Static and dynamic compliance
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have rich, comprehensive content from multiple authoritative textbooks. Here is a complete, well-structured answer:
Static and Dynamic Compliance
Definition and Formula
Compliance is the change in volume (ΔV) produced per unit change in pressure (ΔP). It is the inverse of elastance (stiffness).
$$C = \frac{\Delta V}{\Delta P}$$
Normal total respiratory system compliance is approximately 100 mL/cmH₂O (lung alone ~200 mL/cmH₂O; chest wall alone ~200 mL/cmH₂O in series).
Static Compliance (C_static)
Static compliance is measured under conditions of no airflow - the lung is held at a fixed volume and pressures are allowed to equilibrate. It reflects pure elastic properties of the lung and chest wall, with no contribution from airway resistance or flow-resistive forces.
- Measured from the static pressure-volume curve (inflating the lung in steps and recording pressure at each volume when flow = 0)
- The plateau pressure on a ventilator (measured during an inspiratory pause with zero gas flow) mirrors static compliance
- Formula: C_static = Tidal Volume / (Plateau Pressure - PEEP)
- Normal value: ~60-100 mL/cmH₂O on a ventilator
Determinants of static compliance:
- Elastic tissue of the lungs (collagen, elastin fibers)
- Surface tension at the air-liquid interface of alveoli (accounts for ~two-thirds of elastic recoil)
- Chest wall elasticity
Dynamic Compliance (C_dynamic)
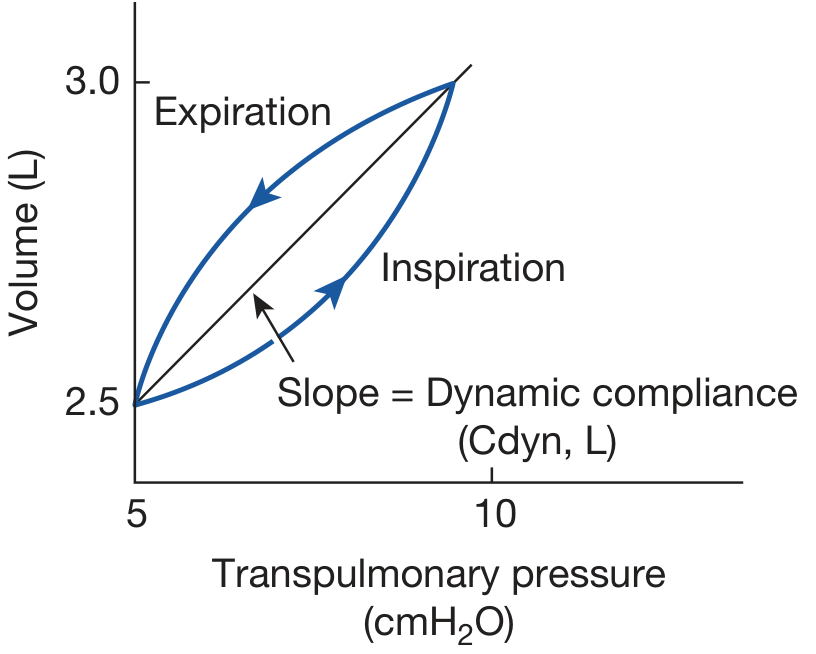
Dynamic compliance is measured during active airflow (during cyclic breathing). It is the change in lung volume divided by the change in transpulmonary pressure, measured at the points of zero airflow at end-inspiration and end-expiration during a breathing cycle.
$$C_{\text{dynamic}} = \frac{\Delta V_L}{-\Delta P_{IP}}$$
- The peak inspiratory pressure (PIP) on a ventilator provides an indication of dynamic compliance
- Formula: C_dynamic = Tidal Volume / (Peak Pressure - PEEP)
- Dynamic compliance incorporates both elastic recoil and airflow resistance effects
Measurement
The patient breathes through an esophageal balloon to measure transpulmonary pressure. A loop relating volume to transpulmonary pressure is generated during the breathing cycle. The slope of the line through the points of zero airflow (end-inspiration and end-expiration) = dynamic compliance.
