Shock
Reading File
Finding Sources
Searching PubMed
"shock" AND "management"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content to write a thorough answer. Let me compile the full response.
Shock
Definition
Shock is a state of circulatory failure that impairs tissue perfusion and leads to cellular hypoxia. At the outset the cellular injury is reversible; however, prolonged shock leads to irreversible tissue injury and death. It may complicate severe hemorrhage, trauma, burns, myocardial infarction, pulmonary embolism, and microbial sepsis.
The current widely accepted definition is "inadequate perfusion of tissue." Oxygen is the most critical nutrient, but blood also carries countless buffers, cells, antibodies, hormones, and antioxins - so thinking in terms of oxygenation alone is an oversimplification.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 134
- Sabiston Textbook of Surgery, p. 563
Classification / Types
| Type | Clinical Examples | Principal Mechanism |
|---|---|---|
| Cardiogenic | MI, ventricular rupture, arrhythmia, cardiac tamponade, pulmonary embolism | Failure of myocardial pump from intrinsic damage, extrinsic compression, or outflow obstruction |
| Hypovolemic | Hemorrhage, vomiting, diarrhea, burns, trauma | Inadequate blood or plasma volume |
| Distributive/Septic | Overwhelming bacterial/fungal infections, SIRS | Cytokine cascades; peripheral vasodilation and blood pooling; endothelial activation/injury; DIC |
| Neurogenic | Spinal cord injury, high spinal anesthesia | Acute vasodilation from loss of sympathetic tone |
| Anaphylactic | IgE-mediated hypersensitivity | Systemic vasodilation + increased vascular permeability |
- Robbins & Kumar Basic Pathology, p. 133
Stages of Shock
Shock is a progressive disorder that evolves through three stages (best characterized in hypovolemic shock but common to all types):
1. Nonprogressive (Compensated) Stage
Reflex compensatory mechanisms activate to maintain vital organ perfusion:
- Baroreceptor reflexes - detect fall in BP
- Catecholamine release - adrenal medulla releases epinephrine/norepinephrine
- Renin-angiotensin-aldosterone axis activation - conserves fluid
- ADH (vasopressin) release - water retention
- Sympathetic stimulation - tachycardia, peripheral vasoconstriction
Net effect: tachycardia, peripheral vasoconstriction, renal fluid conservation. Blood is shunted away from skin to the heart and brain. The skin becomes cool and pale ("shocky" skin). Note: In early septic shock, cutaneous vasodilation may occur instead, presenting with warm, flushed skin.
Laboratory: mild lactate elevation, mild creatinine rise - but no overt organ failure.
2. Progressive (Decompensated) Stage
Compensatory mechanisms are overwhelmed. Widespread tissue hypoxia ensues:
- Aerobic respiration switches to anaerobic glycolysis - excess lactic acid production
- Metabolic lactic acidosis blunts vasomotor response
- Arterioles dilate; blood pools in the microcirculation
- Peripheral pooling worsens cardiac output
- Endothelial cells suffer anoxic injury - risk of DIC
- Vital organs begin to fail
3. Irreversible Stage
Organ injury is permanent regardless of intervention:
-
Widespread cell injury - lysosomal enzyme leakage further aggravates shock
-
Myocardial contractile function worsens (due to increased NO synthesis)
-
Ischemic bowel allows intestinal flora to enter circulation - superimposed bacteremic shock
-
Progressive renal failure
-
Despite best therapy, death follows
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 136
-
Guyton and Hall Textbook of Medical Physiology
-
Harrison's Principles of Internal Medicine 22E, p. 2355
Pathogenesis of Septic Shock
Septic shock is the most clinically important and mechanistically complex form. It is most frequently triggered by gram-positive bacteria, followed by gram-negatives and fungi (SARS-CoV-2 and other emerging viruses can also trigger it).
Key pathogenic mechanisms:
1. Inflammatory response
Microbial PAMPs (pathogen-associated molecular patterns) engage:
- Toll-like receptors (TLRs) on innate immune cells
- G-protein-coupled receptors (bacterial peptides)
- C-type lectin receptors (fungal cell wall, e.g., dectins)
Activation triggers: TNF, IL-1, ROS, prostaglandins, PAF, complement (C3a, C5a, C3b), and fever.
2. Counter-regulatory immunosuppression
The hyperinflammatory state triggers simultaneous immunosuppression - patients may oscillate between hyperinflammatory and immunosuppressed states. Mechanisms include: shift from Th1 to Th2 cytokines, lymphocyte apoptosis, and cellular anergy.
