meniscal tears and repair
Reading File
Finding Sources
Finding Sources
Searching PubMed
"meniscal tear" AND repair
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Excellent — all four images are very clear and informative. I now have comprehensive content to deliver a thorough answer.
Meniscal Tears and Repair
Anatomy & Function
The menisci are paired C-shaped fibrocartilaginous structures that sit on the tibial plateau medially and laterally. Their primary roles are:
- Load distribution — transmitting ~50–70% of compressive forces across the knee compartment
- Shock absorption
- Joint stability and proprioception
Loss of meniscal tissue — through tear or excision — concentrates focal stress on articular cartilage, accelerating degenerative arthritis, particularly on the lateral side.
Epidemiology
- Meniscal tear is the most common knee injury requiring surgery
- The medial meniscus is torn ~3× more often than the lateral
- However, lateral meniscus tears occur more commonly with acute ACL injuries
- Traumatic tears predominate in young, athletic patients; degenerative tears occur insidiously in older patients
— Miller's Review of Orthopaedics, 9th Ed.
Vascular Zones (Key to Healing Potential)
The meniscus has three zones based on blood supply from the perimeniscal capillary plexus:
| Zone | Blood Supply | Healing Potential |
|---|---|---|
| Red-Red (peripheral third) | Well vascularized | High — best candidate for repair |
