Hiv or aids full details
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Here is a comprehensive, authoritative overview of HIV/AIDS, drawn from Harrison's Principles of Internal Medicine 22E (2025), Robbins & Kumar Pathologic Basis of Disease, Medical Microbiology 9e, and Textbook of Family Medicine 9e.
HIV / AIDS — Complete Overview
1. What Is HIV?
Human Immunodeficiency Virus (HIV) is an RNA retrovirus belonging to the family Retroviridae, subfamily Lentiviridae. Its RNA genome is reverse-transcribed into DNA and permanently integrated into the host cell genome. Two types exist:
- HIV-1 — responsible for the global pandemic; four groups (M, N, O, P), with Group M divided into 11 subtypes/clades (A–K)
- HIV-2 — less virulent, primarily in West Africa; lacks the vpu gene, has a vpx gene instead
AIDS (Acquired Immunodeficiency Syndrome) is the end-stage of untreated HIV infection, defined by:
- CD4+ T cell count < 200 cells/μL, OR
- Diagnosis of one or more AIDS-defining opportunistic illnesses (CDC Stage C/Stage 3)
"HIV disease is a spectrum ranging from primary infection… to the relatively asymptomatic stage, to advanced stages associated with opportunistic diseases." — Harrison's Principles of Internal Medicine 22E
2. Virology & Structure
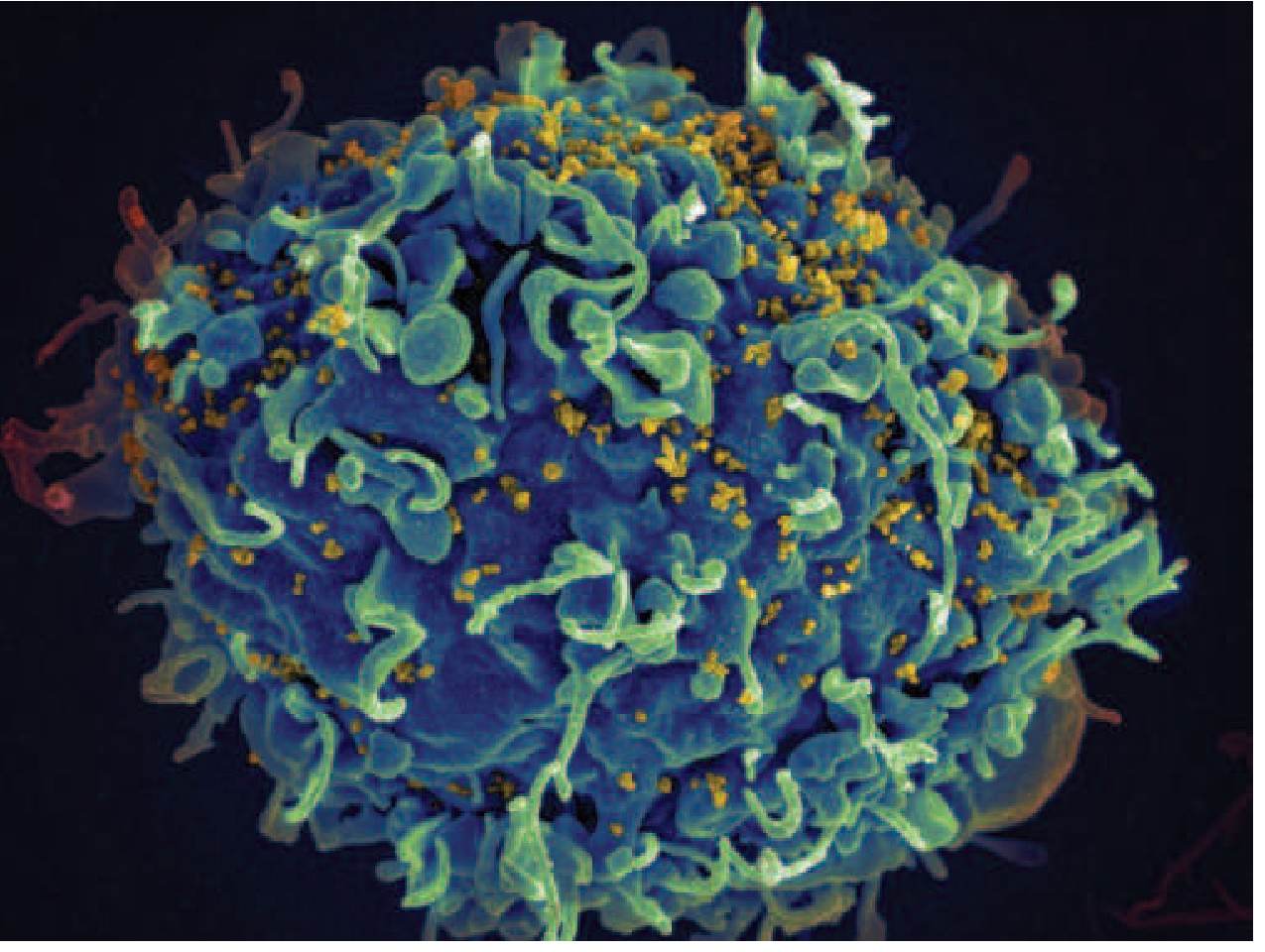
Scanning electron micrograph: HIV-1 virus particles (yellow) budding off a CD4+ T cell (blue). Courtesy of NIAID — Harrison's 22E
Key structural components:
| Component | Function |
|---|---|
| gp120 | Envelope glycoprotein; binds CD4 receptor |
| gp41 | Transmembrane glycoprotein; mediates membrane fusion |
| p24 | Core capsid protein; detected by 4th-generation tests |
| Reverse transcriptase | Converts viral RNA → DNA (error-prone; drives mutation) |
| Integrase | Integrates proviral DNA into host genome |
| Protease | Cleaves polyproteins into functional viral proteins |
Key regulatory genes: tat, rev, nef, vif, vpr, vpu — modulate host cell and viral gene expression, enhance pathogenicity.
The virus mutates at ~10⁷ mutations/minute during replication, making strict multi-drug ART essential to prevent resistance.