3. Endothelial activation and injury
- Inflammatory cytokines loosen endothelial tight junctions - widespread vascular leakage and tissue edema
- Activated endothelium upregulates NO and vasoactive mediators (C3a, C5a, PAF) causing vascular smooth muscle relaxation and systemic hypotension
- Microvascular dysfunction - heterogeneity of flow, loss of autoregulation, O2 supply-demand mismatch
4. Procoagulant state
- Cytokines increase tissue factor production (monocytes, endothelial cells)
- Decrease in anticoagulant factors: TFPI, thrombomodulin, protein C
- Increased PAI-1 (dampens fibrinolysis)
- Neutrophil extracellular traps (NETs) stimulate both intrinsic and extrinsic coagulation pathways
- Result: DIC in up to 50% of septic patients
5. Metabolic abnormalities
- Insulin resistance and hyperglycemia (driven by TNF, IL-1, stress hormones)
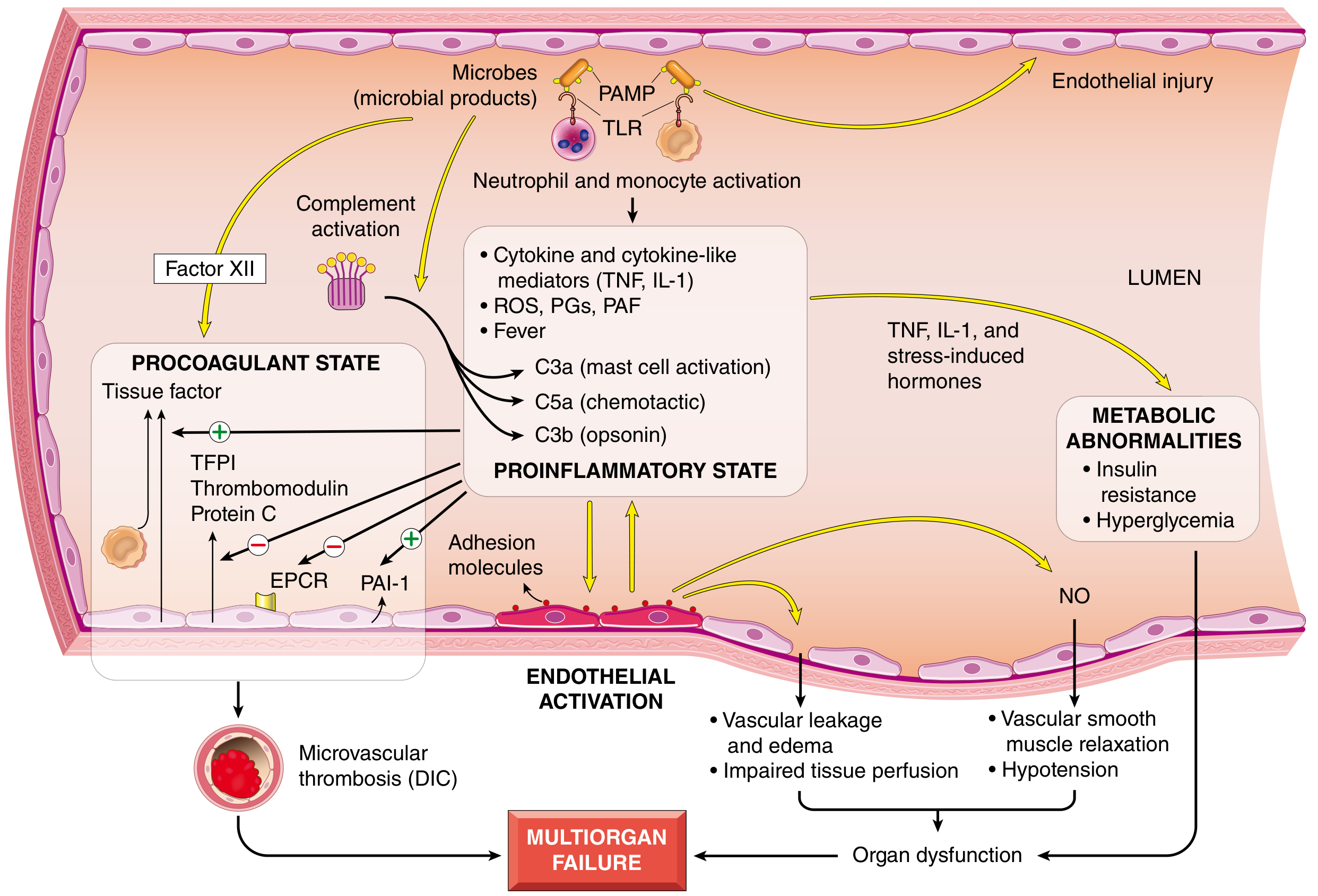
Fig: Major pathogenic pathways in septic shock - Robbins, Cotran & Kumar Pathologic Basis of Disease
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 134-136
Hemorrhagic Shock Classification (ATLS)
The ATLS (Advanced Trauma Life Support) classification divides hemorrhagic shock into four classes based on blood volume lost:
| Class I | Class II | Class III | Class IV | |
|---|---|---|---|---|
| Blood loss (mL) | Up to 750 | 750-1500 | 1500-2000 | >2000 |
| Blood loss (% BV) | Up to 15% | 15-30% | 30-40% | >40% |
| Pulse rate | <100 | >100 | >120 | >140 |
| Blood pressure | Normal | Normal | Decreased | Decreased |
| Pulse pressure | Normal/increased | Decreased | Decreased | Decreased |
| Respiratory rate | 14-20 | >20-30 | 30-40 | >35 |
| Urine output (mL/h) | >30 | >20-30 | 5-15 | Negligible |
| CNS/mental status | Slightly anxious | Mildly anxious | Anxious + confused | Confused + lethargic |
Key notes:
-
About 10% blood volume can be removed with almost no effect on arterial pressure or cardiac output
-
40-45% blood volume loss causes cardiac output and BP to fall to zero
-
In the absence of sympathetic reflexes, only 15-20% loss causes death; with reflexes intact, 30-40% loss can be tolerated
-
Schwartz's Principles of Surgery, p. 220
Morphology (Organ Changes in Shock)
The cellular and tissue effects of shock are those of hypoxic injury, caused by hypoperfusion + microvascular thrombosis. Any organ can be affected, but the most commonly involved are:
| Organ | Change |
|---|---|
| Brain | Encephalopathy (hypoxic injury) |
| Heart | Subendocardial hemorrhage and necrosis |
| Kidneys | Acute tubular necrosis (ATN) - most common cause of acute kidney injury |
| Adrenals | Cortical cell lipid depletion (increased steroid synthesis) |
| GI tract | Hemorrhagic enteropathy; ischemic bowel - risk of bacterial translocation |
| Lungs | "Shock lung" (diffuse alveolar damage) - in septic or traumatic shock; lungs are relatively resistant in pure hypovolemic shock |
Fibrin thrombi most readily seen in kidney glomeruli. Except for neuronal and cardiomyocyte loss, affected tissues can recover completely if the patient survives.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 136
