Discuss the role of external and middle ear in the physiology of hearing. MS ent University exam pattern for 20 marks.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have all the material needed for a comprehensive MS ENT university exam answer. Let me compose the full response.
Role of the External and Middle Ear in the Physiology of Hearing
(MS ENT University Examination - 20 Marks)
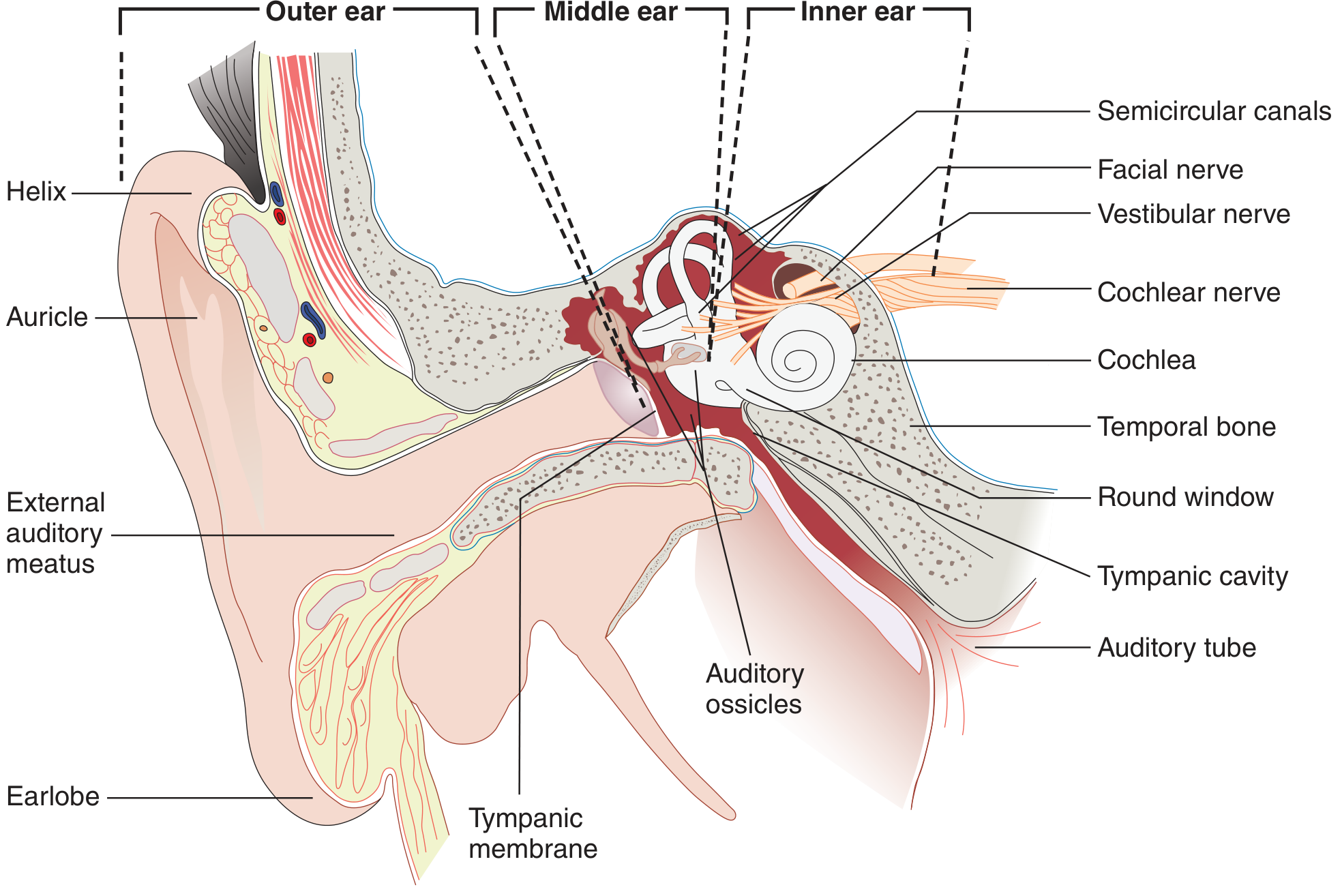
Fig. 1 - Structures of the outer, middle, and inner ear (Ganong's Review of Medical Physiology, 26th Ed.)
Introduction
The process of hearing - audition - requires the detection and neural encoding of airborne sound vibrations. Because sound travels as pressure waves in air while the sensory apparatus of the cochlea is immersed in fluid, a considerable mechanical challenge exists: approximately 99.9% of sound energy incident on an air-fluid interface is reflected back (a loss of ~30 dB). The external and middle ears together constitute the conductive pathway of hearing whose primary role is to capture, concentrate, and efficiently transmit acoustic energy to the cochlea while minimizing this impedance mismatch. Each component contributes in a physiologically precise manner.
