPORT CHAIN (inner membrane)
ATP + H₂O
Net yield per glucose:
- Glycolysis: 2 ATP (net)
- Krebs cycle: 2 ATP
- ETC/Oxidative phosphorylation: ~34 ATP
- Total: ~36-38 ATP per glucose molecule
Clinical Correlations:
| Situation | Effect on Mitochondria | Result |
|---|
| Cyanide poisoning | Blocks Complex IV (cytochrome c oxidase) | No ATP → rapid death |
| Metformin (diabetes drug) | Inhibits Complex I mildly | Reduces hepatic glucose production, lactic acidosis risk |
| Mitochondrial myopathies | mtDNA mutations | Muscle weakness, lactic acidosis, MELAS, MERRF |
| Ischemia (heart attack) | No O₂ → ETC stops | No ATP → cell death, infarct |
| Uncouplers (e.g., DNP) | Dissipate proton gradient | ATP not made; energy lost as heat → used as weight loss agent (dangerous!) |
MELAS = Mitochondrial Encephalomyopathy, Lactic Acidosis, Stroke-like episodes
MERRF = Myoclonic Epilepsy with Ragged Red Fibers
SECRETORY VESICLES
Small membrane-bound sacs that store secretory products (hormones, enzymes, neurotransmitters) until released by exocytosis.
Protein synthesized in Rough ER
↓
Processed in Golgi
↓
Packaged into secretory vesicle
↓
Signal received (Ca²⁺ influx, neural signal, hormone)
↓
Vesicle moves to cell membrane
↓
EXOCYTOSIS - vesicle fuses with membrane, contents released
↓
Product enters extracellular space/bloodstream
Example: Insulin secretion from pancreatic beta cells. When blood glucose rises → Ca²⁺ enters beta cell → insulin vesicles fuse with membrane → insulin secreted → blood glucose falls.
THE CYTOSKELETON
Three types of cytoskeletal elements:
CYTOSKELETON
├── MICROFILAMENTS (Actin filaments - 7nm)
│ ├── Thinnest
│ ├── Give cell shape, enable movement
│ ├── Involved in muscle contraction (with myosin)
│ └── Important in phagocytosis, cytokinesis
│
├── INTERMEDIATE FILAMENTS (10nm)
│ ├── Medium thickness - most stable
│ ├── Types: vimentin, desmin, keratin, neurofilaments, GFAP
│ └── Structural support, resist mechanical stress
│
└── MICROTUBULES (Tubulin - 25nm)
├── Thickest, hollow tubes of alpha+beta tubulin
├── Form the mitotic spindle during cell division
├── Form cilia and flagella (axoneme)
├── Transport organelles and vesicles (motor proteins: kinesin, dynein)
└── Drug target: Colchicine, Vinca alkaloids, Taxol
Clinical correlations of microtubules:
| Drug | Action on Microtubules | Clinical Use |
|---|
| Colchicine | Inhibits tubulin polymerization (prevents spindle) | Gout (inhibits neutrophil movement), familial Mediterranean fever |
| Vinca alkaloids (vincristine, vinblastine) | Same - inhibit polymerization | Cancer chemotherapy |
| Taxol (paclitaxel) | Stabilizes microtubules (prevents depolymerization) | Breast, ovarian cancer |
| Albendazole | Inhibits tubulin in parasites | Helminths, tapeworms |
Kartagener's Syndrome (Primary Ciliary Dyskinesia): Dynein arm defect → cilia don't move properly → situs inversus + bronchiectasis + infertility (sperm flagella don't move). This shows how microtubule motors are essential for normal anatomy!
THE NUCLEUS
The "Command Center" of the cell. Contains the genetic blueprint for all cellular activities.
Components:
NUCLEUS
├── NUCLEAR ENVELOPE (double membrane)
│ ├── Outer membrane: continuous with rough ER
│ ├── Inner membrane: lined by nuclear lamina
│ └── NUCLEAR PORES: allow selective exchange between nucleus and cytoplasm
│ (mRNA goes OUT, transcription factors, histones go IN)
│
├── NUCLEOPLASM (fluid inside nucleus)
│
├── CHROMATIN
│ ├── EUCHROMATIN (lightly packed) = ACTIVE DNA (being transcribed)
│ └── HETEROCHROMATIN (tightly packed) = INACTIVE DNA
│
├── NUCLEOLUS (1-2 per cell)
│ ├── Dark spot within nucleus
│ ├── NOT membrane-bound
│ ├── Site of rRNA synthesis and ribosome assembly
│ └── Prominent in cells making lots of protein (nerve cells, liver cells)
│
└── CHROMOSOMES (46 in humans = 23 pairs)
├── 22 pairs autosomes + 1 pair sex chromosomes
└── Each = 1 DNA molecule + histone proteins
Key fact: The nuclear pores are highly selective. They let through only what the cell needs at that moment. This is regulated gene expression at the structural level.
