Trachoma
Reading File
Finding Sources
Searching PubMed
trachoma Chlamydia trachomatis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of trachoma drawn from Harrison's 22e, Kanski's Clinical Ophthalmology 10e, and Park's Textbook of Preventive & Social Medicine.
Trachoma
Definition & Causative Agent
Trachoma is a chronic infectious keratoconjunctivitis caused by Chlamydia trachomatis serovars A, B, Ba, and C. It is the world's leading cause of preventable infectious blindness. The disease is closely linked to poverty, overcrowding, and poor hygiene, and its severity is driven largely by cycles of re-infection within communities. - Harrison's Principles of Internal Medicine 22E, p. 1518; Kanski's Clinical Ophthalmology 10e, p. 191
Epidemiology
- The WHO estimates ~6 million people have been blinded by trachoma; ~1.3 million currently have preventable blindness from it.
- Hyperendemic zones: northern and sub-Saharan Africa, Middle East, drier parts of the Indian subcontinent, and Southeast Asia.
- In hyperendemic areas, prevalence is nearly 100% by age 2-3 years. Children are the primary reservoir for active infection; adults suffer the blinding sequelae.
- Transmission occurs via contact with ocular/nasal discharge, direct person-to-person spread, and through eye-seeking flies (Musca sorbens) acting as mechanical vectors.
- The WHO Neglected Tropical Diseases roadmap 2021-2030 targets global elimination of blinding trachoma as a public health problem by 2030. - Harrison's 22E, p. 1518
Pathogenesis
A single episode of trachomatous conjunctivitis may be relatively mild, but repeated re-infections trigger a chronic cell-mediated (Type IV delayed hypersensitivity) immune response to chlamydial antigens. Prior contact confers only short-term partial immunity and actually heightens the inflammatory response on re-infection. This is why vaccination attempts have historically sensitized rather than protected individuals. - Kanski's Clinical Ophthalmology 10e, p. 191