I. THE EXTERNAL EAR
Components
- Pinna (auricle)
- External auditory canal (EAC)
- Tympanic membrane (lateral surface)
1. The Pinna
Sound Capture and Funneling
The pinna is vestigial in humans; the auricular muscles are non-functional (unlike predatory mammals that actively rotate the pinna toward sound). However, the pinna still contributes to:
- Focusing acoustic energy onto the external auditory meatus, concentrating it toward the relatively smaller tympanic membrane surface area.
- Sound localization - the unique geometry of the pinna relative to the craniofacial skeleton creates wavelength-dependent delay paths. Combined with head shadow effects, this generates interaural time differences (ITD) and interaural intensity differences (IID) that allow the auditory cortex to compute the spatial position of a sound source, particularly in the vertical plane (elevation cues).
Head Shadow Effect: The head acts as an acoustic barrier between the two ears. A sound arriving from one side reaches the ipsilateral ear slightly earlier and with greater intensity. This binaural disparity is a key cue for horizontal sound localization.
Frequency-Specific Resonance: When the pinna acts in concert with the EAC, the combined unit produces frequency-specific resonance that partially compensates for the impedance loss expected at the air-fluid interface of the cochlea.
Clinical significance: A dysmorphic pinna may reflect underlying EAC and middle ear malformation (embryological co-development). Pinna defects are 3.5 per ear in Down syndrome vs 2.5 in normal individuals, associated with conductive hearing loss.
2. The External Auditory Canal (EAC)
Structure: The EAC is approximately 25-26 mm long in adults. It begins at the concha as the external auditory meatus (EAM) and ends at the tympanic membrane. It has:
- Outer third: cartilaginous, lined with skin containing sebaceous and apocrine ceruminous glands
- Inner two-thirds: bony, lined with thin epithelium
Acoustic (Resonance) Function - The EAC Transfer Function
The most important physiological role of the EAM and EAC is to transfer and amplify the acoustic signal from the open sound field to the tympanic membrane. The EAC acts as a quarter-wave resonator - an open-ended tube that resonates at approximately 2.7 kHz (where wavelength = 4 × length of canal).
This resonance produces a gain of approximately 9 dB centred around 2.7 kHz, boosting frequencies in the speech range (1-4 kHz) where hearing is most critical. At 2 kHz, when the entire external and middle ear system is most efficient, the combined external canal gain of 9 dB and middle ear gain of 26.6 dB offset the ~39.5 dB sound pressure loss at the air-cochlear fluid interface, yielding a total transfer gain of ~35.6 dB.
The EAC has maximum efficiency (low reflectance of the tympanic membrane) between 1 kHz and 4 kHz - exactly the speech frequency range.
Non-Acoustic Functions of the EAC:
- Wax (cerumen): Produced by sebaceous glands and modified apocrine glands; lubricates and cleans the canal; provides bactericidal protection via lysozyme, IgA, and fatty acids; maintains an acidic pH (~6.5-6.8) hostile to microorganisms.
- Skin migration: Dead skin migrates laterally (from umbo outward) - unique self-cleaning mechanism.
- Sensory innervation: Arnold's nerve (auricular branch of vagus) supplies the posterior canal - irritation triggers cough reflex or vasovagal response.
Clinical significance: Complete EAC occlusion (impacted wax, osteoma, atresia) causes conductive hearing loss of up to 40 dB with a high-frequency shift starting from 2 kHz.
3. The Tympanic Membrane (TM)
The TM separates the EAC from the middle ear. It has three layers:
- Outer squamous epithelium (continuous with EAC skin)
- Middle fibrous layer (radial and circular fibers - pars tensa; absent in pars flaccida)
- Inner mucosal layer (continuous with middle ear mucosa)
Mechanical Functions:
The TM is not a flat, uniformly vibrating membrane. Its non-uniform structure provides a multiple integrated multilever mechanical advantage:
- The lateral (canal) surface exhibits a uniphasic response with little pressure variation.
- The medial (middle ear) surface is multiphasic with significant pressure variations - essential for creating the pressure difference that drives ossicular movement.
- Incident sound from the EAC strikes the TM, sets up a travelling wave that is mainly collected at the rim of the membrane, conducted to the umbo, and then coupled to the manubrium of the malleus.
- At low frequencies: the TM transfers energy by uniform movement to the malleus.
- At high frequencies: movement is complex, and part of vibration is shunted by the middle ear.