| Red-White (middle third) | Partial | Intermediate |
| White-White (inner/central) | Avascular | Poor — generally not repairable |
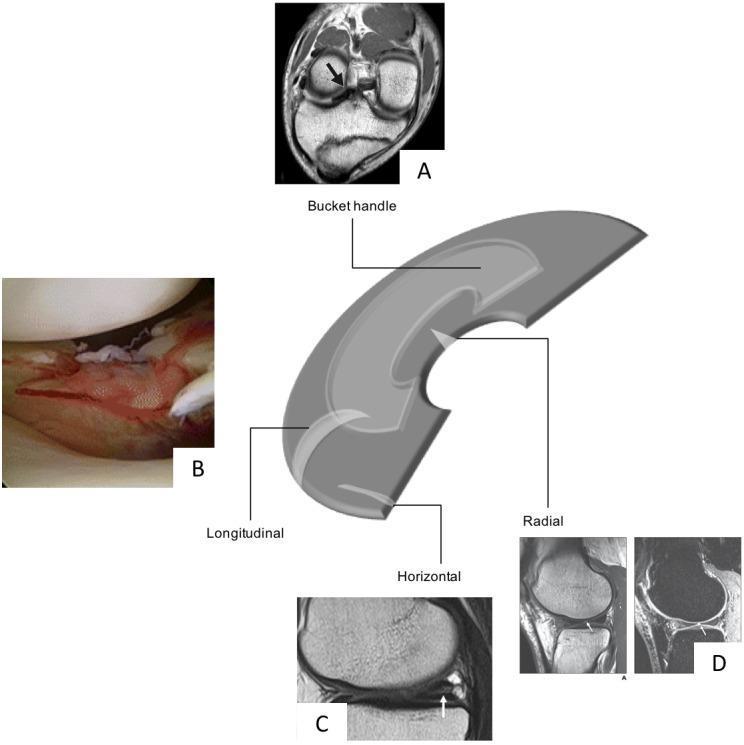
Classification of Tear Patterns
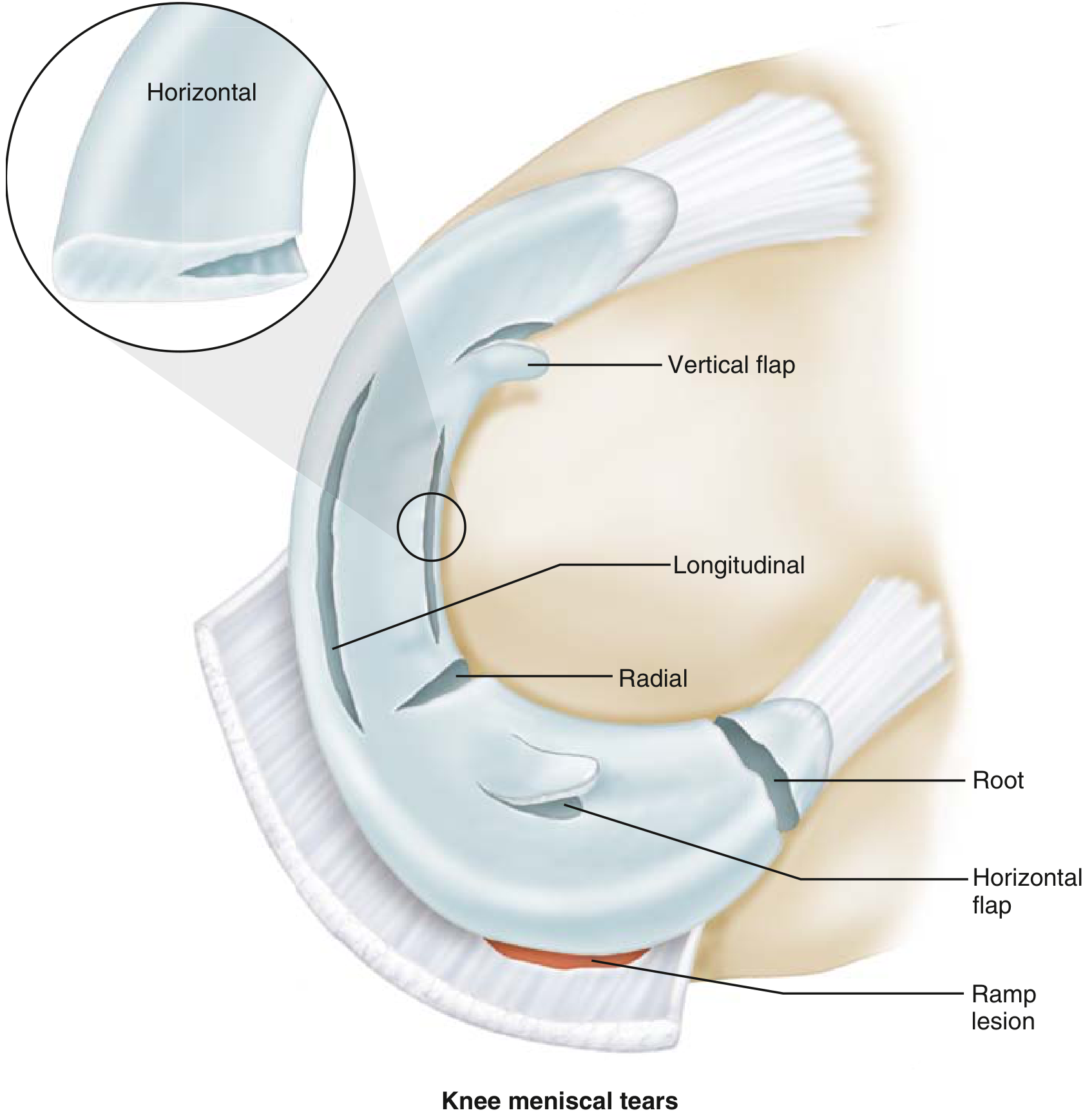
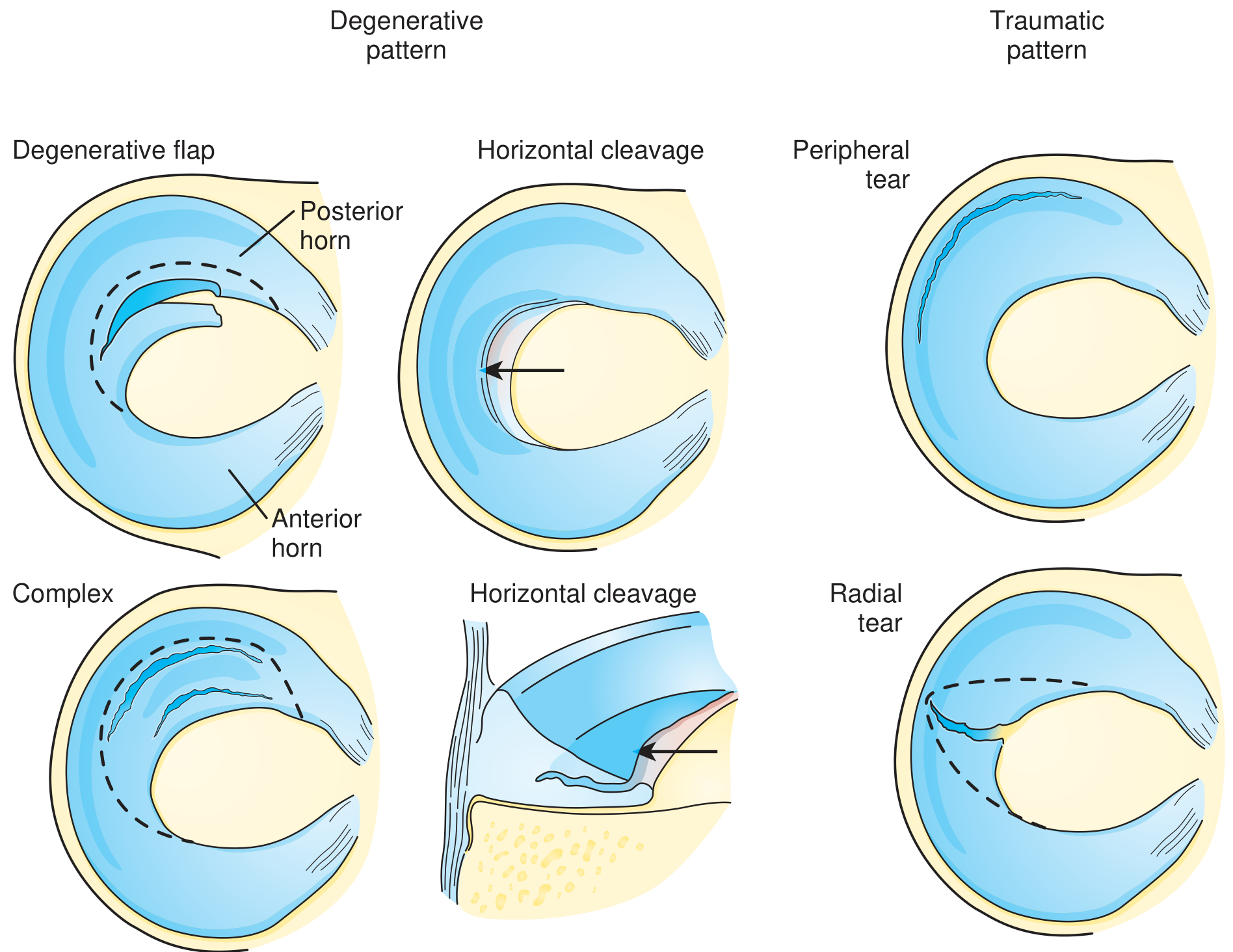
By Orientation
| Type | Description | Typical Context |
|---|---|---|
| Longitudinal (vertical) | Parallel to circumferential fibers; peripheral | Acute trauma in young patients; repairable |
| Bucket-handle | Long longitudinal tear displacing centrally | Young patients; causes locking |
| Radial | Perpendicular to circumferential fibers | Disrupts hoop stress; often not repairable |
| Horizontal cleavage | Splits superior/inferior surfaces | Older, degenerative; associated with meniscal cysts |
| Complex/Degenerative | Multiple planes | Older patients; usually not repairable |
| Root tear | Radial tear or avulsion at tibial attachment | See below |
Meniscal Root Tears
- Defined as a radial tear or avulsion of the meniscal root from the tibial plateau
- Completely disrupts the circumferential (hoop) fibers, abolishing hoop stress
- Biomechanically equivalent to total meniscectomy
- Lateral root tears → associated with ACL tears
- Medial root tears → associated with chondral injuries
- Acute root tears should be repaired whenever possible
— Miller's Review of Orthopaedics, 9th Ed.