Clinical Manifestations
Disease unfolds in two overlapping phases:
Active (Inflammatory) Phase
Most common in pre-school children.
- Mixed follicular/papillary conjunctivitis with mucopurulent discharge (in children <2 years the papillary component may dominate)
- Superior epithelial keratitis and pannus formation (superficial corneal vascularization from the superior limbus downward)
- Inflammatory leukocytic infiltration of the cornea
Cicatricial (Scarring) Phase
Prevalent in middle age and adults.
- Linear or stellate conjunctival scars (mild) or broad confluent scars - the classic "Arlt line" (severe)
- Herbert pits: shallow depressions at the superior limbus left by resolved limbal follicles - pathognomonic of trachoma
- Trichiasis: inward turning of eyelashes abrading the cornea
- Entropion (cicatricial): inward rotation of the eyelid margin
- Progressive corneal ulceration, scarring, and opacification leading to blindness
- Dry eye: goblet cell and lacrimal gland duct destruction causes xerosis and secondary bacterial corneal ulcers
- Seasonal co-epidemics with H. influenzae conjunctivitis worsen inflammatory damage in endemic communities
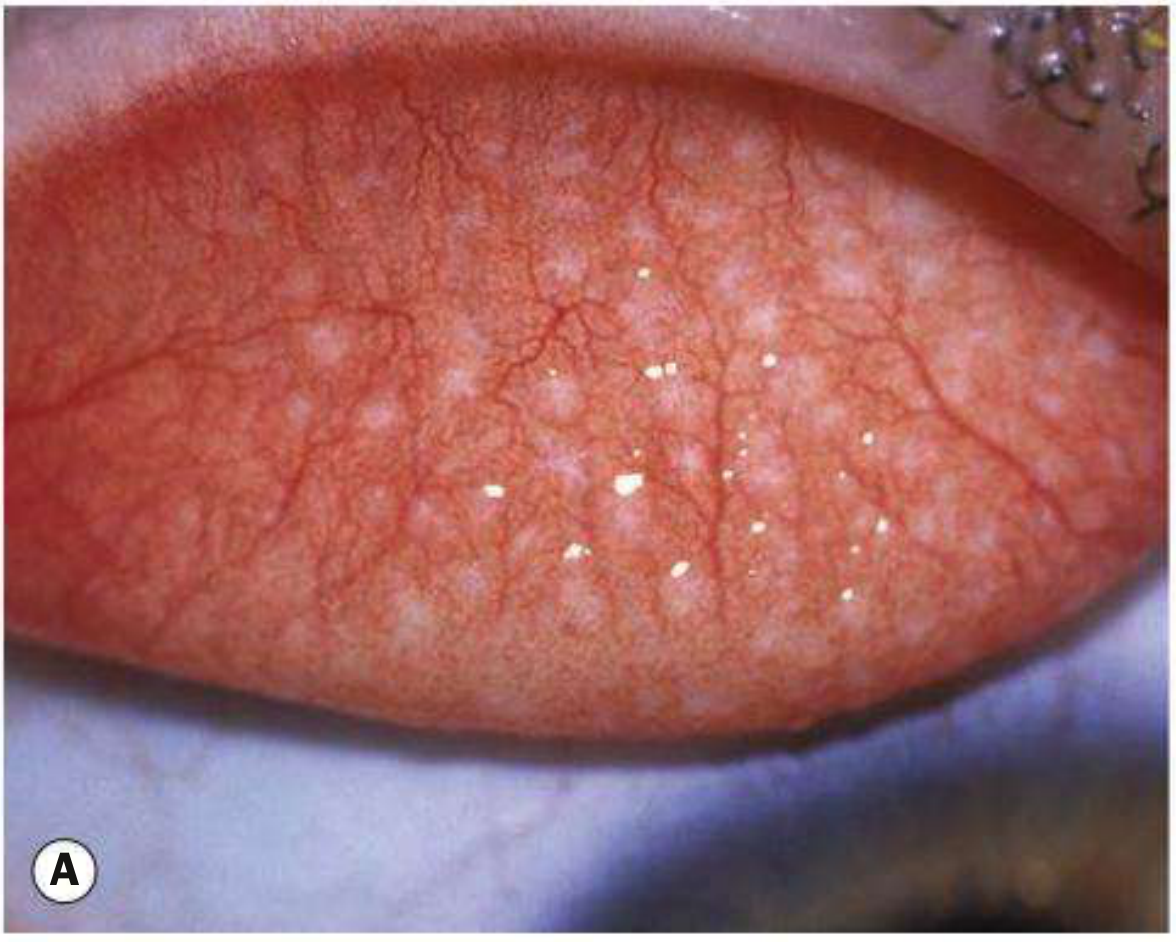
Clinical Photographs
A - Typical white subtarsal follicles (active trachoma):
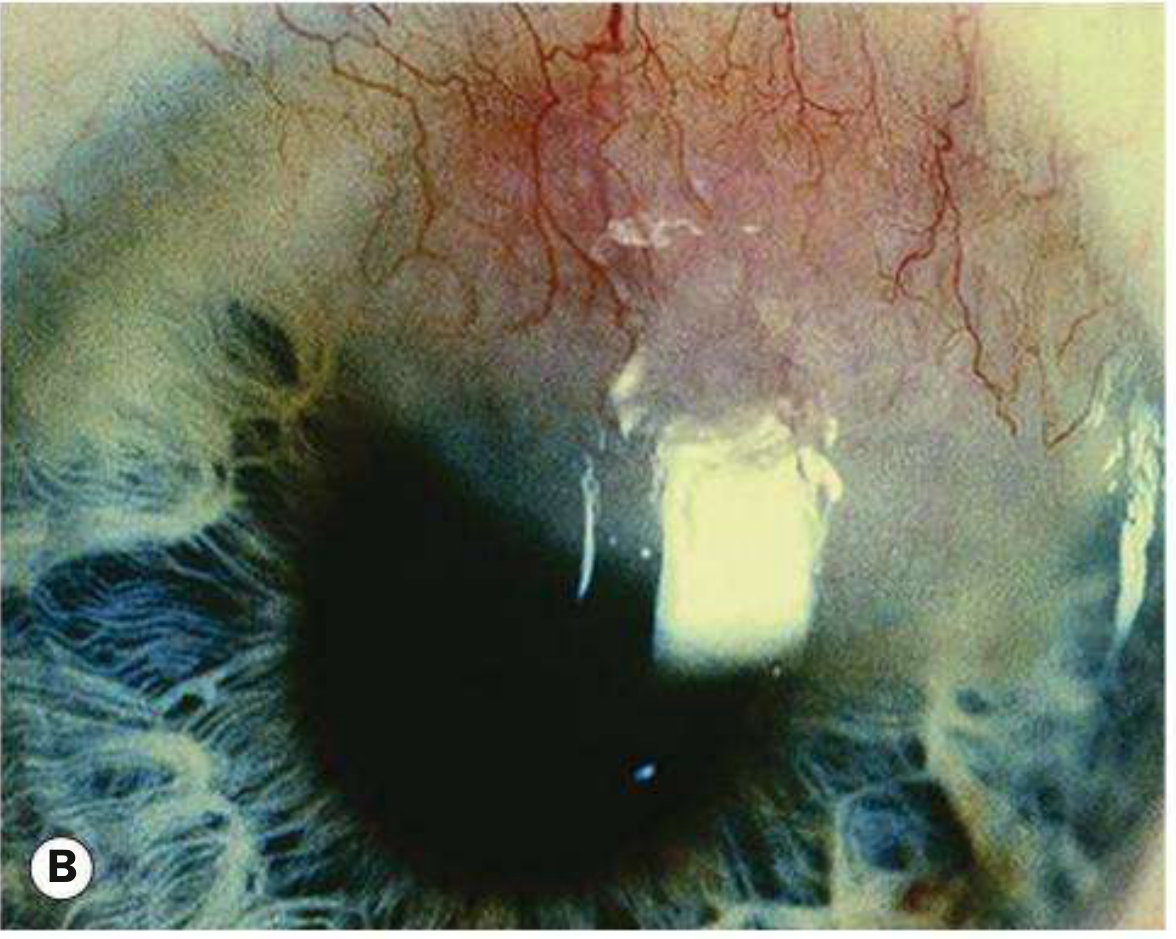
B - Marked corneal pannus (vascular ingrowth from superior limbus):
C - Stellate conjunctival scarring (arrow):
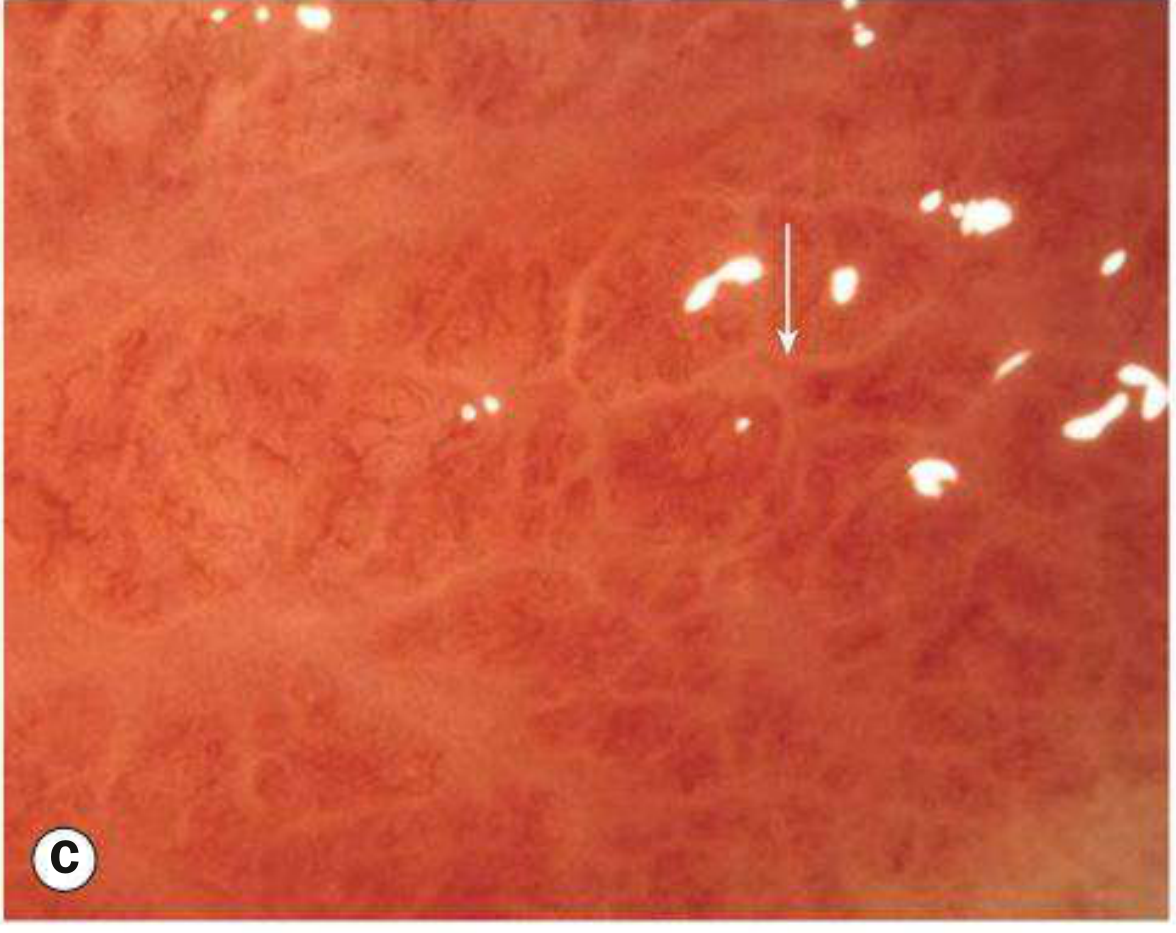
Images from Kanski's Clinical Ophthalmology 10e, Fig. 6.7
WHO Grading System (SAFE-related classification)
| Grade | Definition |
|---|---|