Reflectance Properties:
- Below 1 kHz: high reflectance (inefficient transmission)
- 1-4 kHz: lowest reflectance (maximum energy delivery to cochlea - speech range)
- Above 4-7 kHz: reflectance rises again (limits high-frequency transmission)
The TM has a large effective vibrating surface area (~55 mm²) compared to the stapes footplate (~3.2 mm²), a ratio that is fundamental to the transformer mechanism (see below).
Clinical significance: Tympanic membrane perforations eliminate the multilever action and remove sound protection from the round window. A large perforation causes ~40-45 dB conductive hearing loss (central perforations cause less loss than marginal perforations since energy transfer is via the rim).
II. THE MIDDLE EAR
Components
- Tympanic cavity (air-filled)
- Ossicular chain (malleus, incus, stapes)
- Middle ear muscles (tensor tympani, stapedius)
- Eustachian tube
- Middle ear windows (oval window, round window)
1. The Ossicular Chain - The Transformer Mechanism
The three ossicles - malleus, incus, and stapes - form a linked mechanical chain that transmits vibration from the TM to the oval window. The middle ear acts as a mechanical transformer converting large-amplitude, low-force airborne vibrations into small-amplitude, high-force fluid vibrations in the cochlea.
Two mechanisms achieve this impedance transformation:
A. Hydraulic (Area) Ratio
The effective vibrating area of the tympanic membrane (~55 mm²) is far larger than the footplate of the stapes (~3.2 mm²). Bekesy calculated the effective ratio to be 17:1.
Since pressure = Force/Area, concentrating the same force from a large area to a small area multiplies pressure by 17 times.
B. Lever Ratio of the Ossicular Chain
The malleus and incus act as a lever system. The manubrium of the malleus (the longer arm) rotates about an axis passing through the anterior malleolar ligament and short process of the incus. The long process of the incus (the shorter arm) moves the stapes. The geometric length of the malleus is approximately 2.1 times that of the incus, yielding a lever ratio of 1.3:1 (velocity decreases, force increases by this factor).
Combined Transformer Ratio (Bekesy's Calculation):
Pressure gain = Hydraulic ratio × Lever ratio = 17 × 1.3 = 22 times ≈ 27 dB gain
This 27 dB gain nearly offsets the ~30 dB that would otherwise be lost at the air-fluid interface of the cochlea.
Frequency-dependent ossicular movement:
- Low frequencies: relatively rigid coupling between malleus and incus; stapes shows piston-like in-out movements
- High frequencies: complex spatial movements; some slippage between malleus-incus joint allows efficient conduction of higher frequencies; stapes moves along both long and short axes of the footplate
Clinical significance:
- Ossicular discontinuity: Loss of preferential sound delivery to oval window - conductive hearing loss up to 60 dB (less if incomplete or with pathological bridge)
- Ossicular fixation (e.g., otosclerosis, adhesive otitis media): Continuity maintained but mobility restricted; impedance increased; hearing loss less than discontinuity due to inbuilt redundancy
- Ossicle lever efficiency peaks at 2 kHz, optimized for speech
2. Middle Ear Muscles
A. Tensor Tympani (CN V - Trigeminal)
- Attaches to the manubrium of the malleus; pulls it anteromedially
- Has very low electrical activity in response to sound
- Active in response to: tactile stimulation of EAC/face, pneumatic pressure on eyelids, startle, swallowing, head movements, anticipation of loud sounds
- These stimuli involve bony skull movement that could stimulate the cochlea - tensor tympani acts as a pre-emptive protector in these situations
B. Stapedius (CN VII - Facial nerve) - THE ACOUSTIC REFLEX
The stapedius is the dominant middle ear muscle. It attaches to the neck of the stapes. Its contraction pulls the annular ligament of the stapes footplate, stiffening the ossicular chain.
Acoustic (Stapedial) Reflex:
- Elicited at 80-90 dB SL
- Primarily responds to high-intensity, low-frequency sounds (~0.8 kHz)
- Moves the stapes approximately 50 microns
- Increases stiffness of the ossicular chain
- Attenuates sound transmission to the inner ear by up to 30 dB
- Reflex arc: CN VIII → cochlear nucleus → both facial nuclei → CN VII → stapedius bilaterally (hence ipsilateral AND contralateral reflex)
- Latency: 100-200 ms (too slow to protect from impulse noises such as gunshots)
Three functions of the stapedial reflex:
- Cochlear protection from high-intensity sounds - preserves the dynamic range of the auditory system
- Reduction of high-intensity low-frequency output - prevents masking of high-frequency speech consonants at the cochlear base by forward-travelling cochlear waves
- Self-monitoring modulation - attenuates self-generated voice, preserving ambient sound quality during speech (explains why one's own voice sounds different when recorded)
Clinical significance: Absent stapedial reflex may indicate conductive hearing loss, sensorineural hearing loss (>70 dB), VIIth nerve palsy, or auditory neuropathy spectrum disorder (ANSD).
