Type 2 alveolar epithelial cell full details from fishman and Murray md exam answer 15 marks crisp and condensed structured
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
I now have all the material needed. Let me compile the comprehensive 15-mark answer.
Type II Alveolar Epithelial Cell (AT2 Cell / Type II Pneumocyte)
Sources: Fishman's Pulmonary Diseases and Disorders, 5e; Murray & Nadel's Textbook of Respiratory Medicine
1. Overview and Nomenclature
- Also called: type II pneumocyte, granular pneumocyte, great alveolar cell, septal cell
- Classically termed the "defender of the alveolus" (Mason & Williams, 1977)
- Despite being called the "large alveolar cell," its mean volume is actually less than half that of the type I cell (Table 2-2, Fishman's)
- Numerically the more abundant cell type, but covers only ~5% of the alveolar surface (type I cells cover ~95%)
2. Morphology and Ultrastructure
Light microscopy:
- Cuboidal shape; apical surface bulges into the alveolar lumen
- Located preferentially at alveolar corners and near pores of Kohn
- Usually found as solitary cells; clustering occurs only during repair after injury
Electron microscopy (see EM image below):
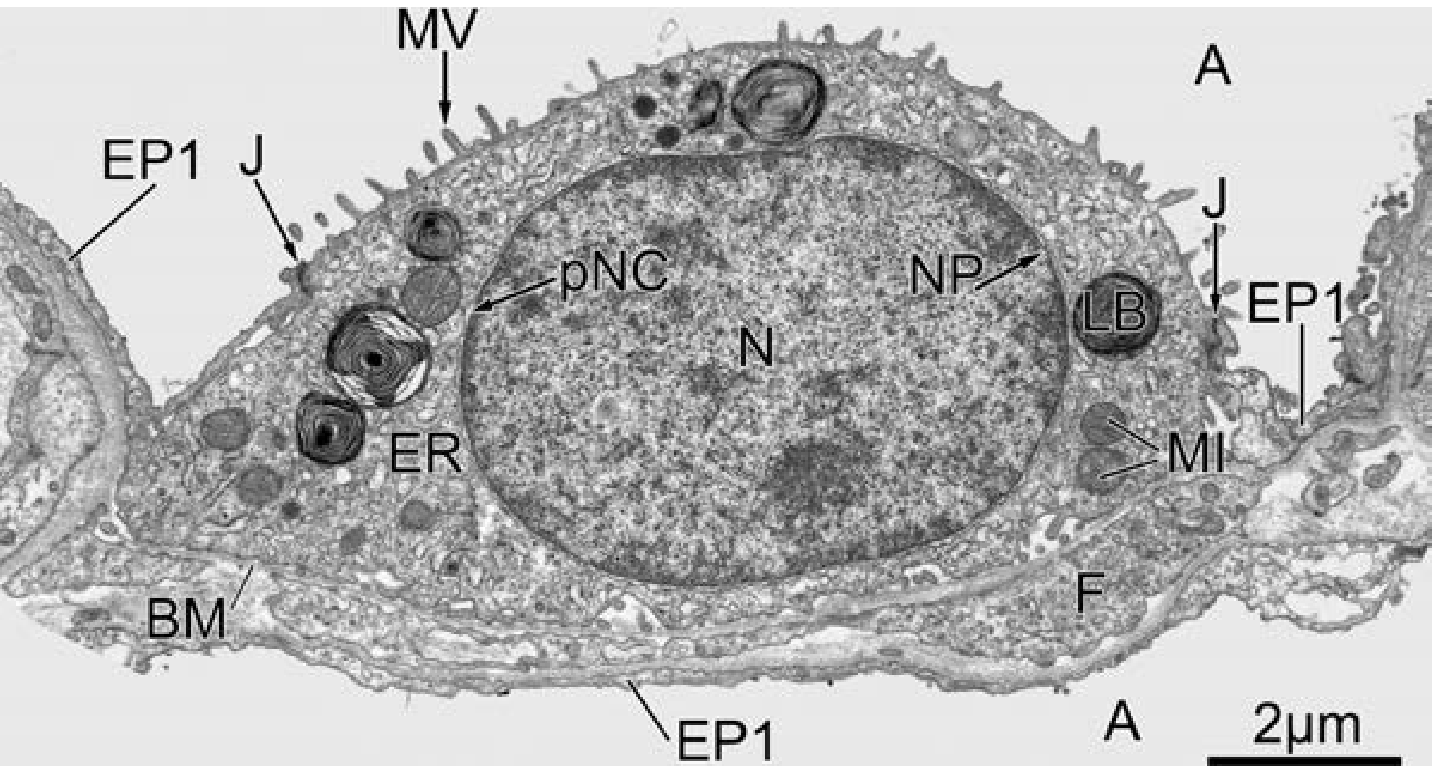
- Microvilli on apical surface (concentrated at periphery, smooth center)
- Abundant cytoplasmic organelles: mitochondria, rough ER with ribosomes, well-developed Golgi complex
- Multivesicular bodies (MVBs): junction point between biosynthetic and endocytic pathways
- Lamellar bodies: the hallmark organelle (see below)
- Basement membrane beneath AT2 cells is occasionally interrupted - foot processes can extend into interstitium toward interstitial cells
- Forms junctions (tight junctions + desmosomes) with adjacent type I cells
3. Lamellar Bodies - The Defining Organelle
| Feature | Detail |
|---|---|
| Nature | Secretory lysosome-related organelles |
| Contents | Densely packed phospholipid lamellae |
| Size | ~1 μm diameter - among the largest secretory organelles in the body |
| Number per cell | 200-500 lamellar bodies/cell |
| Total volume (both lungs) | ~2 cm³ |
| pH | ~5.5 (acidic) |
| Enzymes | Acid phosphatase, cathepsins |
| Membrane proteins | LAMP (lysosomal membrane proteins) |
| Species difference | Rodents: parallel stacks; Humans: concentric lamellae with projection core of short stacks |
| Turnover time of surfactant | 4-10 hours |
Synthesis pathway: ER → Golgi → MVBs → Lamellar bodies → Exocytosis
4. Surfactant - Synthesis, Secretion, and Recycling