| TF - Trachomatous Inflammation (Follicular) | ≥5 follicles (>0.5 mm) on the superior tarsal plate |
| TI - Trachomatous Inflammation (Intense) | Diffuse tarsal involvement obscuring ≥50% of deep tarsal vessels; papillae present |
| TS - Trachomatous Scarring | Easily visible fibrous white tarsal bands |
| TT - Trachomatous Trichiasis | At least one lash touching the globe |
| CO - Corneal Opacity | Opacity sufficient to blur part of the pupillary margin |
- Kanski's Clinical Ophthalmology 10e, p. 192
Diagnosis
Clinical diagnosis requires at least 2 of the following 4 signs:
- Lymphoid follicles on the upper tarsal conjunctiva
- Typical conjunctival scarring
- Vascular pannus (most marked at the superior limbus)
- Limbal follicles or their sequelae (Herbert pits)
Laboratory confirmation:
-
Giemsa staining of conjunctival smears: intracytoplasmic chlamydial inclusions in 10-60% of active cases
-
NAATs (PCR) are most sensitive and specific - can detect chlamydial DNA even when cultures are negative, suggesting persistent infection is more common than previously recognized
-
NAATs remain prohibitively expensive for most endemic regions
-
Harrison's 22E, p. 1518; Park's Textbook of Preventive and Social Medicine
Treatment
Individual Treatment
| Drug | Regimen | Notes |
|---|---|---|
| Azithromycin (1st line) | Single oral dose: 20 mg/kg (up to 1 g) | Drug of choice; no documented chlamydial resistance |
| Doxycycline | 100 mg twice daily x 10-14 days | Avoid in pregnancy and children <12 (tooth staining) |
| Erythromycin | 500 mg twice daily x 14 days | Alternative for pregnancy/children |
| Topical tetracycline 1% ointment | Twice daily x 6 weeks | Less effective than oral treatment; used as alternative |
- All sexual partners and family members should be treated simultaneously to prevent re-infection.