3. Epidemiology
- ~39 million people worldwide living with HIV (2022)
- ~630,000 deaths attributed to HIV/AIDS in 2022
- ~67% of all cases in Sub-Saharan Africa
- ~50,000 new infections per year in the United States
- ~50% of HIV-infected persons worldwide are unaware of their infection
- Disproportionately affects African Americans, Hispanics/Latinos in the US
— Harrison's Principles of Internal Medicine 22E; Textbook of Family Medicine 9e
4. Transmission
HIV is transmitted by:
| Route | Details |
|---|---|
| Sexual contact | Most common globally; risk increased by genital ulcers (syphilis, HSV, chancroid), other STIs (gonorrhea, chlamydia), high viral load, uncircumcised status |
| Blood exposure | Sharing needles/syringes (IV drug use), blood transfusions, needle-stick injuries |
| Mother-to-child (vertical) | During pregnancy, labor/delivery, or breastfeeding |
Critical principle — U=U (Undetectable = Untransmittable): When viral load is suppressed to < 20 copies/mL on ART, there is essentially zero risk of sexual transmission. This has been confirmed in multiple large RCTs.
Risk factors for increased transmission:
- High plasma viral load (strongest predictor)
- Presence of genital ulcer disease
- Uncircumcised male
- Concurrent STIs (chlamydia, gonorrhea, trichomoniasis)
5. Pathogenesis
Primary Target Cells
HIV has tropism for CD4-expressing cells:
- CD4+ T lymphocytes (especially memory T cells)
- Monocytes and macrophages
- Dendritic cells (DCs) and Langerhans cells
- Microglial cells (CNS)
How HIV Enters Cells
- gp120 binds to the CD4 receptor on the host cell surface
- Co-receptor binding occurs — either CCR5 (M-tropic/R5 virus, early infection) or CXCR4 (T-tropic/X4 virus, late disease)
- gp41 mediates membrane fusion, allowing viral core entry
- Reverse transcriptase converts viral RNA → double-stranded DNA
- Integrase inserts proviral DNA permanently into the host genome
CCR5-Δ32 mutation: Individuals homozygous for this mutation lack surface CCR5 and are resistant to HIV infection (~1% of northern Europeans). CCR5 is the target of the drug maraviroc.