Clinical Presentation
- Joint line tenderness (medial or lateral)
- Intermittent locking, clicking, or catching
- Giving way sensation
- Effusion (often delayed)
- Recurrent swelling with activity
Physical Examination
- McMurray test: Knee hyperflexed, varus/valgus stress applied while internally/externally rotating the tibia as the knee is brought to extension. A palpable click + pain = positive (highly indicative of tear)
- Apley grind test, Thessaly test also used
Imaging
MRI is the modality of choice — detects the tear and associated ligamentous/cartilage injuries.
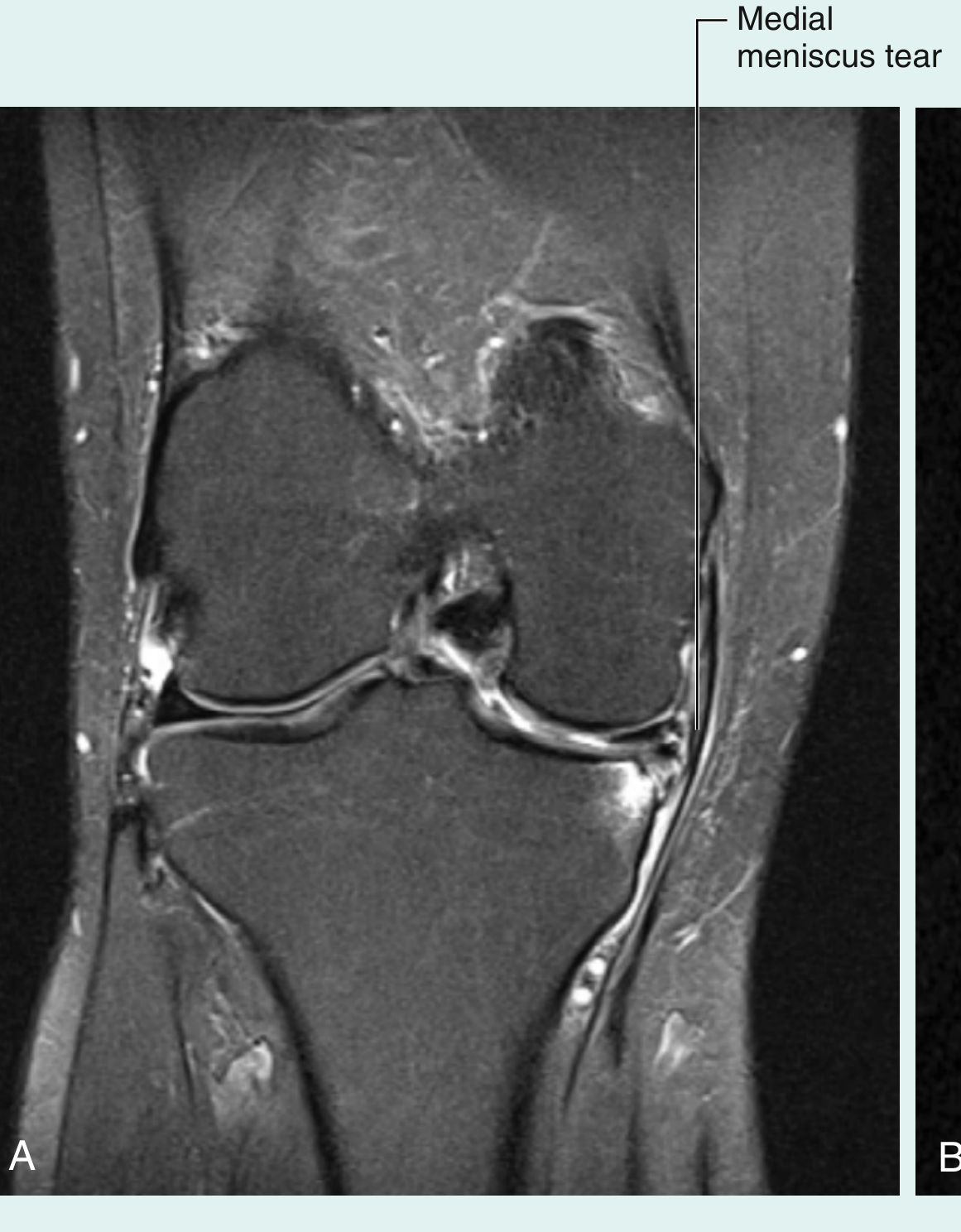
- Plain radiographs and CT cannot diagnose meniscal tears
- Arthroscopy remains the gold standard for diagnosis and is simultaneously therapeutic
Management
Conservative (Non-Operative)
Appropriate for:
- Degenerative tears without mechanical symptoms
- Partial-thickness tears, tears <5–10 mm, or those that cannot be displaced >1–2 mm
- Initial management for all: NSAIDs, activity modification, physiotherapy, ice, corticosteroid injections
In the absence of intermittent swelling, catching, and locking, meniscal tears—particularly degenerative tears—may be treated conservatively. — Miller's Review of Orthopaedics
Surgical Options
1. Partial Meniscectomy
- For tears not amenable to repair (complex, degenerative, central/radial tears)
- Goal: resect minimal normal tissue
- Recovery: weight-bearing as tolerated, return to activities ~3–4 weeks
- Downside: increases peak stresses in the affected compartment → long-term OA risk
2. Meniscal Repair
General indications:
- Tear length 1–4 cm
- Vertical tear orientation
- Red-red zone (vascularized)
- Meniscal root tear
- Patient < 40 years old
- Concomitant ACL reconstruction (extends indications; improves results)
Augmentation techniques (fibrin clot, PRP, vascular access channels, synovial rasping) may extend repair indications into less-vascularized zones.