- A single course is not always sufficient; communities may need annual treatment cycles.
Surgical Treatment
- Bilamellar tarsal rotation for cicatricial entropion and trichiasis - aims to relieve lid inversion and maintain full lid closure, preventing ongoing corneal abrasion.
The WHO SAFE Strategy (Control Framework)
The international standard for trachoma control endorsed by WHO:
| Letter | Component | Details |
|---|---|---|
| S | Surgery | For trichiasis/entropion - immediate impact on blindness prevention |
| A | Antibiotics | Azithromycin (mass or selective treatment) |
| F | Facial hygiene | Facial cleanliness is a critical preventive measure |
| E | Environmental improvement | Access to clean water, sanitation, fly control |
Mass vs. Selective Treatment
-
Mass (blanket) treatment: indicated when moderate-to-severe trachoma prevalence is >5% in children under 10 - tetracycline 1% ointment twice daily for 5 consecutive days/month for 6 months, or 60 consecutive days. Azithromycin mass drug administration is now preferred.
-
Selective treatment: used in low-to-medium prevalence communities - screen first, treat only those with active disease.
-
Park's Textbook of Preventive and Social Medicine, p. 1135-1168; Kanski's Clinical Ophthalmology 10e, p. 192
Key Points Summary
| Feature | Detail |
|---|---|
| Causative organism | C. trachomatis serovars A, B, Ba, C |
| Mechanism of blindness | Trichiasis → corneal abrasion → ulceration → scarring/opacification |
| Pathognomonic sign | Herbert pits (healed limbal follicles) |
| Classic scar | Arlt line (broad horizontal scar on tarsal conjunctiva) |
| Diagnosis | ≥2 of 4 WHO criteria; NAATs most sensitive |
| Treatment of choice | Azithromycin single dose (20 mg/kg, max 1 g) |
| Surgery | Bilamellar tarsal rotation for entropion/trichiasis |
| Control strategy | SAFE (Surgery, Antibiotics, Facial hygiene, Environmental improvement) |
| Elimination target | 2030 (WHO NTD Roadmap) |
Recent evidence note: A 2025 systematic review and meta-analysis (PMID: 40860538) examined the prevalence and risk factors for active trachoma among children aged 1-9 in low-income African countries, reconfirming that young children in resource-poor settings remain the highest-burden group and that socioeconomic and hygiene factors remain key drivers - consistent with textbook guidance.
Corneal ulcer
Finding Sources
Searching PubMed
corneal ulcer keratitis management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of corneal ulcer drawn from Kanski's Clinical Ophthalmology 10e, Wills Eye Manual, and Tintinalli's Emergency Medicine.
Corneal Ulcer
Definition
A corneal ulcer is a serious infection involving multiple layers of the cornea - specifically when infectious agents invade the underlying corneal stroma through a break in the epithelial barrier. Unlike a simple epithelial defect, a true ulcer involves tissue loss extending into the stroma, resulting in a white/gray infiltrate with an overlying epithelial defect. - Tintinalli's Emergency Medicine, p. 191
Pathophysiology
The sequence of events:
- Epithelial barrier disruption (by trauma, desiccation, hypoxia, direct microbial invasion, or desquamation)
- Microorganisms gain access to the corneal stroma
- Inflammatory cell recruitment causes stromal necrosis and tissue loss
- Progressive thinning may lead to descemetocoele (posterior bulging of Descemet membrane) and perforation
Some organisms (N. gonorrhoeae, N. meningitidis, C. diphtheriae, H. influenzae) can penetrate an intact corneal epithelium. All others require a pre-existing defect.