━━━━━━━━━━━━━━━━━━━━
STAGE 4: MOLECULAR & CELLULAR PHYSIOLOGY
━━━━━━━━━━━━━━━━━━━━
Cell Membrane - Molecular Detail
The Fluid Mosaic Model (Singer & Nicolson, 1972)
Key features:
1. FLUID - phospholipids can move laterally (like swimmers in a pool)
2. MOSAIC - proteins are embedded at various points (like tiles in a mosaic)
3. ASYMMETRY - inner leaflet ≠ outer leaflet
- Outer leaflet: PC (phosphatidylcholine), SM (sphingomyelin), glycolipids
- Inner leaflet: PE (phosphatidylethanolamine), PS (phosphatidylserine)
Critical clinical point - Phosphatidylserine:
PS is normally on the INNER leaflet. During apoptosis (programmed cell death), PS flips to the OUTER leaflet - this is the "eat me" signal for macrophages. Drugs like Annexin V detect this flip (used in apoptosis assays).
Second Messengers (membrane receptor signaling):
Signal (hormone, neurotransmitter) binds receptor
↓
Receptor activates G-protein (Gs, Gi, Gq)
↓
┌─────────────────────────────────┐
│ Gs → activates adenylyl cyclase │
│ → cAMP → PKA │
│ │
│ Gi → INHIBITS adenylyl cyclase │
│ → ↓ cAMP │
│ │
│ Gq → activates PLC │
│ → IP₃ + DAG │
│ IP₃ → Ca²⁺ release from ER │
│ DAG → PKC activation │
└─────────────────────────────────┘
Examples:
- Beta-1 adrenergic receptor (heart): Gs → cAMP → PKA → faster heart rate, stronger contraction
- Muscarinic M2 receptor (heart): Gi → ↓cAMP → slower heart rate
- Alpha-1 receptor (vessels): Gq → IP₃/DAG → vasoconstriction
Ion Channels - Types and Clinical Relevance
| Channel Type | How It Opens | Example | Clinical Drug |
|---|
| Voltage-gated | Change in membrane potential | Na⁺ channel (nerve) | Lidocaine (local anesthetic), Phenytoin (epilepsy) |
| Ligand-gated | Binding of neurotransmitter | GABA receptor | Benzodiazepines, barbiturates |
| Mechanically-gated | Physical force/stretch | Hearing cells (hair cells) | - |
| Second messenger-gated | cAMP, IP₃, Ca²⁺ | Ryanodine receptor (muscle) | Dantrolene (malignant hyperthermia) |
━━━━━━━━━━━━━━━━━━━━
STAGE 5: INTEGRATED PHYSIOLOGY
━━━━━━━━━━━━━━━━━━━━
How Cell Biology Connects Everything
NERVOUS SYSTEM ←→ CELL
Neurons are cells with:
- Extremely long cytoplasmic extensions (axons up to 1 meter!)
- Voltage-gated channels for action potential
- Mitochondria concentrated at synapses (high energy need)
ENDOCRINE SYSTEM ←→ CELL
Hormones bind cell membrane receptors → intracellular signals
- The receptor IS a membrane protein
- The target is the nucleus (gene expression)
- Example: Cortisol (lipid-soluble) → crosses membrane → nuclear receptor
CARDIOVASCULAR ←→ CELL
- Cardiac cells need 10x more mitochondria than average cell
- Endothelial cells produce NO (from smooth ER enzymes) → vasodilation
RENAL ←→ CELL
- Tubular cells have Na⁺-K⁺-ATPase (integral membrane protein) on basolateral side
- This is how the kidney reabsorbs everything
IMMUNE ←→ CELL
- Cell surface glycoproteins (MHC molecules) are what immune cells "read"
- T-cells check "self vs non-self" by scanning cell surface proteins
━━━━━━━━━━━━━━━━━━━━
STAGE 6: APPLIED PHYSIOLOGY
━━━━━━━━━━━━━━━━━━━━
Exercise Physiology at the Cell Level
During intense exercise:
ATP demand ↑↑↑ in muscle cells
↓
Mitochondria upregulate ETC
↓
If O₂ supply insufficient → anaerobic glycolysis
↓
Lactate produced (NOT lactic acid - it's lactate at physiological pH)
↓
Blood lactate rises → "lactic acidosis" in extreme exercise
↓
Recovery: Cori cycle - lactate → liver → glucose → back to muscle
Adaptation: Regular aerobic exercise → more mitochondria in muscle cells (mitochondrial biogenesis via PGC-1α) → more efficient ATP production → better endurance.
Aging at the Cell Level
Aging:
├── TELOMERE SHORTENING - each cell division shortens telomeres
│ → Hayflick limit (~50 divisions) → senescence → cell death
│
├── MITOCHONDRIAL DYSFUNCTION - mtDNA mutations accumulate
│ → Less ATP → organ failure
│
├── LYSOSOMAL DYSFUNCTION - accumulation of waste (lipofuscin "age pigment")
│ → Seen in old neurones as brown granules
│
└── OXIDATIVE STRESS - accumulated ROS damage
→ DNA mutations, protein aggregates
→ Alzheimer's, Parkinson's, cardiovascular disease
Lipofuscin = "wear and tear" pigment in aging cells = undigested material in secondary lysosomes = yellowish-brown granules. Seen prominently in neurons and cardiomyocytes.