Surgical Techniques
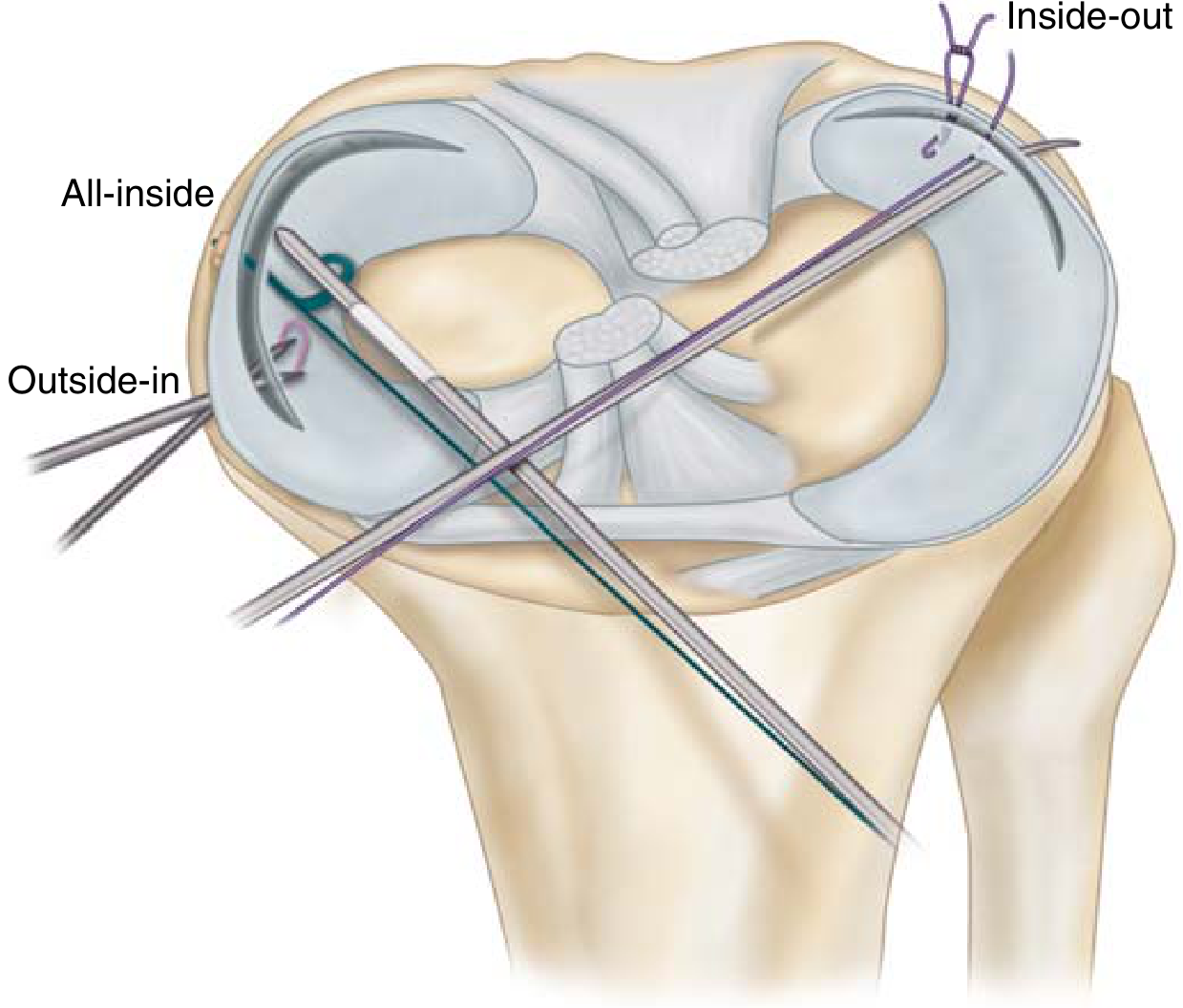
| Technique | Description | Notes |
|---|---|---|
| Open | Direct suture via open incision | Rarely used today |
| Outside-in | Needles passed through skin into joint | Good for anterior tears |
| Inside-out | Cannulas passed through portals; sutures tied externally | Gold standard — vertical mattress sutures |
| All-inside | Entirely intra-articular using implant devices | Most popular due to ease of use; latest generation allows tensioning |
Nerve protection during repair:
- Medial repairs → protect saphenous nerve branches (anterior to semitendinosus/gracilis, posterior to sartorius)
- Lateral repairs → protect peroneal nerve (posterior to biceps femoris)
Outcomes of Repair
| Setting | Success Rate |
|---|---|
| Repair + concurrent ACL reconstruction | ~90% |
| Repair with intact ACL | ~60% |
| Repair with ACL-deficient knee | ~30% |
Recovery after repair: restricted weight-bearing for 3–6 weeks; avoid flexion >90°; return to unrestricted activity in 2–3 months.