Etiology & Risk Factors
Common Organisms
| Category | Pathogens |
|---|---|
| Bacteria | Pseudomonas aeruginosa (>60% of CL-related), S. pneumoniae, S. aureus, Streptococci, Moraxella spp. |
| Fungi | Fusarium, Aspergillus (filamentous); Candida (yeast) |
| Viruses | HSV, VZV |
| Protozoa | Acanthamoeba spp. |
Key Risk Factors
| Risk Factor | Associated Pathogen |
|---|---|
| Contact lens wear (especially extended-wear soft lenses) | Pseudomonas (most common), Acanthamoeba |
| Trauma with vegetable matter / agricultural injury | Filamentous fungi (Fusarium, Aspergillus) |
| Chronic ocular surface disease / dry eye | Candida, HSV |
| Topical or systemic steroids | Fungal, viral |
| Immunosuppression / diabetes | Fungal |
| Post-refractive surgery (LASIK) | Bacterial |
| Bell's palsy / exposure keratopathy | S. pneumoniae, S. aureus |
| Swimming/hot tub use with contact lenses | Acanthamoeba |
Symptoms
- Pain (often severe; disproportionately severe pain suggests Acanthamoeba or Pseudomonas)
- Photophobia
- Foreign body sensation
- Redness and lid swelling
- Mucopurulent or purulent discharge
- Decreased visual acuity (especially if ulcer is in the visual axis)
- Acute contact lens intolerance
Signs
On slit-lamp examination:
-
Focal white/gray stromal opacity (infiltrate) with overlying epithelial defect - the hallmark finding. An examiner using a slit beam cannot see clearly through an infiltrate/ulcer to the iris (unlike stromal edema or mild scars which are more transparent)
-
Stromal edema, folds in Descemet membrane
-
Anterior uveitis: cells and flare, keratic precipitates
-
Hypopyon (sterile layered pus in anterior chamber) - common in moderate-to-severe disease
-
Circumcorneal injection (ciliary flush)
-
Chemosis and eyelid swelling (moderate-severe)
-
Descemetocoele (bulging of Descemet membrane) in severe thinning
-
Posterior synechiae, raised IOP in severe cases
-
Wills Eye Manual, p. 199; Kanski's Clinical Ophthalmology 10e, p. 227
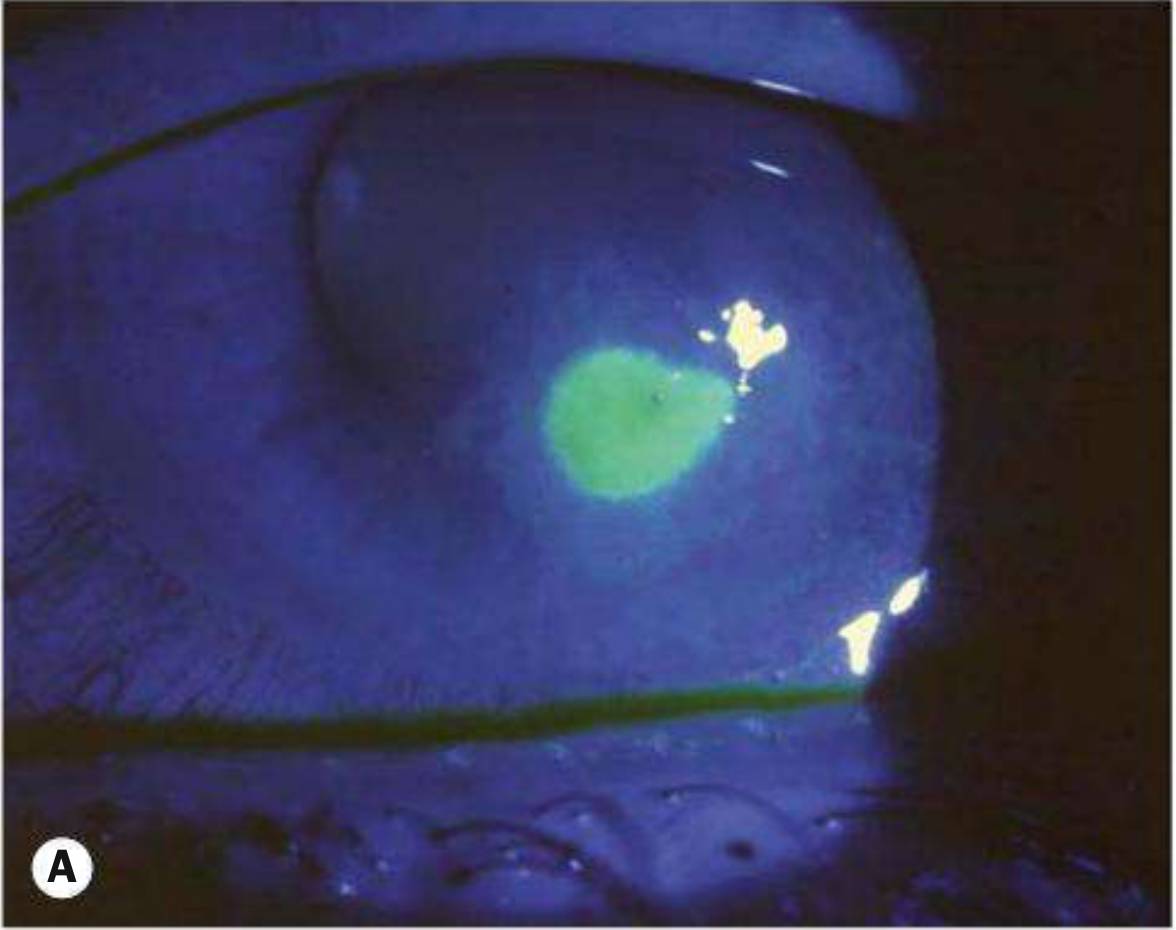
Clinical Photographs
A - Bacterial keratitis: fluorescein-stained corneal ulcer (epithelial defect glows green under cobalt blue light):
D - Large Pseudomonas corneal ulcer with dense white infiltrate covering most of the cornea:

Fig. 7.7 Bacterial keratitis, Kanski's Clinical Ophthalmology 10e
Types of Corneal Ulcer
1. Bacterial Keratitis
