Laryngomalacia history taking and clinical examination for one month baby
Reading File
Finding Sources
Finding Sources
Searching PubMed
laryngomalacia neonates diagnosis clinical
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, authoritative content from three major otolaryngology textbooks plus endoscopic images. Here is a thorough, structured response:
Laryngomalacia in a 1-Month-Old: History Taking & Clinical Examination
Laryngomalacia (LM) is the most common cause of neonatal stridor, accounting for approximately 75% of cases of infantile stridor. It results from partial or complete collapse of the supraglottic structures on inspiration, likely due to neuromuscular and structural immaturity of the larynx.
HISTORY TAKING
1. Presenting Complaint
- Onset of stridor: Ask when the noisy breathing was first noticed. In LM, inspiratory stridor typically appears within the first 2 weeks of life (often day 1-2 of life, or shortly after birth).
- Nature of the sound: High-pitched, fluttering inspiratory noise (sometimes described as a "squeaky" or "crowing" sound). Compared to vocal cord paralysis, it is often relatively low-pitched and lacks a musical quality.
2. Aggravating & Relieving Factors
| Factor | Effect in LM |
|---|---|
| Activity / agitation / crying | Worsens stridor (mild-moderate LM) |
| Feeding | Worsens (increased respiratory effort) |
| Supine position | Worsens (gravity pulls supraglottic tissues into airway) |
| Prone / neck extension | Improves (lifts epiglottis away from airway) |
| Sleep | Often improves or disappears |
| Mild-moderate LM + crying | May improve (increased pharyngeal tone) |
| Severe LM + crying | Worsens (increased airflow through collapsed larynx) |
3. Feeding History (critical in a 1-month-old)
- Does the baby tire quickly during feeds?
- How long does feeding take? (prolonged feeds >30 min are concerning)
- Does the baby need to stop and breathe during feeds?
- Any coughing, choking, or gagging during/after feeds?
- Any regurgitation or vomiting after feeds? (suggests GORD, which co-exists in the majority of LM cases)
- Breast vs. bottle fed? (bottle feeding may be better tolerated)
- Current weight and whether gaining appropriately - ask birth weight vs. current weight
- Any failure to thrive?
4. Severity Indicators - "Red Flag" Symptoms
Ask directly about:
- Cyanotic episodes or colour changes (blue/grey) during feeds or at rest
- Apnoea - pauses in breathing
- Severe chest retractions visible to parents
- Difficulty sleeping / sleep-disordered breathing
- Cardiorespiratory distress at rest (suggests severe LM requiring urgent intervention)
5. Positional History
- Does the baby breathe better in any particular position?
- Has the parent noticed improvement when baby is held upright or in prone position?
6. Birth & Antenatal History
- Gestation: Premature infants (especially Hispanic and Black infants) are at higher risk
- Birth weight, delivery method (instrumental delivery - risk of nerve injury)
- Neonatal resuscitation required? (intubation history - raises risk of subglottic stenosis as alternative diagnosis)
- NICU admission?
- Any antenatal abnormalities on scan?
7. Neurological & Developmental History
- Any known neurological diagnosis (cerebral palsy, hypotonia, Chiari malformation)? - LM may be associated with neuromuscular disorders
- Is the baby alert, fixing and following?
- Any other dysmorphic features? (syndromes such as Down's syndrome are associated)
8. Family & Social History
- Family history of airway problems
- Passive smoke exposure
- Who are the main caregivers and their level of anxiety/coping
9. Systems Review
- Any concurrent upper respiratory tract infections?
- Noisy breathing from the nose (choanal stenosis as co-existing lesion)?
- Drooling?
- Episodes of colour change?
CLINICAL EXAMINATION
General Inspection
- Overall appearance: Well vs. unwell, alert, colour (pink vs. mottled/cyanosed)
- Nutritional status: Assess for signs of failure to thrive - subcutaneous fat, muscle bulk
- Dysmorphic features: Down syndrome, Pierre Robin sequence, CHARGE syndrome (associated with LM)
- Work of breathing at rest: Is the baby comfortable or in distress?