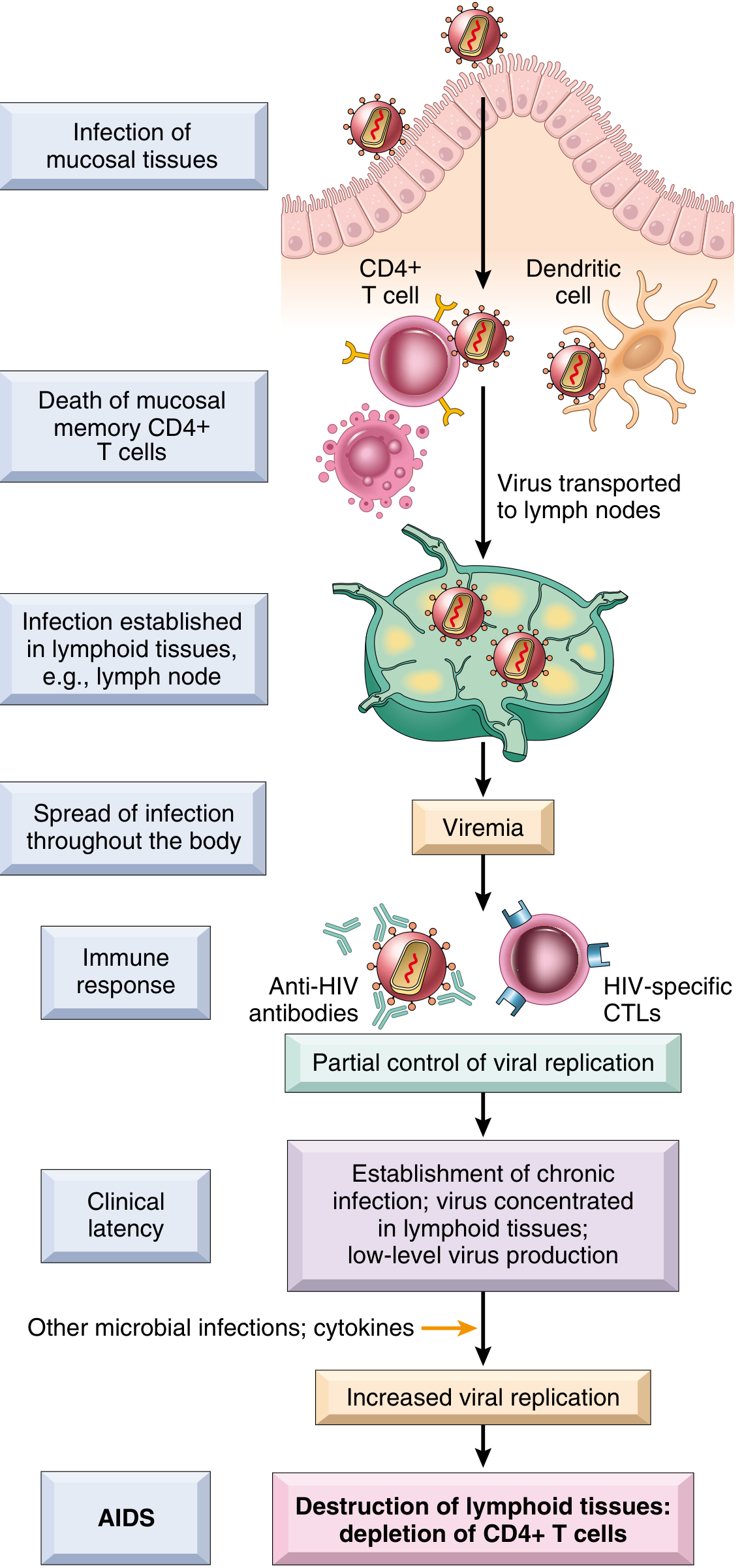
Pathogenesis of HIV-1 infection — Robbins & Kumar Pathologic Basis of Disease
Mechanisms of CD4+ T Cell Destruction
- Direct lytic infection — virus kills activated permissive CD4 T cells
- Apoptosis — induced in non-permissive bystander cells
- Syncytia formation — gp120 on infected cells binds CD4 on uninfected cells → giant cells that die within hours (mainly X4 virus)
- CTL-mediated killing — HIV-specific CD8+ T cells destroy infected cells
- Latent reservoir — integrated provirus in long-lived memory CD4 T cells and germinal center follicular helper T cells persists indefinitely despite ART
Consequences of CD4 Depletion
- Loss of Th1-type cell-mediated immunity → susceptibility to intracellular organisms
- Loss of T-cell help for B cells → impaired humoral responses to new antigens
- Macrophage dysfunction → decreased phagocytosis and antigen presentation
- Gut CD4 T cell depletion → disruption of mucosal barrier → microbial translocation, diarrhea
CNS Involvement (HAND)
HIV enters the CNS via infected macrophages ("Trojan horse"). Infected microglia release neurotoxic cytokines (IL-1, TNF, IL-6), nitric oxide (via gp41), and soluble gp120 → HIV-Associated Neurocognitive Disorder (HAND). Neurons themselves are not directly infected.