- Presentation: rapid onset, pain, mucopurulent discharge
- Hallmark: focal well-defined white/yellow-white infiltrate with epithelial defect
- Pseudomonas: particularly aggressive, may cause rapid perforation
- S. aureus: focal, fairly well-defined infiltrate
- Streptococci: often aggressive
2. Fungal Keratitis
A - Filamentous keratitis (Fusarium/Aspergillus) with fluffy edges and satellite lesions (arrow); B - ring infiltrate and satellite lesions; C - large ulcer with hypopyon; D - Candida stained with calcofluor white:
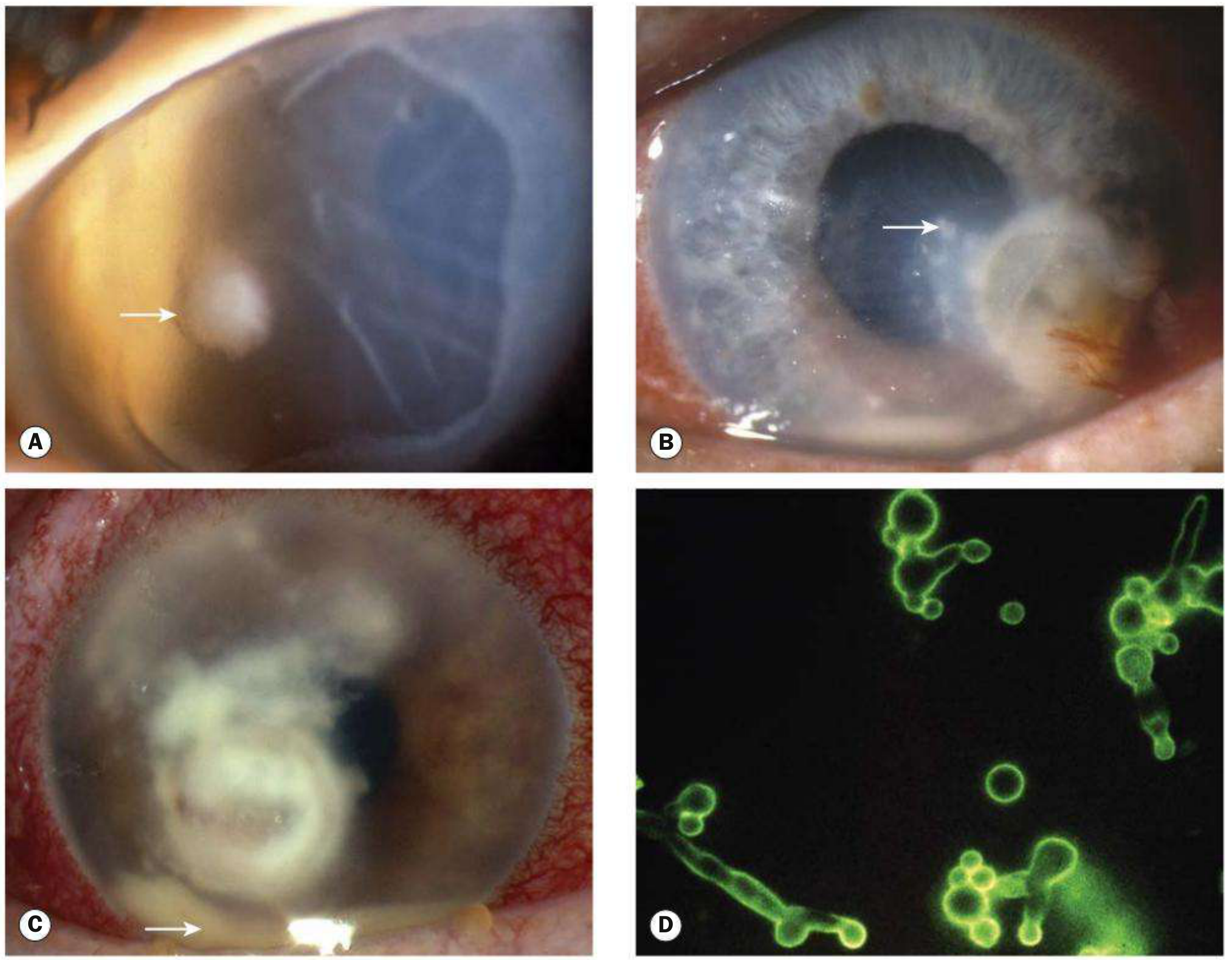
Fig. 7.10 Fungal keratitis, Kanski's Clinical Ophthalmology 10e
- Filamentous fungi (tropics, agricultural trauma): gray-white stromal infiltrate with indistinct fluffy margins, satellite lesions, feathery branch-like extensions, ring infiltrate
- Candida (temperate climates, pre-existing ocular disease): yellow-white densely suppurative infiltrate, mimics bacterial ulcer
- Key feature: infiltrate often extends beyond the epithelial defect
- Can penetrate intact Descemet membrane and cause endophthalmitis without obvious perforation
- Diagnosis frequently delayed - always maintain high suspicion
3. Acanthamoeba Keratitis
Radial keratoneuritis (perineural infiltration) - pathognomonic early sign:
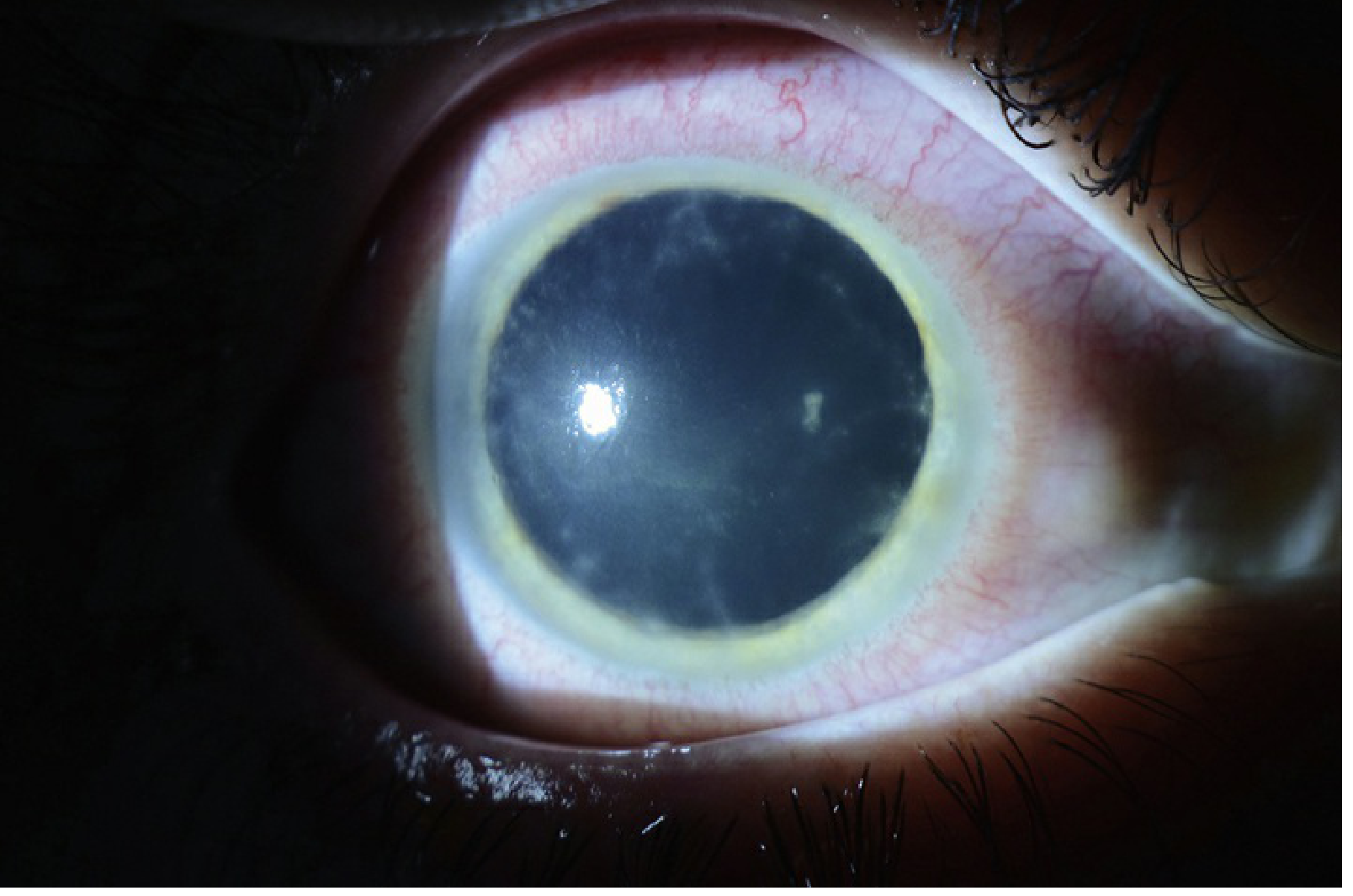
Fig. 4.13.1, Wills Eye Manual
- Classic history: soft contact lens wearer + exposure to water (swimming, hot tub, tap water for lens cleaning)
- Pain out of proportion to early clinical findings
- Early: pseudodendrites, epitheliitis, subepithelial microcysts, radial keratoneuritis (perineural infiltrates) - pathognomonic
- Late (3-8 weeks): ring-shaped stromal infiltrate
- Bacteria cultures are negative; does not respond to antibiotics or antivirals
- Often mimics HSV keratitis early - always consider Acanthamoeba in contact lens wearers with apparent HSV
Investigations
Corneal Scraping (when to do it)
Scrape all ulcers that are:
-
2 mm in size
- Middle to deep stromal involvement
- Within the visual axis
- Chronic or atypical in appearance
Technique:
- Instill preservative-free topical anaesthetic (e.g., proxymetacaine 0.5%)
- Use No. 11 scalpel blade, 20-21G hypodermic needle tip, or Kimura spatula
- Remove loose mucus/necrotic tissue first
- Scrape margins and base of lesion
Culture Media (routine)
- Blood agar - general bacteria