Vital Signs
- Respiratory rate (normal in a 1-month-old: 30-60/min)
- Oxygen saturations (SpO2) - critical to assess
- Heart rate
- Weight - plot on centile chart; compare with birth weight
Respiratory Examination
Inspection
- Character of stridor: Confirm it is inspiratory (LM is purely inspiratory; biphasic stridor suggests subglottic/tracheal pathology)
- Sternal and intercostal recession: Mild recession is common in mild LM; severe recession is a red flag indicating significant obstruction
- Subcostal recession
- Suprasternal notch indrawing
- Nasal flaring
- Tracheal tug
- Abdominal breathing / paradoxical chest movement (in severe obstruction)
Auscultation
- Air entry: Equal and clear bilaterally? (unequal raises suspicion of vascular ring, mass, or other lesion)
- Listen over neck - stridor loudest over the larynx
- Any wheeze (suggests lower airway component - GOR-related / bronchomalacia)?
- Any crackles (aspiration pneumonia from feeding difficulties)?
Effect of Position
- Observe stridor in supine vs. prone - improvement in prone is characteristic of LM
Cardiovascular Examination
- Heart sounds, murmurs - exclude congenital heart disease contributing to respiratory distress
- Check femoral pulses, capillary refill time
Abdominal Examination
- Hepatomegaly (cardiac failure)?
- Signs of GORD: abdomen soft, no masses
Oropharyngeal Examination
- Inspect oral cavity for cleft palate, micrognathia (Pierre Robin)