— Miller's Review of Orthopaedics, 9th Ed.; Textbook of Family Medicine, 9th Ed.
Special Considerations
Meniscal Cysts
- Primarily associated with horizontal cleavage tears of the lateral meniscus
- Treatment: arthroscopic partial meniscectomy or repair + decompression through the tear
- En bloc excision is no longer favored
Baker (Popliteal) Cysts
- Commonly related to meniscal disorders
- Located between the semimembranosus and medial head of gastrocnemius
- Usually resolve with treatment of the underlying meniscal pathology
Discoid Meniscus
- Congenital variant; lateral meniscus more commonly affected
- May cause "snapping knee syndrome" in children
Recent Evidence
A 2025 systematic review (PMID: 39799406) in American Journal of Sports Medicine found that meniscal repair offers superior biomechanical properties compared to meniscectomy for horizontal meniscal tears — supporting a more aggressive repair-first approach even for tear patterns traditionally treated with resection.
Sources: Miller's Review of Orthopaedics 9th Ed. | Textbook of Family Medicine 9th Ed. | Gray's Anatomy for Students | ROSEN's Emergency Medicine
different meniscal tear on mri
Finding Sources
Finding Sources
Searching Images
meniscal tear MRI types bucket handle radial longitudinal
Reading File
Reading File
Reading File
Searching Images
meniscal root tear MRI extrusion radial
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have all the images and textual content needed. Let me compile the comprehensive answer.
Meniscal Tears on MRI — A Complete Visual Guide
MRI Basics: What You're Looking For
On MRI (best on proton density fat-saturated or T2-weighted sequences), the normal meniscus appears as a homogeneous low-signal (dark) triangular structure. A tear is diagnosed when:
- Increased signal intensity within the meniscus extends to the articular surface (superior or inferior margin)
- Distortion of the normal meniscal morphology
- Discontinuity of the fibrocartilage
Internal "globular" or "linear" high signal that does not reach the surface = intrasubstance degeneration (not a true tear, no surgical significance)
Overview of Tear Types — Anatomy to MRI Correlation
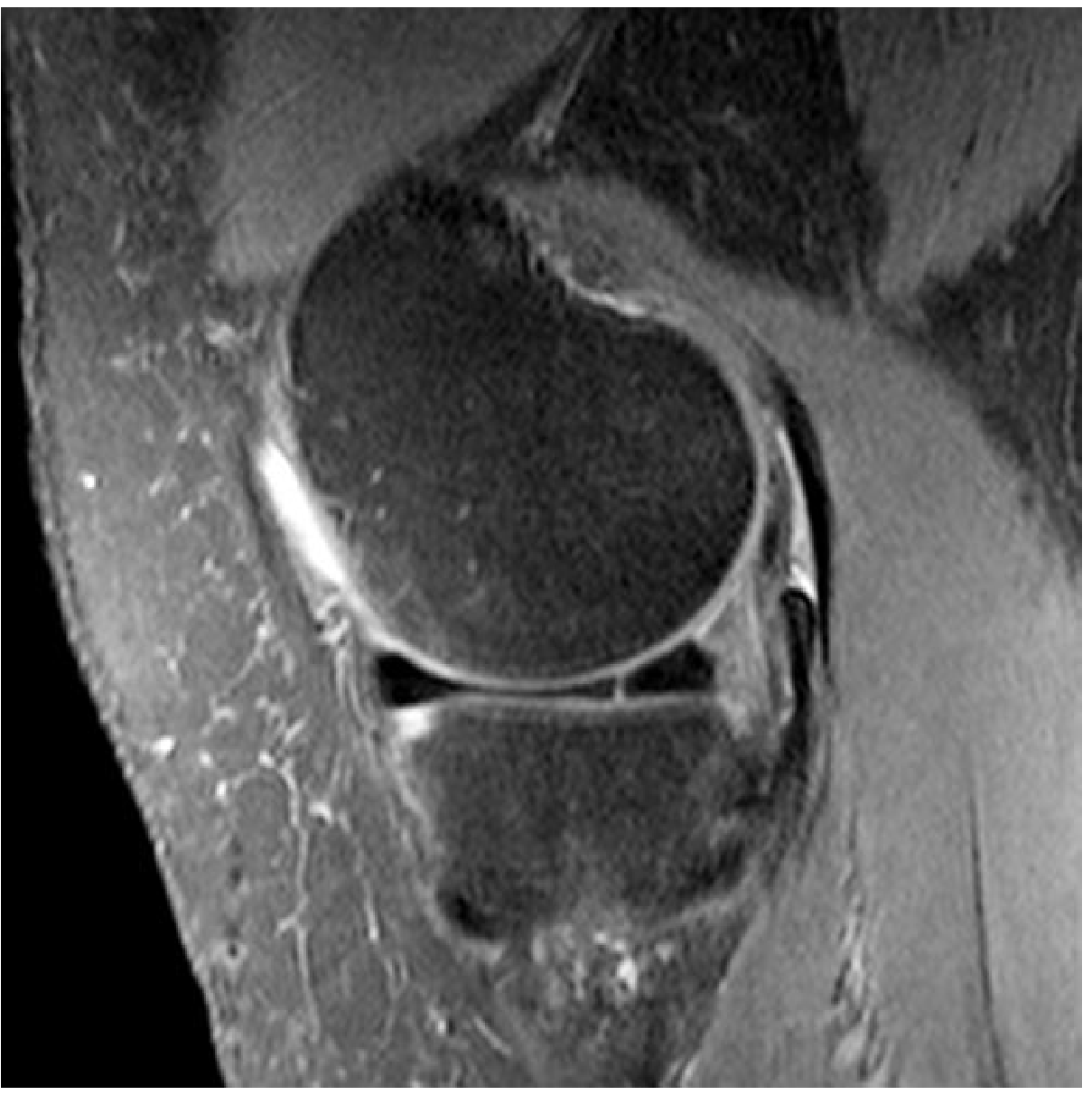
1. Horizontal (Cleavage) Tear
Mechanism: Degenerative; splits the meniscus into superior and inferior leaves parallel to the tibial plateau.