━━━━━━━━━━━━━━━━━━━━
STAGE 7: CLINICAL PHYSIOLOGY
━━━━━━━━━━━━━━━━━━━━
"What Happens If It Goes Wrong?" - Organelle by Organelle
| Organelle | Dysfunction | Disease | Manifestation |
|---|
| Cell membrane | Permeability disrupted | Burns, sepsis | Massive edema, electrolyte imbalance |
| Cell membrane (channel) | CFTR Cl⁻ channel mutated | Cystic fibrosis | Thick mucus, recurrent infections, infertility |
| Cell membrane (pump) | Na⁺-K⁺-ATPase inhibited | Digitalis toxicity | Bradycardia, increased cardiac contractility |
| ER (rough) | ER stress | Multiple myeloma | Excessive antibody production overwhelms ER |
| ER (smooth) | CYP450 induced by alcohol | Drug interactions | Faster drug metabolism, reduced drug efficacy |
| Golgi | Processing failure | I-cell disease | Lysosomal storage, severe developmental delay |
| Lysosomes | Missing enzyme | Gaucher's, Tay-Sachs, etc. | Organ enlargement, neurodegeneration |
| Peroxisomes | Absent peroxisomes | Zellweger syndrome | Severe neurological damage, early death |
| Mitochondria | ETC block | Cyanide poisoning | Sudden death, "smells like almonds" |
| Mitochondria | mtDNA mutation | MELAS, MERRF | Stroke-like episodes, myopathy, lactic acidosis |
| Cytoskeleton | Dynein defect | Kartagener's | Situs inversus, bronchiectasis, infertility |
| Nucleus (DNA) | Mutations accumulate | Cancer | Uncontrolled proliferation |
━━━━━━━━━━━━━━━━━━━━
STAGE 8: PATHOPHYSIOLOGY
━━━━━━━━━━━━━━━━━━━━
Case Study: Lysosomal Storage Disease (Tay-Sachs)
NORMAL:
GM2 ganglioside (in neurons)
↓ Hexosaminidase A
Breakdown products → excreted safely
MUTATION: HEX A gene mutation (autosomal recessive)
↓
No Hexosaminidase A in lysosomes
↓
GM2 ganglioside ACCUMULATES in lysosomes (especially neurons)
↓
Lysosomes swell → "ganglion cell ballooning"
↓
Neurons cannot function → die
↓
SIGNS & SYMPTOMS:
├── Normal at birth (maternal enzyme clears substrate in utero)
├── 3-6 months: progressive motor weakness
├── Cherry-red macula (fovea has no ganglion cells → normal red,
│ surrounded by white swollen ganglion cells)
├── Progressive neurodegeneration, blindness, seizures
└── Death by age 2-5 years
COMPLICATIONS:
├── Aspiration pneumonia
└── No treatment (enzyme replacement doesn't cross blood-brain barrier)
Case Study: Cyanide Poisoning (Mitochondria)
NORMAL:
O₂ → Complex IV (cytochrome c oxidase) → H₂O + ATP produced
CYANIDE EXPOSURE (from fires, industrial, apricot seeds):
↓
CN⁻ binds Fe³⁺ in Complex IV → IRREVERSIBLE BLOCK
↓
Electron transport STOPS
↓
No proton gradient → No ATP synthesis
↓
Cells cannot use O₂ (even though it's available)
↓
"HISTOTOXIC HYPOXIA" - O₂ is there but can't be used
↓
SIGNS: Lactic acidosis, cherry-red skin (O₂-saturated venous blood),
seizures, coma, cardiac arrest
↓
TREATMENT:
├── Hydroxocobalamin (B12 derivative) - binds CN⁻ → cyanocobalamin (excreted)
├── Sodium thiosulfate - CN⁻ + thiosulfate → thiocyanate (non-toxic)
└── Sodium nitrite - creates methemoglobin which has HIGH affinity for CN⁻
━━━━━━━━━━━━━━━━━━━━
STAGE 9: PHARMACOLOGICAL CORRELATIONS
━━━━━━━━━━━━━━━━━━━━
Drugs Acting on Cell Components
| Drug | Target | Mechanism | Use |
|---|
| Colchicine | Microtubules | Binds tubulin → prevents polymerization → stops neutrophil movement | Gout, FMF |
| Taxol (Paclitaxel) | Microtubules | Stabilizes (prevents depolymerization) → cell can't divide | Cancer |
| Vincristine/Vinblastine | Microtubules | Prevents polymerization | Cancer |
| Dantrolene | Ryanodine receptor (sarcoplasmic ER) | Blocks Ca²⁺ release | Malignant hyperthermia |
| Chloroquine | Lysosomes | Raises lysosomal pH → impairs pathogen digestion | Malaria, SLE |
| Statins | Smooth ER (HMG-CoA reductase) | Inhibit cholesterol synthesis | Hyperlipidemia |
| Metformin | Mitochondria | Inhibits Complex I → less ATP → AMPK activation | Type 2 Diabetes |