6. Natural History & Clinical Stages
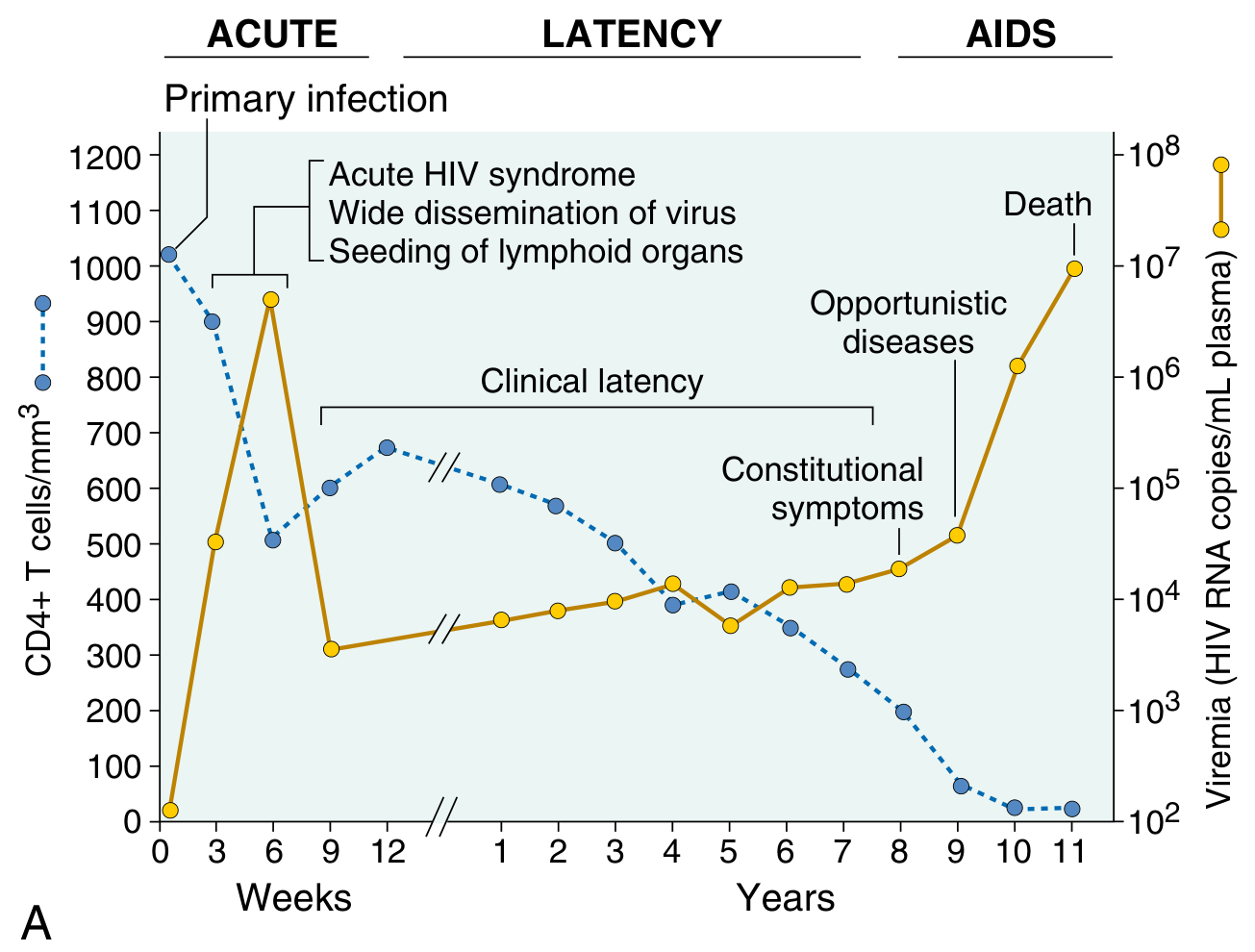
Clinical course of HIV — CD4 count falling, viral load rising to AIDS stage — Robbins & Kumar
Phase 1: Acute Retroviral Syndrome (weeks 1–6)
- High-level viremia with rapid dissemination to lymphoid tissue
- Occurs in 40–90% of patients
- Presents as: flu-like illness, maculopapular rash, fever, lymphadenopathy, pharyngitis, myalgia, aseptic meningitis, or heterophile-negative mononucleosis-like syndrome
- CD4 count drops sharply, then partially recovers
- Host immune response (CTLs + antibodies) partially controls viremia → viral "set point" established
Phase 2: Clinical Latency (months to years)
- Usually asymptomatic but fully infectious
- CD4 count gradually declines (~50–100 cells/μL per year without ART)
- Viral load stable at set point
- Duration: median ~10 years (range: months to >15 years)
- Later: constitutional symptoms — night sweats, weight loss, fatigue, generalized lymphadenopathy
Phase 3: AIDS (CD4 < 200 cells/μL or AIDS-defining illness)
- Severe immunosuppression → opportunistic infections and tumors
7. AIDS-Defining Conditions (CDC Stage C / Stage 3)
| Category | Examples |
|---|---|
| Fungal | Pneumocystis jirovecii pneumonia (PCP), esophageal/pulmonary candidiasis, cryptococcosis, histoplasmosis, coccidioidomycosis |
| Mycobacterial | M. tuberculosis (any site), M. avium complex (MAC), disseminated |
| Viral | CMV retinitis/disease, HSV chronic ulcers (>1 month), progressive multifocal leukoencephalopathy (PML) |