Key Difference: Static vs Dynamic
| Feature | Static Compliance | Dynamic Compliance |
|---|---|---|
| Airflow during measurement | None (zero flow) | Present (cyclic) |
| Includes airway resistance | No | Yes |
| Ventilator correlate | Plateau pressure | Peak inspiratory pressure |
| What it reflects | Lung/chest wall elasticity alone | Elasticity + resistive forces |
| At zero frequency | Same as dynamic | Same as static |
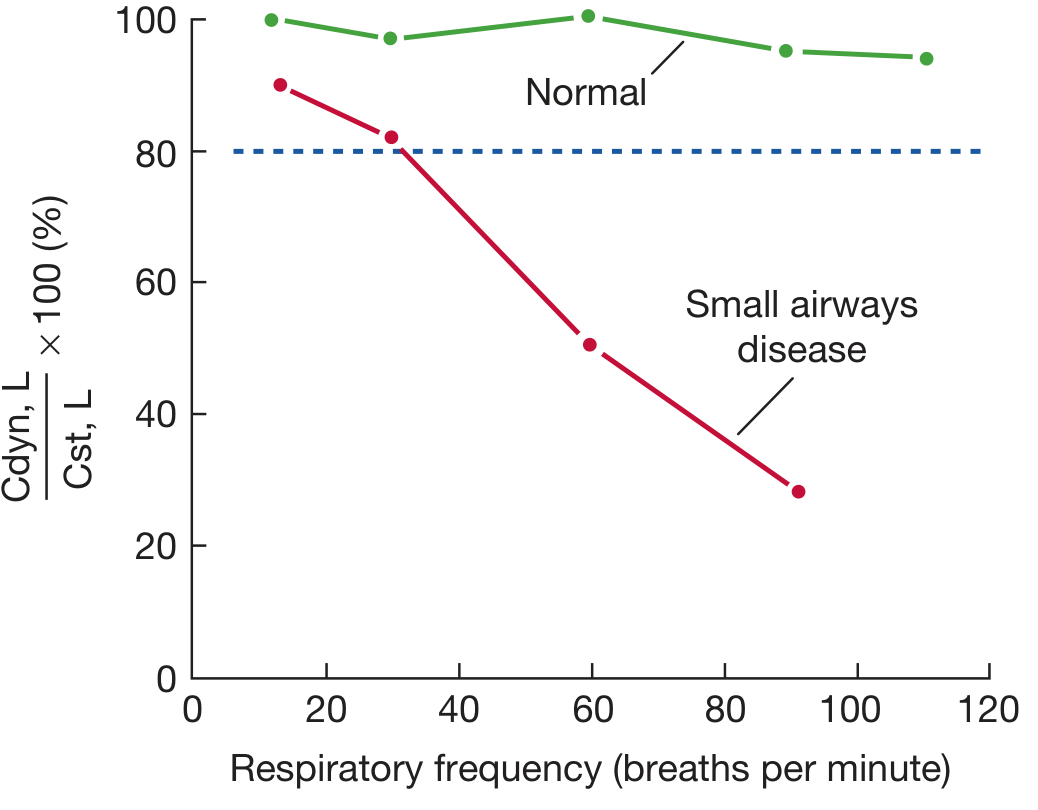
At a respiratory frequency of zero, static and dynamic compliance are identical. As frequency increases, C_dynamic falls below C_static, and the degree of divergence increases with airway resistance.
- In a normal lung: C_dynamic/C_static remains ≥80% even at frequencies >60 breaths/min
- In airway disease: C_dynamic falls progressively below C_static as breathing frequency increases
Frequency Dependence of Dynamic Compliance
This is a clinically important concept. Normally, dynamic compliance is independent of breathing frequency. However, when there is non-uniform ventilation (e.g., small airways disease), dynamic compliance falls as frequency increases - this is called frequency dependence of compliance.
Physiologic basis: In airways disease, some lung units have a longer time constant (RC product). At higher frequencies, inspiration terminates before these slow units can fill adequately, reducing the effective tidal volume and thus dynamic compliance. The lung behaves as if units "drop out" of ventilation at high frequencies.
Normal: Cdyn,L/Cst,L ≥ 80% at all frequencies
Small airways disease: Cdyn,L/Cst,L falls progressively below 80% as frequency rises
This is valid as a marker of small-airway disease only when static compliance and overall airway resistance are both normal. If either is abnormal, frequency dependence of dynamic compliance is merely another manifestation of the broader disease.
Clinical Correlation on Mechanical Ventilation
| Pressure Change | Likely Cause |
|---|---|
| Both PIP and plateau pressure increase | Decreased pulmonary compliance (e.g., pulmonary edema, pneumothorax, pleural effusion, ARDS, endobronchial intubation) |
| PIP increases, plateau pressure unchanged | Increased airway resistance (bronchospasm, secretions, kinked ETT, foreign body) |
The difference between PIP and plateau pressure represents the resistive component (flow x resistance). A large gap suggests high airway resistance; an elevated plateau alone points to low static compliance.
Diseases Affecting Compliance
| Condition | Compliance | Mechanism |
|---|---|---|
| Emphysema | Increased (high C_static) | Loss of elastic fibers; reduced recoil |
| Pulmonary fibrosis | Decreased | Stiffening of lung parenchyma |
| Pulmonary edema / ARDS | Decreased | Fluid-filled alveoli, surfactant dysfunction |
| Asthma | C_dynamic falls with frequency; C_static relatively normal | Increased R_AW with preserved elasticity |
| Neonatal RDS | Decreased | Surfactant deficiency; increased surface tension |
In emphysema, because C_static is elevated, a C_dynamic vs. frequency plot starts above normal (high initial C_dynamic) but then falls below C_static at higher frequencies, as long time-constant units fail to fill. In asthma, C_static is relatively preserved but C_dynamic falls sharply as R_AW rises.
Sources:
- Fishman's Pulmonary Diseases and Disorders, Dynamic Compliance section (pp. 592-593)
- Medical Physiology (Boron & Boulpaep), Ch. 27 - Effect of respiratory frequency on dynamic compliance
- Costanzo Physiology 7th Edition, Diseases of Lung Compliance
- Morgan and Mikhail's Clinical Anesthesiology 7e, Pressure & Volume Monitoring
This is a shared conversation. Sign in to Orris to start your own chat.