| Digitalis (Digoxin) | Na⁺-K⁺-ATPase (cell membrane) | Inhibits pump → Ca²⁺ accumulates → stronger heart contraction | Heart failure, AF |
| Lidocaine | Voltage-gated Na⁺ channels (membrane) | Blocks Na⁺ entry → no action potential | Local anesthesia, arrhythmia |
━━━━━━━━━━━━━━━━━━━━
STAGE 10: IMPORTANT GRAPHS
━━━━━━━━━━━━━━━━━━━━
Graph 1: Membrane Fluidity vs Temperature
Membrane Fluidity
(Liquid state)
|
| Without cholesterol
|\
| \
| \___________ ← Sharp transition (gel → liquid)
|
| With cholesterol
| ~~~~~~~~~~~~~~~~~~ ← Gradual, buffered transition
|
+----------------------------------→ Temperature
Cold Hot
Interpretation:
- Without cholesterol: membrane goes from rigid (gel phase) to fluid (liquid phase) sharply with temperature
- With cholesterol: the transition is smooth - membrane stays usable across a wide temperature range
- Why this matters: Cholesterol is a membrane fluidity buffer - prevents freezing at cold AND prevents disintegration at heat
- Clinical: Cholesterol-lowering drugs (statins) reduce cholesterol → may affect membrane fluidity
━━━━━━━━━━━━━━━━━━━━
STAGE 11: IMPORTANT TABLES
━━━━━━━━━━━━━━━━━━━━
Rough ER vs Smooth ER
| Feature | Rough ER | Smooth ER |
|---|
| Ribosomes | YES (attached) | NO |
| Appearance | Rough/granular | Smooth |
| Main function | Protein synthesis | Lipid synthesis, detoxification, Ca²⁺ storage |
| Prominent in | Secretory cells, plasma cells | Liver cells, steroid-producing cells, muscle cells |
| Clinical relevance | Plasma cell: antibody production | Liver: CYP450 drug metabolism |
Organelles: Summary Comparison
| Organelle | Shape | Function | Clinical Disease |
|---|
| Cell Membrane | Sheet (bilayer) | Barrier, receptors, transport | CF (CFTR), hereditary spherocytosis |
| Rough ER | Tubular network | Protein synthesis | Myeloma (overactive), ER stress |
| Smooth ER | Tubular, no ribosomes | Lipid synthesis, detox | Alcohol-induced enzyme induction |
| Golgi | Stacked sacs | Processing, packaging, shipping | I-cell disease |
| Lysosomes | Spherical vesicles | Digestion, recycling | Gaucher's, Tay-Sachs, Pompe's |
| Peroxisomes | Spherical | Fatty acid oxidation, H₂O₂ neutralization | Zellweger syndrome |
| Mitochondria | Oval, double membrane | ATP synthesis | MELAS, cyanide poisoning |
| Nucleus | Spherical (double membrane) | DNA storage, gene expression | Cancer (DNA mutation) |
━━━━━━━━━━━━━━━━━━━━
STAGE 12: NUMERICAL VALUES - HIGH YIELD
━━━━━━━━━━━━━━━━━━━━
| Value | Number | Unit | Significance |
|---|
| Total body cells | 35-40 trillion | cells | Human body size |
| Red blood cells | 25 trillion | cells | Most numerous cell type |
| Cell membrane thickness | 7.5-10 | nanometers | Extremely thin! |
| Membrane protein content | 55% | % of membrane | Proteins dominate |
| Membrane phospholipid content | 25% | % of membrane | Main structural lipid |
| Membrane cholesterol | 13% | % of membrane | Fluidity regulator |
| Intracellular water | 70-85% | % of cell mass | Main component |
| Intracellular protein | 10-20% | % of cell mass | 2nd most abundant |
| Lysosomal pH | 4.5-5.0 | pH units | Acidic (activates hydrolases) |
| Cytosol pH | 7.2 | pH units | Near neutral |
| ATP from 1 glucose | 36-38 | ATP molecules | Energy yield of metabolism |
| Mitochondrial DNA | 37 | genes | Encodes 13 proteins, 22 tRNAs, 2 rRNAs |
| Human chromosomes | 46 | (23 pairs) | Diploid number |
| Smooth ER surface area (liver) | 30-40x cell membrane | fold increase | Liver's detox capacity |
━━━━━━━━━━━━━━━━━━━━
STAGE 13: VIVA PREPARATION
━━━━━━━━━━━━━━━━━━━━
Short Viva Questions
Q1. What is the most abundant substance in most cells?
A: Water (70-85% of cell mass)
Q2. What is the approximate thickness of the cell membrane?
A: 7.5-10 nanometers
Q3. What percentage of the cell membrane is proteins?