- Tongue size (macroglossia in hypothyroidism / Beckwith-Wiedemann)
Neurological Assessment
- Tone: Hypotonia is associated with LM (neuromuscular immaturity theory)
- Primitive reflexes: suck, rooting, Moro
- Level of alertness and interaction
ENT-Specific Examination
- Nose: Patent nasal passages bilaterally (pass suction catheter or observe fogging of mirror)
- Ears: Basic otoscopy if possible
ENDOSCOPIC ASSESSMENT (Gold Standard)
The definitive diagnosis requires endoscopic examination. This is done in the outpatient setting with awake flexible fibre-optic nasolaryngoscopy (nasendoscopy):
"The child should be wrapped in a blanket and held firmly by a nurse or parent. The supraglottic collapse on inspiration, which is typical of laryngomalacia, is easily seen."
- Scott-Brown's Otorhinolaryngology, Vol 2
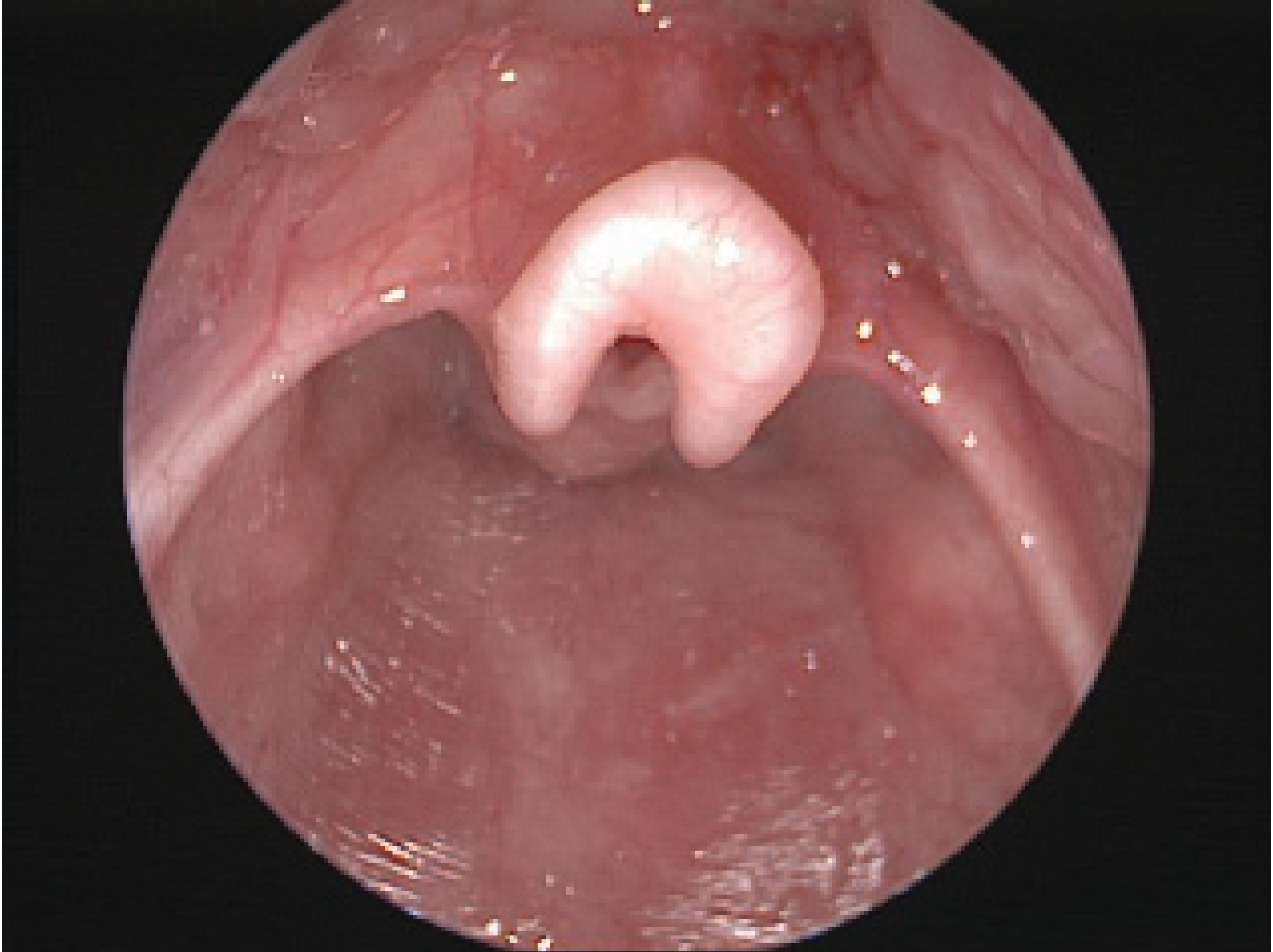
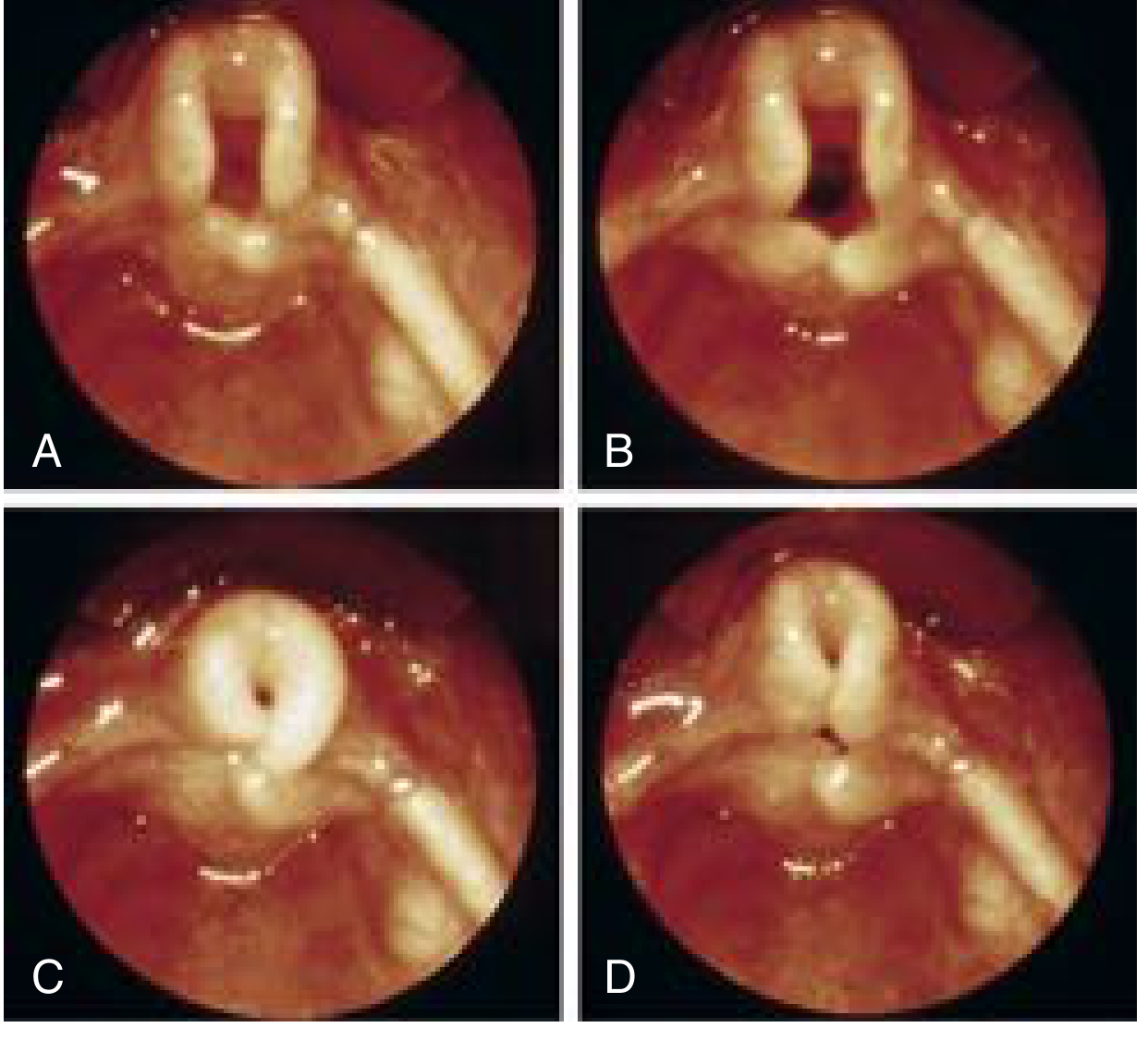
Key endoscopic findings:
- Omega-shaped (curled, long) epiglottis
- Short, foreshortened aryepiglottic folds tethering the epiglottis posteriorly
- Redundant arytenoid mucosa prolapsing into the glottic airway on inspiration
- Deep interarytenoid cleft
- Normal vocal fold mobility (important to confirm - differentiates from vocal cord paralysis)
LM Classification (K.J. Lee):
- Type 1: Foreshortened/tight aryepiglottic folds
- Type 2: Redundant supraglottic tissue