| Protozoal | Toxoplasmosis of brain, cryptosporidiosis (chronic), isosporiasis |
| Bacterial | Recurrent bacterial pneumonia, recurrent Salmonella septicemia |
| Neoplastic | Kaposi's sarcoma, Burkitt's lymphoma, immunoblastic lymphoma, primary CNS lymphoma, invasive cervical cancer |
| Other | HIV encephalopathy, wasting syndrome |
8. Diagnosis
Screening
- 4th-generation HIV Ag/Ab immunoassay (recommended): detects both p24 antigen and HIV antibodies; window period ~6–7 days post-infection
- Rapid tests: results in < 20 minutes; CLIA-waived
- Viral load (HIV RNA PCR): used to detect acute infection before seroconversion; required for monitoring
CDC Recommended Testing
Voluntary opt-out HIV testing in all healthcare settings for persons aged 13–64 years.
Test when patient presents with:
- STDs
- Constitutional symptoms (fever, night sweats, weight loss)
- Oral thrush (oropharyngeal candidiasis)
- Herpes zoster in persons < 50 years
- Asymptomatic generalized lymphadenopathy
- Oral hairy leukoplakia
Staging by CD4 Count (Adults ≥ 6 years)
| Stage | CD4 Count |
|---|---|
| Stage 1 | ≥ 500 cells/μL |
| Stage 2 | 200–499 cells/μL |
| Stage 3 (AIDS) | < 200 cells/μL |
9. Antiretroviral Therapy (ART)
ART is the cornerstone of HIV management and should be initiated as soon as possible after diagnosis — regardless of CD4 count.
Exception: In cryptococcal meningitis or TB, stabilize with specific antimicrobials for several weeks before starting ART (to reduce risk of severe immune reconstitution inflammatory syndrome/IRIS).