A: 55% (proteins are the most abundant component)
Q4. What is the difference between rough and smooth ER?
A: Rough ER has ribosomes attached (synthesizes proteins); Smooth ER has no ribosomes (synthesizes lipids, detoxifies drugs, stores Ca²⁺)
Q5. What enzyme is in peroxisomes that destroys H₂O₂?
A: Catalase
Q6. What is the pH inside lysosomes and why is it important?
A: pH 4.5-5.0; acidic pH activates hydrolytic (digestive) enzymes
Q7. Why do mitochondria have their own DNA?
A: Because they evolved from endosymbiotic bacteria (endosymbiotic theory). Mitochondrial DNA is circular, like bacterial DNA, and mitochondria have 70S ribosomes.
Q8. What drug targets microtubules and is used in gout?
A: Colchicine - it binds tubulin and prevents polymerization, stopping neutrophil migration to the site of urate crystal inflammation.
Q9. What is I-cell disease and which organelle does it affect?
A: I-cell disease (mucolipidosis II) - Golgi apparatus fails to add mannose-6-phosphate tag to lysosomal enzymes → enzymes secreted outside cell → lysosomes cannot digest material → inclusion bodies accumulate.
Q10. What is Kartagener's syndrome and which cytoskeletal component is defective?
A: Primary ciliary dyskinesia with situs inversus + bronchiectasis + infertility. Defect: dynein arms of microtubules (cilia can't beat effectively).
Long Viva Questions
Q1. Describe the structure and functions of the cell membrane in detail, with pharmacological correlations.
(Answer should cover: lipid bilayer, composition, integral vs peripheral proteins, channels, pumps, receptors, fluid mosaic model, clinical drugs acting on each component)
Q2. Discuss the endoplasmic reticulum - types, functions, clinical relevance, and drugs.
(Answer: Rough ER - ribosomes, protein synthesis, mRNA processing; Smooth ER - lipid synthesis, CYP450, Ca²⁺; ER stress response; drugs - statins act on ER enzyme HMG-CoA reductase; dantrolene blocks ER Ca²⁺ release)
Q3. Explain the pathophysiology of lysosomal storage diseases with three examples.
(Answer: missing enzyme → substrate accumulation → lysosome enlargement → cell dysfunction → organ failure; Gaucher's, Tay-Sachs, Pompe's)
━━━━━━━━━━━━━━━━━━━━
STAGE 14: EXAM PREPARATION
━━━━━━━━━━━━━━━━━━━━
MBBS University Exam High-Yield Points
- Cell membrane composition (memorize exact %: 55% protein, 25% phospholipid, 13% cholesterol)
- Fluid mosaic model - Singer and Nicolson 1972
- Integral vs peripheral proteins - definition, examples, functions
- Rough vs smooth ER - differences and functions
- Golgi as "post office" - cis to trans flow
- Lysosomal pH and why it matters
- Mitochondria - structure (cristae = inner membrane folds = more surface area = more ATP)
- Mitochondria - own DNA, maternal inheritance
- Cytoskeleton - 3 types (microfilaments, intermediate, microtubules) and their diameters
- Nuclear pores - selective transport
PG Entrance Concepts (USMLE/NEET PG/AIIMS)
- Cherry-red spot on macula - Tay-Sachs, Niemann-Pick (lysosomal storage)
- Gaucher cells ("crinkled paper cells") - glucocerebrosidase deficiency
- Pompe disease = "acid maltase" deficiency = glycogen in lysosomes = cardiomyopathy
- Zellweger = peroxisome disorder = VLCFA accumulation = brain damage
- MELAS/MERRF = mitochondrial disorders = maternal inheritance
- I-cell disease = Golgi dysfunction = mannose-6-phosphate tag missing
- Kartagener's = dynein defect = situs inversus
- Malignant hyperthermia = ryanodine receptor = dantrolene treatment
- Cyanide = Complex IV block = histotoxic hypoxia = hydroxocobalamin treatment
- Digoxin = Na⁺-K⁺-ATPase inhibition = positive inotrope
━━━━━━━━━━━━━━━━━━━━
STAGE 15: MEMORY TOOLS
━━━━━━━━━━━━━━━━━━━━
Mnemonics
Cell Membrane Composition (55, 25, 13, 4, 3):