Clinical Features
| Type of Shock | Skin | Pulse | BP | Other |
|---|---|---|---|---|
| Hypovolemic | Cool, clammy, cyanotic | Weak, rapid | Low | Tachypnea |
| Cardiogenic | Cool, clammy, cyanotic | Weak, rapid | Low | Signs of heart failure (JVD, pulmonary edema) |
| Septic (early) | Warm, flushed | Bounding | Low | Fever, leukocytosis |
| Septic (late) | Cool, clammy | Weak, rapid | Low | Multiorgan failure |
| Neurogenic | Warm, dry | Slow (bradycardia) | Low | History of spinal injury |
| Anaphylactic | Urticaria, flushing | Rapid | Low | Bronchospasm, angioedema |
Management Principles
The key priorities in managing shock (per Harrison's 22E):
- Recognize shock early - high clinical suspicion for any new organ dysfunction or hypotension
- Assess the type of shock - the etiology determines specific therapy
- Initiate therapy simultaneously with evaluation
- Aim: restore oxygen delivery to tissues
Response to fluid resuscitation (hypovolemic/hemorrhagic shock):
- Responders - vital signs normalize; no ongoing hemorrhage
- Transient responders - improve initially but deteriorate; significant ongoing hemorrhage
- Non-responders - persistent hypotension; require immediate source control
A base deficit > 8 mmol/L implies ongoing cellular shock.
Resuscitation fluids:
- Crystalloids (normal saline, Lactated Ringer's) - widely used but poorly retained in vascular space (only ~175-200 mL of a 1L infusion remains intravascular after a few hours)
- Blood products are essential in hemorrhagic shock - whole blood or packed RBCs restore volume and oxygen-carrying capacity
Specific interventions by type:
-
Hypovolemic: IV fluids, blood transfusion, hemorrhage control
-
Cardiogenic: Inotropes (dobutamine), vasopressors (norepinephrine), treat underlying cause (PCI for MI, drainage for tamponade)
-
Septic: Antibiotics (broad-spectrum, early), source control, vasopressors (norepinephrine first-line), IV fluids (30 mL/kg crystalloid initial bolus)
-
Anaphylactic: Epinephrine IM is the cornerstone; antihistamines, corticosteroids, IV fluids
-
Neurogenic: Volume resuscitation, vasopressors (phenylephrine, norepinephrine)
-
Harrison's Principles of Internal Medicine 22E
-
Sabiston Textbook of Surgery
Recent Evidence Update
The Surviving Sepsis Campaign 2026 pediatric guidelines (PMID 41869844) provide updated management for septic shock in children. A 2024 meta-analysis in JAMA (PMID 38864162) found that prolonged/extended infusions of beta-lactam antibiotics are associated with improved outcomes in sepsis/septic shock compared to intermittent dosing - a meaningful update for clinical practice.
Summary mnemonic for types of shock: "He Doesn't Stop Necrotizing Arterioles"
- Hypovolemic
- Distributive (septic, anaphylactic, neurogenic)
- Septic (subset of distributive)
- Neurogenic
- Anaphylactic (+ Cardiogenic + Obstructive)
This is a shared conversation. Sign in to Orris to start your own chat.