Drug Classes
| Class | Mechanism | Examples |
|---|---|---|
| NRTIs (Nucleoside/Nucleotide Reverse Transcriptase Inhibitors) | Competitive inhibition of reverse transcriptase | Tenofovir (TDF/TAF), Emtricitabine (FTC), Lamivudine (3TC), Abacavir (ABC) |
| NNRTIs (Non-Nucleoside RTIs) | Non-competitive allosteric inhibition of RT | Efavirenz, Rilpivirine, Doravirine |
| PIs (Protease Inhibitors) | Inhibit viral protease; boosted with ritonavir or cobicistat | Darunavir, Atazanavir, Lopinavir |
| INSTIs (Integrase Strand Transfer Inhibitors) | Block integration of proviral DNA | Dolutegravir, Bictegravir, Raltegravir, Cabotegravir |
| Fusion Inhibitors | Block gp41-mediated membrane fusion | Enfuvirtide |
| CCR5 Antagonists | Block CCR5 co-receptor | Maraviroc |
| CD4 Attachment Inhibitors | Block gp120 binding to CD4 | Fostemsavir |
| Capsid Inhibitors | Interfere with viral capsid assembly/uncoating | Lenacapavir |
Standard Regimen
A typical first-line regimen: 2 NRTIs + 1 INSTI (e.g., Bictegravir/Tenofovir AF/Emtricitabine as a single daily pill — Biktarvy).
Two-drug regimen: Dolutegravir + 3TC is approved for initial therapy in Hep B-negative patients with viral load < 500,000 copies/mL.
Long-Acting Injectable ART
Cabotegravir/rilpivirine (Cabenuva) — given every 1–2 months by injection; improves adherence.
Goals of ART
- Suppress viral load to < 20 copies/mL (undetectable)
- Restore and preserve CD4+ T cell counts
- Prevent opportunistic infections and AIDS-defining events
- Prevent transmission (U=U)
- Approach near-normal life expectancy
10. Immune Abnormalities in AIDS
| System | Abnormality |
|---|---|
| T cells | Lymphopenia; preferential loss of activated/memory CD4+ T cells; decreased delayed-type hypersensitivity; reduced IL-2, IFN-γ |
| B cells | Polyclonal activation → hypergammaglobulinemia; paradoxically cannot mount de novo antibody responses |
| Monocytes/Macrophages | Decreased chemotaxis, phagocytosis, Class II HLA expression, antigen presentation |
— Robbins & Kumar Pathologic Basis of Disease
11. Opportunistic Infection Prophylaxis
| CD4 Threshold | Prophylaxis |
|---|---|
| < 200 cells/μL | TMP-SMX for PCP (also covers toxoplasmosis) |
| < 100 cells/μL | TMP-SMX for toxoplasmosis |
| < 50 cells/μL | Azithromycin for MAC |
| All patients | Annual influenza; pneumococcal vaccine; consider TB testing |
12. Prevention
| Strategy | Details |
|---|---|
| U=U / TasP | Viral suppression on ART eliminates sexual transmission |
| PrEP (Pre-Exposure Prophylaxis) | Tenofovir/emtricitabine (daily oral or injectable cabotegravir) for HIV-negative at-risk persons; > 99% effective |
| PEP (Post-Exposure Prophylaxis) | 28-day ART regimen initiated within 72 hours of exposure |
| Condoms | Correct and consistent use is highly effective |
| Male circumcision | Reduces HIV acquisition in heterosexual men (~50–60% in RCTs); protective via reduced Langerhans/CD4 cell density in foreskin |
| Needle/syringe programs | Prevent bloodborne transmission among PWID |
| PMTCT | ART during pregnancy + neonatal prophylaxis + avoiding breastfeeding (where safe) eliminates mother-to-child transmission |
| Treat STIs | Reduces HIV transmission in low-prevalence settings |
13. Prognosis
- Without ART: median survival from AIDS diagnosis ~2–3 years
- With modern ART: life expectancy approaches that of HIV-negative individuals
- Success with ART exceeds outcomes for most adult cancers or complications of coronary artery disease
- UNAIDS "95-95-95" target (by 2030): 95% know their status → 95% on ART → 95% virally suppressed
"ART transformed HIV infection from an inescapably fatal disease into a manageable chronic illness." — Harrison's Principles of Internal Medicine 22E (2025)
Sources:
- Harrison's Principles of Internal Medicine 22E (2025, McGraw-Hill)
- Robbins & Kumar Pathologic Basis of Disease (Elsevier)
- Medical Microbiology 9e (Murray et al.)
- Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.