"Proteins Predominate, Cholesterol Comes Last"
55% Proteins, 25% Phospholipids, 13% Cholesterol, 4% other Cholesterols/lipids, 3% Carbohydrates
Lysosomal Storage Diseases - "Fat Fred Never Keeps Good Habits":
- Fabry's (alpha-galactosidase A deficiency)
- Farber's
- Niemann-Pick (sphingomyelinase)
- Krabbe's
- Gaucher's (beta-glucocerebrosidase)
- Hurler's / Hunter's
Mucopolysaccharidoses - "Hunters Hardly Hunt Huddled Masses":
- Hunter's = Type II, No corneal clouding, X-linked, male only
- Hurler's = Type I, corneal Haze (clouding), gargoylism
Analogies
Cell = A factory/city:
- Cell membrane = City boundary wall with gates (selective permeability)
- Nucleus = Mayor's office / City hall (command and control)
- Rough ER = Manufacturing unit (proteins)
- Smooth ER = Chemical plant + refinery (lipids, detox)
- Golgi = Post office + packaging + shipping
- Lysosomes = Garbage disposal / recycling center
- Peroxisomes = Hazardous waste treatment plant (H₂O₂ neutralized)
- Mitochondria = Power plant (ATP)
- Cytoskeleton = Roads and railway tracks
Mitochondria = Power plant:
- Outer membrane = outer wall of power plant (accessible)
- Intermembrane space = turbine hall
- Inner membrane (cristae) = turbines (where electricity/ATP is generated)
- Matrix = control room (Krebs cycle enzymes)
━━━━━━━━━━━━━━━━━━━━
STAGE 16: FLOWCHART & MIND MAP
━━━━━━━━━━━━━━━━━━━━
Master Flowchart: Protein Synthesis to Secretion
DNA in NUCLEUS
↓ Transcription
mRNA (exits through nuclear pores)
↓
RIBOSOMES on ROUGH ER
↓ Translation
New Protein (enters ER lumen)
↓ Processing in ER (folding, initial glycosylation)
Transport vesicle buds off
↓
CIS-GOLGI (receives protein)
↓ Further glycosylation, phosphorylation, sulfation
TRANS-GOLGI (sorts and ships)
↓
├── SECRETORY VESICLE → EXOCYTOSIS (outside cell)
├── PLASMA MEMBRANE PROTEIN (inserted into membrane)
└── LYSOSOME (tagged with M6P)
Mind Map: THE CELL
CELL
|
________________|________________
| | |
MEMBRANE CYTOPLASM NUCLEUS
| | |
Lipid bilayer Cytosol Nuclear membrane
Proteins Organelles Nucleolus
├─ Integral ├─ Rough ER Chromatin
└─ Peripheral ├─ Smooth ER DNA (46 chr)
Carbohydrates ├─ Golgi
(glycocalyx) ├─ Lysosomes
├─ Peroxisomes
├─ Mitochondria
├─ Secretory vesicles
└─ Cytoskeleton
├─ Actin (7nm)
├─ Intermediate (10nm)
└─ Microtubules (25nm)
━━━━━━━━━━━━━━━━━━━━
STAGE 17: COMMON MISTAKES
━━━━━━━━━━━━━━━━━━━━
Misconceptions to Avoid
1. "The cell membrane is mainly lipid"
WRONG. Proteins are 55% - proteins are the MAJOR component. Lipids are 25+13+4 = 42%.
2. "Smooth ER and Rough ER are completely separate"
WRONG. They are continuous with each other and with the nuclear envelope.
3. "Lysosomes are only for destroying foreign material"
WRONG. They also perform AUTOPHAGY (digesting your own old/damaged organelles) - essential for cell survival.
4. "Mitochondria only make ATP"
WRONG. They also regulate apoptosis (release cytochrome c → caspase activation → cell death), calcium homeostasis, and heat production (uncoupling).
5. "Cholesterol is bad for membranes"
WRONG in the CONTEXT OF CELL BIOLOGY. Cholesterol is ESSENTIAL for membrane fluidity and stability. The problem is excess cholesterol in blood vessels, not in cell membranes.
6. "Tay-Sachs and Niemann-Pick both show hepatosplenomegaly"
WRONG. Tay-Sachs affects NEURONS specifically - NO hepatosplenomegaly. Niemann-Pick DOES have hepatosplenomegaly. Both have cherry-red macula.
7. "Mitchondrial inheritance is equal from mother and father"
WRONG. Mitochondria are inherited ONLY from mother (maternal inheritance) - from the egg, not sperm.
8. "Rough ER makes all proteins"
WRONG. Rough ER makes SECRETORY proteins, membrane proteins, and lysosomal proteins. FREE ribosomes (not on ER) make cytoplasmic and nuclear proteins.