MRI appearance:
- Linear high signal running horizontally through the meniscal substance, extending to the inferior articular surface (or both surfaces)
- Most common in the posterior horn of the medial meniscus
- May be asymptomatic; joint fluid can escape → parameniscal cyst
2. Longitudinal (Vertical) Tear
Mechanism: Acute trauma; tear runs parallel to the circumferential fibers in the periphery (red zone).
MRI appearance:
- Vertical cleft within the peripheral substance of the meniscus on coronal views
- High signal intensity confined to the peripheral third
- Healing potential is better here due to vascular supply

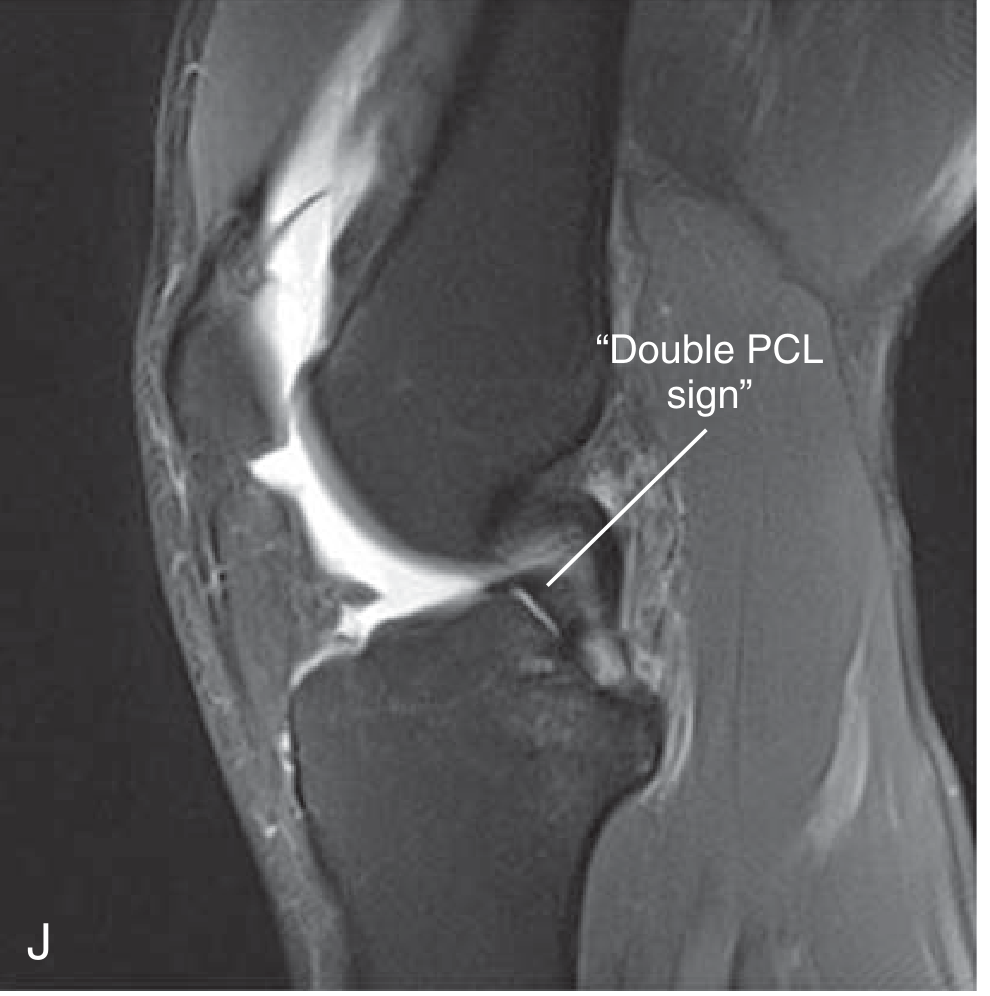
3. Bucket-Handle Tear
A large longitudinal tear in which the inner fragment remains attached at both ends but displaces centrally into the intercondylar notch — like the handle of a bucket flipping inward. The classic cause of acute knee locking.