- Chocolate agar - Neisseria, Haemophilus
- Sabouraud dextrose agar - fungi
- Brain-heart infusion (BHI) - enrichment broth
Stains
| Stain | Best For |
|---|---|
| Gram stain | Bacteria (sensitivity ~60-80%) |
| Giemsa | General, Acanthamoeba cysts |
| KOH preparation | Fungi (rapid, highly sensitive) |
| Calcofluor white | Fungi, Acanthamoeba |
| PAS, GMS (methenamine silver) | Fungi |
| PCR | Acanthamoeba (very sensitive, ~up to 90% for fungi) |
Other
-
Confocal microscopy: in vivo identification of organisms; especially useful for Acanthamoeba; not widely available outside tertiary centres
-
Corneal biopsy: for suspected fungal keratitis with no improvement after 3-4 days and no growth on culture after 1 week
-
Kanski's Clinical Ophthalmology 10e, p. 228
Management
General Measures (All Ulcers)
- Discontinue contact lens wear immediately
- Cycloplegic drop (e.g., cyclopentolate 1% TID; atropine 1% BID-TID if hypopyon present) - for comfort and to prevent posterior synechiae
- Obtain cultures before starting antibiotics
- Emergent ophthalmology referral
- Avoid topical steroids until infection is controlled
Bacterial Keratitis - Treatment Algorithm (Wills Eye)
| Risk Level | Criteria | Treatment |
|---|---|---|
| Low risk | Small peripheral infiltrate, minimal AC reaction, no discharge | Fluoroquinolone (moxifloxacin/gatifloxacin/levofloxacin) q1-2h awake |
| Borderline | 1-1.5 mm infiltrate, or smaller with epithelial defect/mild AC reaction | Fluoroquinolone q1h around the clock ± polymyxin B/trimethoprim |
| Vision-threatening | >1.5-2 mm, in visual axis, or unresponsive to initial treatment | Fortified antibiotics: tobramycin/gentamicin (15 mg/mL) alternating with cefazolin (50 mg/mL) or vancomycin (25 mg/mL) - one drop every 30 minutes around the clock |
Note: Moxifloxacin and besifloxacin have slightly better Gram-positive coverage. Gatifloxacin and ciprofloxacin have slightly better Pseudomonas and Serratia coverage.
Fungal Keratitis - Treatment
| Fungus Type | 1st Line | Alternatives |
|---|---|---|
| Candida | Amphotericin B 0.15% or econazole 1% topically | Natamycin 5%, voriconazole |
| Filamentous | Natamycin 5% (only FDA-approved topical antifungal) or econazole 1% | Amphotericin B 0.15%, miconazole 1%, voriconazole 1-2% |
- Start hourly for 48 hours, then reduce as signs permit