Composition
- ~90% lipids: mainly saturated phosphatidylcholine (DPPC)
- ~10% proteins: SP-A, SP-B, SP-C, SP-D
- Motto: "Keeps alveoli open, dry, and clean"
Surfactant Proteins and Their Roles
| Protein | Type | Secretion Route | Function |
|---|---|---|---|
| SP-A | Hydrophilic | Constitutive (bypasses lamellar bodies) | Tubular myelin formation; innate immunity; inhibits surfactant secretion; stimulates reuptake |
| SP-B | Hydrophobic | Lamellar body (projection core) | Transforms LB → tubular myelin; surface activity |
| SP-C | Hydrophobic | Lamellar body | Surface activity |
| SP-D | Hydrophilic | Constitutive | Innate immunity; immune modulation |
Intra-alveolar Surfactant Subtypes (in sequence)
- Freshly secreted lamellar body-like forms (hypophase)
- Tubular myelin - unique lattice structure, probable precursor of surface film (SP-A + SP-B required)
- Surface film - reduces alveolar surface tension
- Small unilamellar vesicles - "spent" surfactant for recycling
Secretion Mechanism
- Lamellar body membrane fuses with apical plasma membrane
- Fusion pore forms, diameter < lamellar body diameter
- Surfactant is squeezed through the pore
- Primary physiologic trigger: mechanical stretch during ventilation (direct on AT2 cells, or indirectly via AT1 cells/capillary endothelium as "strain sensors")
Clearance and Recycling
- Major route: Reuptake by type II cells → recycled or degraded
- Minor routes: Alveolar macrophage ingestion + lysosomal degradation; clearance via airways
- SP-A inhibits secretion and stimulates reuptake (negative feedback)
5. Functions of the Type II Cell - "Defender of the Alveolus"
A. Surfactant Production
- Prevents alveolar atelectasis - surface area-dependent reduction of alveolar surface tension
- Prevents intra-alveolar edema - reduces transcapillary fluid forces
- Innate host defense - immunomodulatory functions (especially SP-A and SP-D)
B. Alveolar Epithelial Regeneration (Stem Cell Role)
- AT2 cells are progenitor/stem cells of the alveolar epithelium
- Can transdifferentiate into type I alveolar cells (AT1) after injury
- Normally found singly; proliferates to form clusters during epithelial repair
- AT2 progenitor cells reside in niches adjacent to fibroblasts
- Wnt signaling (juxtacrine, from fibroblasts) maintains the AT2 stem cell pool
- Autocrine Wnt activation in AT2 cells prevents transdifferentiation to AT1
- Blockade of Wnt in AT2 → permits AT1 transdifferentiation (in vitro)