MRI appearance — key signs:
Double PCL Sign (Sagittal)
The displaced fragment lies in the intercondylar notch anterior and inferior to the PCL, creating a second band paralleling the PCL on sagittal views.
Fragment-in-Notch Sign (Coronal)
Displaced dark low-signal fragment sitting in the intercondylar notch; peripheral meniscus appears truncated.


Double Anterior Horn Sign (Sagittal)
Posterior horn fragment flips anteriorly and lies adjacent to the native anterior horn → two triangular dark structures at the anterior compartment.
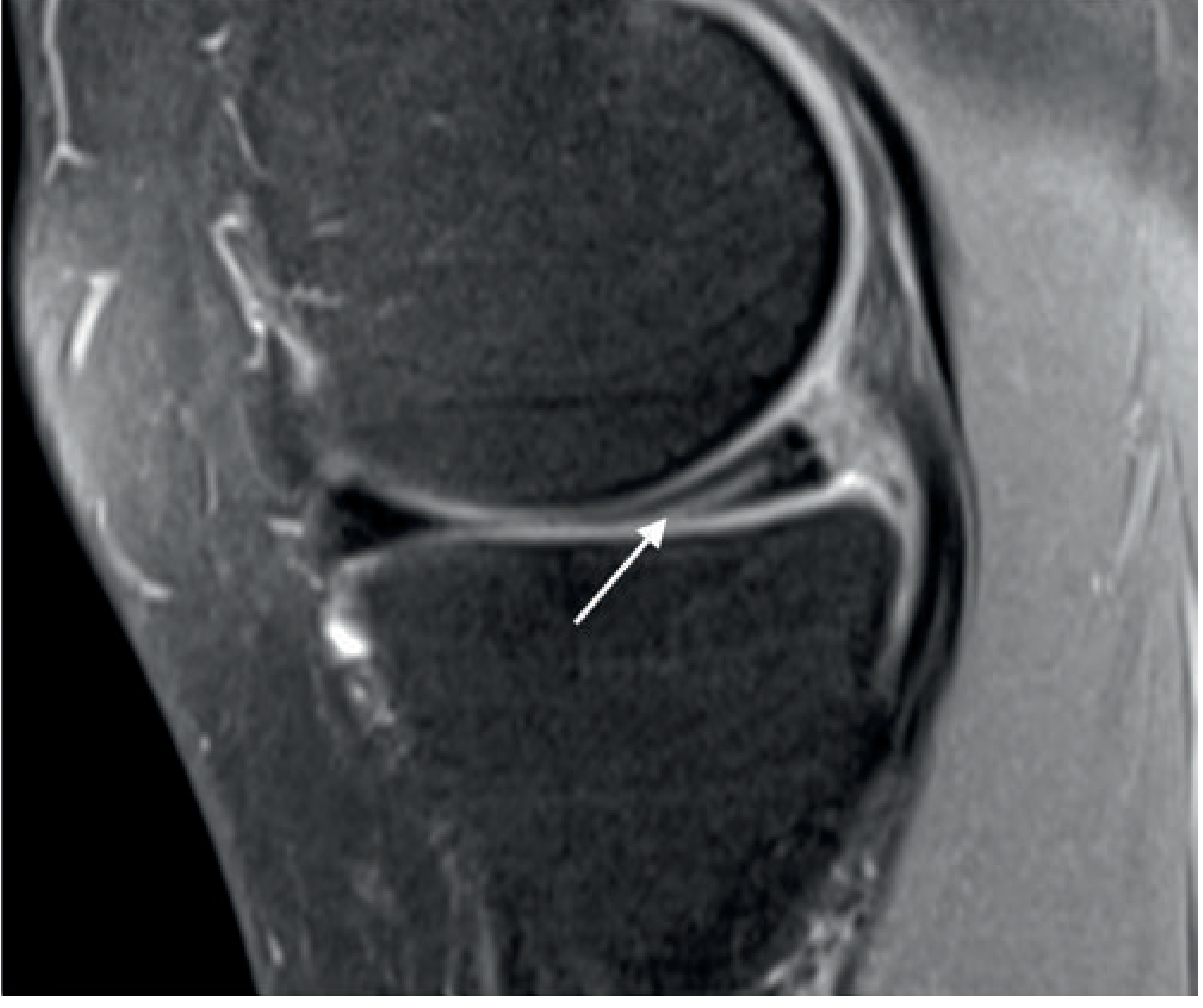
4. Radial Tear
Mechanism: Extends perpendicular to the circumferential fibers from the free inner edge. Disrupts hoop stress.
MRI appearance:
- Sagittal: high-signal "blunting" or truncation of the free edge — the normal pointed triangular shape is lost
- Coronal/axial: focal gap in the meniscal substance
- Complete radial tear → "Ghost Meniscus" sign: the section passes through the gap, showing no meniscal tissue where it should be

Parrot-beak tear = a small oblique radial slit at the free edge; a common variant.