3. The Eustachian (Auditory) Tube
The Eustachian tube connects the middle ear to the nasopharynx. It is normally closed at rest but opens during swallowing, chewing, and yawning.
Three functions:
- Pressure equalization - maintains equal air pressure on both sides of the tympanic membrane. Unequal pressure renders the TM tense and unable to vibrate freely, causing conductive hearing loss.
- Mucociliary clearance - the middle ear mucosa is ciliated; secretions drain toward the nasopharynx.
- Middle ear protection - acts as a one-way valve preventing ascent of pharyngeal secretions and bacteria into the middle ear.
Clinical significance: Eustachian tube dysfunction underlies otitis media with effusion (glue ear), barotrauma, and negative middle ear pressure (TM retraction and atelectasis).
4. Middle Ear Windows
Oval Window
- Closed by the stapes footplate via the annular ligament
- Receives mechanical energy from the ossicular chain; transmits it to the perilymph of the scala vestibuli
- At the oval window, the 27 dB ossicular pressure gain far exceeds competitive pressure from the round window, ensuring directional cochlear fluid displacement
Round Window
- In the normal ear, acts as a pressure-relief opening at the opposite end of the cochlear duct
- Moves passively in the opposite phase to the stapes footplate, allowing maximum to-and-fro movement of the non-compressible cochlear fluid column
- Protected from direct sound impact by the intact TM, which damps sound and creates a phase difference
Clinical significance: In TM perforation, the round window loses its sound protection. Sound reaches both windows almost simultaneously, causing cancellation of perilymph movement - the basis for the 40-45 dB conductive loss seen in total TM perforation.
III. OVERALL SUMMARY - THE MIDDLE EAR AS AN IMPEDANCE MATCHING DEVICE
| Mechanism | Gain |
|---|---|
| EAC resonance gain | ~9 dB (at 2.7 kHz) |
| Hydraulic ratio (TM : stapes footplate area) | ~25 dB |
| Ossicular lever ratio (malleus : incus) | ~2.5 dB |
| Total middle ear transformer gain | ~27 dB |
| Sound pressure loss at air-fluid cochlear interface | ~30 dB |
| Net efficient transmission at 2.7 kHz | ~35.6 dB total gain vs 39.5 dB loss = efficient coupling |
The middle ear thus acts as a biological impedance matching transformer - converting low-pressure, large-amplitude airborne sound into high-pressure, small-amplitude fluid waves in the cochlea, enabling efficient cochlear transduction.
IV. APPLIED PHYSIOLOGY - SUMMARY TABLE
| Structure | Function | Effect of Pathology |
|---|---|---|
| Pinna | Sound capture, localization | Dysmorphia → conductive loss; poor localization |
| EAC | Resonance gain (~9 dB at 2.7 kHz); cerumen protection | Occlusion → 40 dB loss |
| Tympanic membrane | Multilever transducer; sound protection of round window | Perforation → 40-45 dB loss |
| Malleus-Incus lever | 1.3:1 mechanical gain | Fixation → ossicular conductive loss |
| TM:footplate area ratio | 17:1 hydraulic gain (×22 combined → 27 dB) | Discontinuity → up to 60 dB loss |
| Stapedius reflex | Cochlear protection, speech clarity, self-monitoring | Absent in VII palsy, ANSD |
| Tensor tympani | Pre-emptive protection from bone-conducted sound | Tensor tympani syndrome (rare) |
| Eustachian tube | Pressure equalization, drainage, protection | Dysfunction → OME, barotrauma |
| Oval window | Transmits energy to cochlear perilymph | Otosclerosis → stapes fixation |
| Round window | Pressure relief for cochlear fluid | Loss of protection → sound cancellation |
Conclusion
The external and middle ear together form a remarkably elegant acousto-mechanical system. The external ear captures, funnels, and resonates sound in the speech frequency range, providing ~9 dB of free gain. The middle ear overcomes the fundamental air-to-fluid impedance mismatch through a dual mechanism - the 17:1 hydraulic area ratio and the 1.3:1 ossicular lever ratio - yielding a combined transformer ratio of approximately 22 (27 dB). The middle ear muscles modulate this transmission dynamically for cochlear protection and speech clarity, while the Eustachian tube maintains the pressure conditions essential for normal TM vibration. Understanding these mechanisms is fundamental to the rational management of all conductive hearing disorders.
References:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2 - Applied Physiology of Hearing (Dasgupta)
- Shambaugh - Surgery of the Ear - Physiology of Middle Ear
- Ganong's Review of Medical Physiology, 26th Ed. - Chapter 11
This is a shared conversation. Sign in to Orris to start your own chat.