- Systemic antifungals for severe cases: voriconazole 400 mg BID x1 day then 200 mg BID; itraconazole 200 mg OD; fluconazole 200 mg BID
- Tetracycline (doxycycline 100 mg BID) for anticollagenase effect if significant thinning
- Therapeutic keratoplasty (penetrating or deep anterior lamellar) when medical therapy fails or post-perforation
Acanthamoeba Keratitis - Treatment
- PHMB (polyhexamethylene biguanide) 0.02% + propamidine isethionate (Brolene) 0.1% topically - intensive initially then tapered over months
- Treatment is prolonged (often >6 months)
- Does not respond to standard antibiotics or antivirals
Surgical Options for Corneal Ulcer Complications
| Situation | Intervention |
|---|---|
| Persistent epithelial defect | Bandage contact lens, tarsorrhaphy, amniotic membrane graft |
| Severe thinning | Tissue glue + bandage contact lens |
| Descemetocoele/perforation | Penetrating keratoplasty (therapeutic), tissue glue |
| End-stage scarring | Optical penetrating keratoplasty (once infection resolved) |
Recent evidence note: A 2025 systematic review (PMID: 39257085) found that amniotic membrane grafts are effective for managing persistent epithelial defects following infective corneal ulcers and keratitis, consistent with Kanski's guidance on this technique.
Differential Diagnosis Summary
| Feature | Bacterial | Fungal (Filamentous) | Fungal (Candida) | Acanthamoeba |
|---|---|---|---|---|
| Onset | Acute/rapid | Subacute/insidious | Subacute | Weeks to months |
| Infiltrate borders | Well-defined | Fluffy, feathery | Dense, suppurative | Variable |
| Special features | Hypopyon common | Satellite lesions, ring | Mimics bacterial | Radial keratoneuritis, ring infiltrate late |
| Key history | Contact lens, trauma | Vegetable matter, tropics | Pre-existing ocular disease | Contact lens + water exposure |
| Pain | Moderate-severe | Moderate | Moderate | Severe, out of proportion |
| Culture media | Blood, chocolate | Sabouraud | Sabouraud | Non-nutrient agar with E. coli |
| Key stain | Gram | KOH, calcofluor | KOH, calcofluor | Calcofluor, Giemsa, confocal |
| Treatment | Fluoroquinolone / fortified ABx | Natamycin / voriconazole | Amphotericin B / econazole | PHMB + propamidine |
- Kanski's Clinical Ophthalmology 10e, p. 226-233; Wills Eye Manual, p. 199-215; Tintinalli's Emergency Medicine, p. 191
This is a shared conversation. Sign in to Orris to start your own chat.