━━━━━━━━━━━━━━━━━━━━
STAGE 18: RAPID REVISION
━━━━━━━━━━━━━━━━━━━━
20 Key Takeaways
- Human body = 35-40 trillion cells; RBCs are the most numerous (25 trillion)
- Cell = bounded by plasma membrane (7.5-10 nm thick; 55% protein, 25% phospholipid)
- Phospholipid bilayer = hydrophilic heads out, hydrophobic tails in; self-sealing
- Cholesterol = membrane fluidity buffer (prevents extremes)
- Integral proteins = span entire membrane; include channels, pumps, receptors
- Peripheral proteins = surface only; easily removed
- Rough ER = ribosomes attached → protein synthesis; connects to nuclear envelope
- Smooth ER = no ribosomes → lipid synthesis, CYP450 drug detox, Ca²⁺ storage
- Golgi = post office; cis (receives) → trans (ships); adds M6P tag for lysosomes
- Lysosomes = pH 4.5-5 → acidic hydrolases; autophagy + heterophagy
- Lysosomal storage disease = missing enzyme → substrate builds up
- Peroxisomes = oxidize VLCFAs; catalase destroys H₂O₂; Zellweger = peroxisome disorder
- Mitochondria = double membrane; cristae = inner membrane folds = more ATP
- Mitochondria = own circular DNA, 70S ribosomes → maternal inheritance
- ATP yield: 36-38 molecules per glucose (glycolysis 2 + Krebs 2 + ETC ~34)
- Cytoskeleton: microfilaments (7nm actin), intermediate (10nm), microtubules (25nm tubulin)
- Colchicine/vincristine/taxol = target microtubules
- Nucleus: nuclear pores = selective; euchromatin = active; heterochromatin = inactive
- Nucleolus = rRNA synthesis + ribosome assembly
- Phosphatidylserine flip to outer leaflet = apoptosis signal = "eat me" for macrophages
Clinical Pearls
- Cherry-red macula + no hepatosplenomegaly + neurodegeneration = Tay-Sachs
- Cherry-red macula + hepatosplenomegaly = Niemann-Pick
- Crinkled paper cells (Gaucher cells) in spleen = Gaucher's disease
- Cardiomegaly + hypotonia in infant = Pompe disease (glycogen in lysosomes)
- Situs inversus + bronchiectasis + male infertility = Kartagener's (dynein defect)
- Lactic acidosis + stroke-like episodes + maternal inheritance = MELAS
- Cherry-red skin + metabolic acidosis + almond smell = Cyanide poisoning (Complex IV block)
- Digoxin toxicity = Na⁺-K⁺-ATPase inhibited → hyperkalemia, bradycardia, arrhythmias
━━━━━━━━━━━━━━━━━━━━
STAGE 19: CLINICAL CASES
━━━━━━━━━━━━━━━━━━━━
Case 1 (Basic)
A 6-month-old baby, previously normal, now shows progressive weakness and decreased eye contact. Eye examination shows a cherry-red spot at the macula. No enlargement of liver or spleen. Family history: parents are Ashkenazi Jewish.
Using your knowledge of cell physiology:
- Which organelle is malfunctioning?
- What enzyme is deficient?
- What accumulates inside neurons?
- Why is there no hepatosplenomegaly?
- What does the cherry-red spot represent anatomically?
Case 2 (Intermediate)
A 45-year-old man is brought to the ER after a house fire. He is confused, with bright red skin despite normal or high oxygen saturation. ABG shows severe metabolic acidosis. Venous blood appears arterial-red in color.
Using cell physiology, explain:
- Which organelle/complex is poisoned?
- Why is venous blood cherry-red?
- Why is there lactic acidosis despite normal O₂ levels?
- What is the treatment and its mechanism?
- What term describes this type of hypoxia?
Case 3 (Advanced)
A 28-year-old woman presents with recurrent respiratory infections since childhood, dextrocardia on chest X-ray, and inability to conceive. Semen analysis of her brother shows severe oligoasthenospermia.
Using cell physiology, explain the entire pathophysiology:
- What structure is defective?
- How does this produce situs inversus?
- How does it cause bronchiectasis?
- Why is the brother infertile?
- What is the inheritance pattern?
- What physiological principle explains why cilia normally need to beat in a coordinated pattern?
━━━━━━━━━━━━━━━━━━━━
STAGE 20: ACTIVE RECALL - MCQs
━━━━━━━━━━━━━━━━━━━━
Q1. The cell membrane is composed of approximately what percentage of proteins?
- A) 13%
- B) 25%
- C) 55%
- D) 3%
Q2. A student states: "Smooth ER synthesizes proteins while Rough ER synthesizes lipids." This is:
- A) Correct
- B) Incorrect - it is reversed
- C) Partially correct
- D) Correct only for liver cells
Q3. A 3-year-old presents with hepatosplenomegaly, coarse facial features, corneal clouding, and developmental delay. Enzyme assay shows deficiency of alpha-L-iduronidase. Which organelle is dysfunctional?
- A) Peroxisome
- B) Mitochondria
- C) Lysosome
- D) Golgi apparatus
Q4. Which drug works by stabilizing microtubules (preventing depolymerization)?
- A) Colchicine
- B) Vincristine
- C) Paclitaxel (Taxol)
- D) Albendazole
Q5. Mitochondrial diseases are inherited through which parent, and why?
- A) Father - mitochondria come from sperm
- B) Mother - mitochondria come from the egg
- C) Either parent equally
- D) Both parents (codominant)
Q6. A child is found to have no functional peroxisomes. Which fatty acids would accumulate?
- A) Short-chain fatty acids
- B) Medium-chain fatty acids
- C) Very long-chain fatty acids (VLCFAs)
- D) Unsaturated fatty acids
Q7. (Assertion-Reason)
- Assertion: Lysosomal hydrolases do not damage the cytoplasm when lysosomes rupture.