- Demonstrated using "alveolospheres" - organoid assays in Matrigel with fibroblasts
6. Pathological Significance
Surfactant Dysfunction Disorders
| Condition | Mechanism |
|---|---|
| RDS of prematurity | Developmental deficiency - lung immaturity |
| Hereditary surfactant dysfunction | Mutations in SP-B, SP-C, or ABCA3 (limiting membrane of LBs) |
| ARDS/Acute lung injury | Damage to AT2 cells; oxidant/neutrophil elastase damage to surfactant proteins; plasma protein inhibition |
| IPF | Loss of AT2 cells, reduced regenerative capacity; ER stress from SP-A2/SP-C mutations |
ER Stress and UPR in Fibrosis
- SP-A2 and SP-C mutations → misfolded surfactant proteins → ER stress → Unfolded Protein Response (UPR)
- AT2 dysfunction: acquires profibrotic phenotype → promotes fibroblast expansion, myofibroblast activation, ECM deposition
- AT2 cells do not directly transform into mesenchymal cells (no EMT)
- In IPF: loss of AT2 cells + expansion of basal cells documented by single-cell RNA sequencing
AT2 in IPF (Fishman's, block 11)
- AT2 cells have reduced regenerative capacity in IPF organoid assays
- Restoration of AT2 regenerative capacity = active therapeutic target
- Expanded basal cells in IPF produce secretory-primed phenotype in mucin-rich areas
7. Key Distinguishing Features vs. Type I Cell
| Feature | Type I Cell | Type II Cell |
|---|---|---|
| Shape | Squamous/flat | Cuboidal |
| Surface coverage | ~95% alveolar surface | ~5% alveolar surface |
| Volume | Larger | Smaller (<½ of type I) |
| Organelles | Sparse | Abundant (ER, Golgi, LBs) |
| Lamellar bodies | Absent | Present (pathognomonic) |
| Microvilli | Absent | Present (peripheral tuft) |
| Function | Gas exchange | Surfactant production + repair |
| Stem cell capacity | None | Yes - generates AT1 cells |
8. Surfactant Replacement Therapy (Clinical Correlate)
- Primary indication: RDS of premature neonates
- One of the major advances in neonatology
- Expanding indications: other forms of respiratory failure (ARDS) where endogenous surfactant is impaired/inactivated
- Efficacy depends on preparation's ability to resist the same inhibition that inactivated the endogenous system
- The story of surfactant therapy is a paradigmatic example of translational bench-to-bedside medicine
Sources: Fishman's Pulmonary Diseases and Disorders, 5e (Chapter 2 - Alveolar Architecture; Chapter on IPF) | Murray & Nadel's Textbook of Respiratory Medicine, 7e
This is a shared conversation. Sign in to Orris to start your own chat.