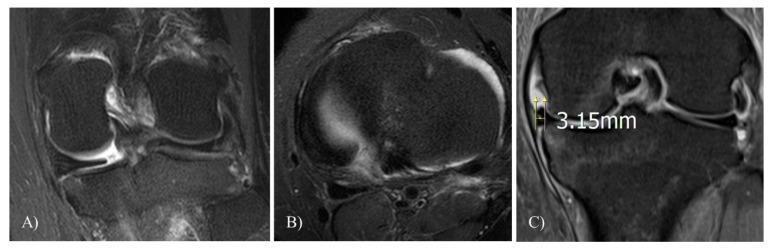
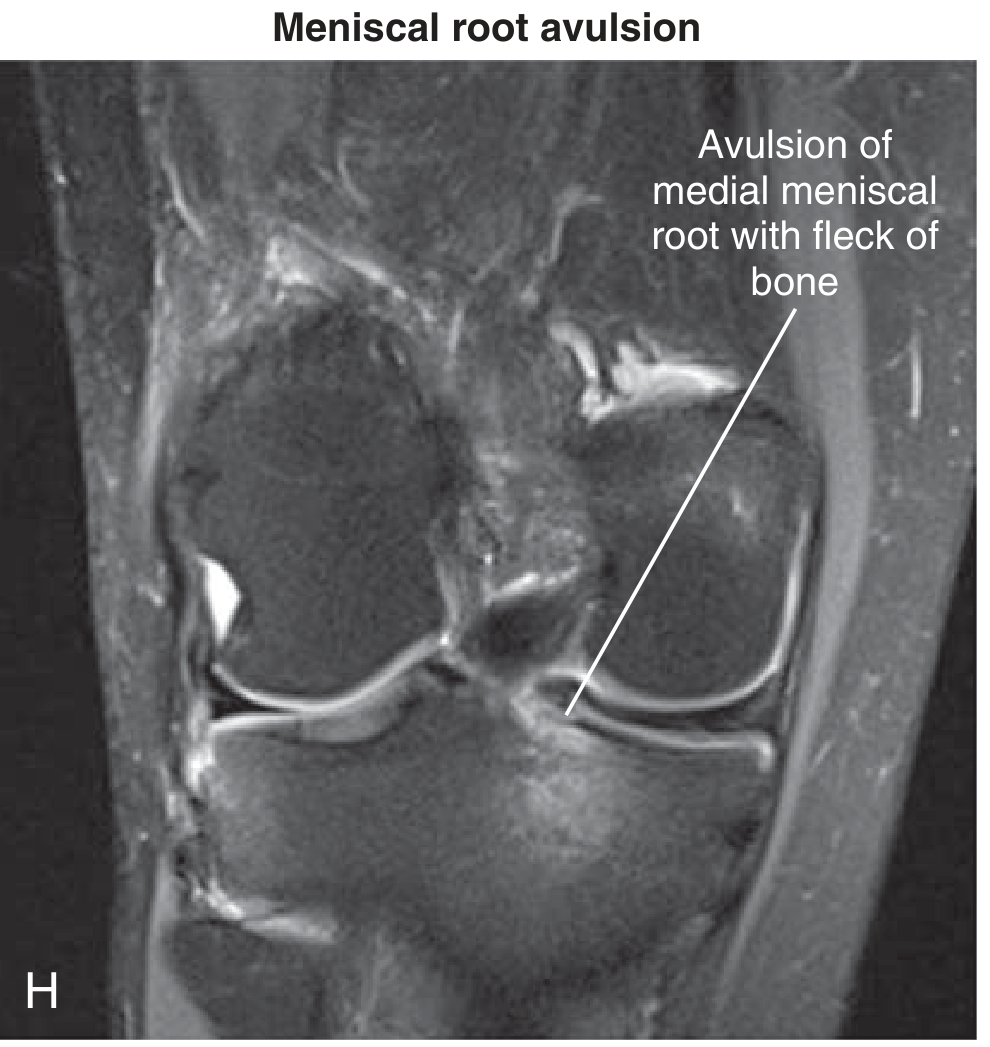
5. Meniscal Root Tear
Definition: Radial tear or avulsion within 1 cm of the tibial root attachment — biomechanically equivalent to total meniscectomy.
MRI appearance:
- Sagittal: "Ghost sign" — absent posterior horn signal where root should anchor
- Coronal + axial: focal high-signal gap at root attachment
- Key secondary finding: meniscal extrusion >3 mm beyond the tibial margin (loss of hoop stress causes the meniscus to be extruded radially)
- Medial root tears: often associated with subchondral marrow edema and cartilage loss
6. Complex / Degenerative Tear
Mechanism: Multi-planar tear in degenerated fibrocartilage; common in older patients.
MRI appearance:
- Diffuse irregular high signal involving multiple planes
- Distorted meniscal morphology
- Often involves the posterior horn of the medial meniscus
- Associated with articular cartilage loss and subchondral edema
Summary Table
| Tear Type | Key MRI Sign | Best Sequence/Plane | Clinical Note |
|---|---|---|---|
| Horizontal | Linear signal to inferior surface | Sagittal PD | Degenerative; may form cyst |
| Longitudinal | Vertical peripheral cleft | Coronal PD | Good healing potential (red zone) |
| Bucket-handle | Double PCL sign; fragment-in-notch; double anterior horn | Sagittal + Coronal | Causes locking; requires repair |
| Radial | Truncated free edge; ghost meniscus | Sagittal + Axial | Disrupts hoop stress; often not repairable |
| Root tear | Ghost sign at root; meniscal extrusion ≥3 mm | Coronal + Axial | Biomechanically = total meniscectomy; repair urgently |
| Complex/Degenerative | Multi-planar irregular signal | All planes | Older patients; partial meniscectomy |
Sources: Grainger & Allison's Diagnostic Radiology | Miller's Review of Orthopaedics 9th Ed. | Imaging Anatomy Vol. 3 (Thieme) | PMC Clinical VQA
meniscal transplantation
Finding Sources
Finding Sources
Searching PubMed
"meniscal allograft transplantation"
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.