- Type 3: Posterior epiglottic collapse - associated with underlying neuromuscular disorders
ASSESSING SEVERITY - A Practical Summary
| Feature | Mild | Severe (Red Flags) |
|---|---|---|
| Stridor | Only with activity | At rest |
| SpO2 | Normal | Desaturations |
| Recession | Mild, intermittent | Marked sternal/intercostal at rest |
| Feeding | Minor difficulty | Prolonged, frequent breaks, fatigue |
| Weight gain | Normal | Failure to thrive |
| Episodes | No apnoea/cyanosis | Apnoeic/cyanotic spells |
| GORD | Absent or mild | Prominent, worsening LM |
- ~90% of cases are mild and resolve spontaneously by 18-24 months without intervention
- Severe cases require supraglottoplasty (endoscopic surgical division of the aryepiglottic folds)
INVESTIGATIONS TO CONSIDER
- SpO2 monitoring (pulse oximetry)
- Weight chart / growth monitoring (serial)
- Chest X-ray if indicated (hyperinflation, aspirate, cardiac silhouette)
- Flexible nasolaryngoscopy - definitive (usually done by ENT/Paediatric otolaryngologist)
- GORD workup if clinically indicated (pH impedance study)
- Rigid microlaryngobronchoscopy under GA - if severe stridor, cyanosis, or secondary airway lesion suspected (~10-15% of LM cases have a synchronous lesion)
Sources: Cummings Otolaryngology Head & Neck Surgery | Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2 | K.J. Lee's Essential Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.