- Reason: Lysosomal hydrolases require an acidic pH (~4.5) for activity, and the cytosol pH is ~7.2.
- A) Both A and R are true, R is the correct explanation of A
- B) Both A and R are true, R is NOT the correct explanation
- C) A is true, R is false
- D) A is false, R is true
Q8. Digoxin (Digitalis) exerts its positive inotropic effect by inhibiting which cell membrane component?
- A) Voltage-gated Ca²⁺ channels
- B) Na⁺-K⁺-ATPase pump
- C) CFTR Cl⁻ channel
- D) Na⁺-glucose cotransporter
Answer Key
| Q | Answer | Explanation |
|---|
| 1 | C (55%) | Proteins are the MAJORITY component of cell membrane |
| 2 | B (Reversed) | Rough ER synthesizes proteins; Smooth ER synthesizes lipids |
| 3 | C (Lysosome) | Hurler's syndrome = lysosomal storage disease; alpha-L-iduronidase processes heparan+dermatan sulfate |
| 4 | C (Paclitaxel) | Taxol STABILIZES microtubules; colchicine + vincristine PREVENT polymerization |
| 5 | B (Mother) | Eggs contain many mitochondria; sperm contribute almost no mitochondria to the fertilized egg |
| 6 | C (VLCFAs) | Peroxisomes specialize in beta-oxidation of VLCFAs (>C22); absence = VLCFA accumulation |
| 7 | A | Both are true; the pH mechanism is exactly why lysosomal enzymes are "safe" in cytosol |
| 8 | B (Na⁺-K⁺-ATPase) | Digoxin blocks the pump → Na⁺ accumulates inside cell → Na⁺-Ca²⁺ exchanger reverses → Ca²⁺ builds up → stronger myocardial contraction |
━━━━━━━━━━━━━━━━━━━━
ONE-PAGE SUMMARY: THE CELL
━━━━━━━━━━━━━━━━━━━━
┌──────────────────────────────────────────────────────────────────────┐
│ THE CELL - GUYTON & HALL │
│ (Quick Revision Card) │
├──────────────────────────────────────────────────────────────────────┤
│ Total body cells: 35-40 trillion | RBCs: 25 trillion │
│ Protoplasm = H₂O (70-85%) + Proteins (10-20%) + Lipids + Carbs + Ions│
├───────────────┬──────────────────────────────────────────────────────┤
│ ORGANELLE │ FUNCTION → DISEASE IF ABSENT │
├───────────────┼──────────────────────────────────────────────────────┤
│ Cell membrane │ Barrier, signaling → CF (CFTR), Digitalis toxicity │
│ Rough ER │ Protein synthesis → ER stress (myeloma) │
│ Smooth ER │ Lipid synthesis, CYP450, Ca²⁺ → Zellweger (perox) │
│ Golgi │ Post office → I-cell disease (no M6P tag) │
│ Lysosomes │ Digestion (pH 4.5-5) → Gaucher's, Tay-Sachs, Pompe │
│ Peroxisomes │ VLCFA oxidation, catalase → Zellweger syndrome │
│ Mitochondria │ ATP (36-38/glucose), maternal DNA → MELAS, cyanide │
│ Cytoskeleton │ Shape, movement → Kartagener's (dynein), colchicine │
│ Nucleus │ DNA, gene expression → Cancer │
├───────────────┴──────────────────────────────────────────────────────┤
│ KEY VALUES: Membrane = 7.5-10nm | Proteins 55% | Lysosomes pH 4.5-5 │
│ Mitochondria have OWN DNA (37 genes) | maternal inheritance │
│ Cytoskeleton: Actin 7nm | Intermediate 10nm | Microtubules 25nm │
├──────────────────────────────────────────────────────────────────────┤
│ DRUG TARGETS: Colchicine/Taxol → microtubules | Digoxin → Na⁺-K⁺pump│
│ Statins → ER (HMG-CoA reductase) | Dantrolene → ER Ca²⁺ release │
│ Metformin → Mitochondria Complex I | Cyanide → Complex IV block │
└──────────────────────────────────────────────────────────────────────┘
SOURCE: Guyton and Hall Textbook of Medical Physiology (14th Ed.), Chapter 2, Unit I. All content verified directly from the textbook.
What's Next?
Session 1 is complete. We have covered the entire cell - from basic structure to advanced clinical pharmacology. You now understand:
- Why the cell exists and its homeostatic role
- All organelles - structure, function, disease, and drugs
- 8 clinical scenarios linked to cell pathology
- 20 MCQs for self-testing
- Memory tools for long-term retention
Next logical topic options (Guyton sequence):
- Transport Across Cell Membranes - diffusion, osmosis, active transport, channels (this directly builds on what we just learned)
- The Action Potential - how neurons use membrane properties to transmit signals
- Homeostasis and Control Systems - negative feedback, positive feedback, control mechanisms
Which topic would you like next? We can continue in strict Guyton sequence, or you can pick any subtopic you want to master deeper.