Types of apnea
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have very rich content from the textbooks and an excellent diagram. Let me compile the full answer.
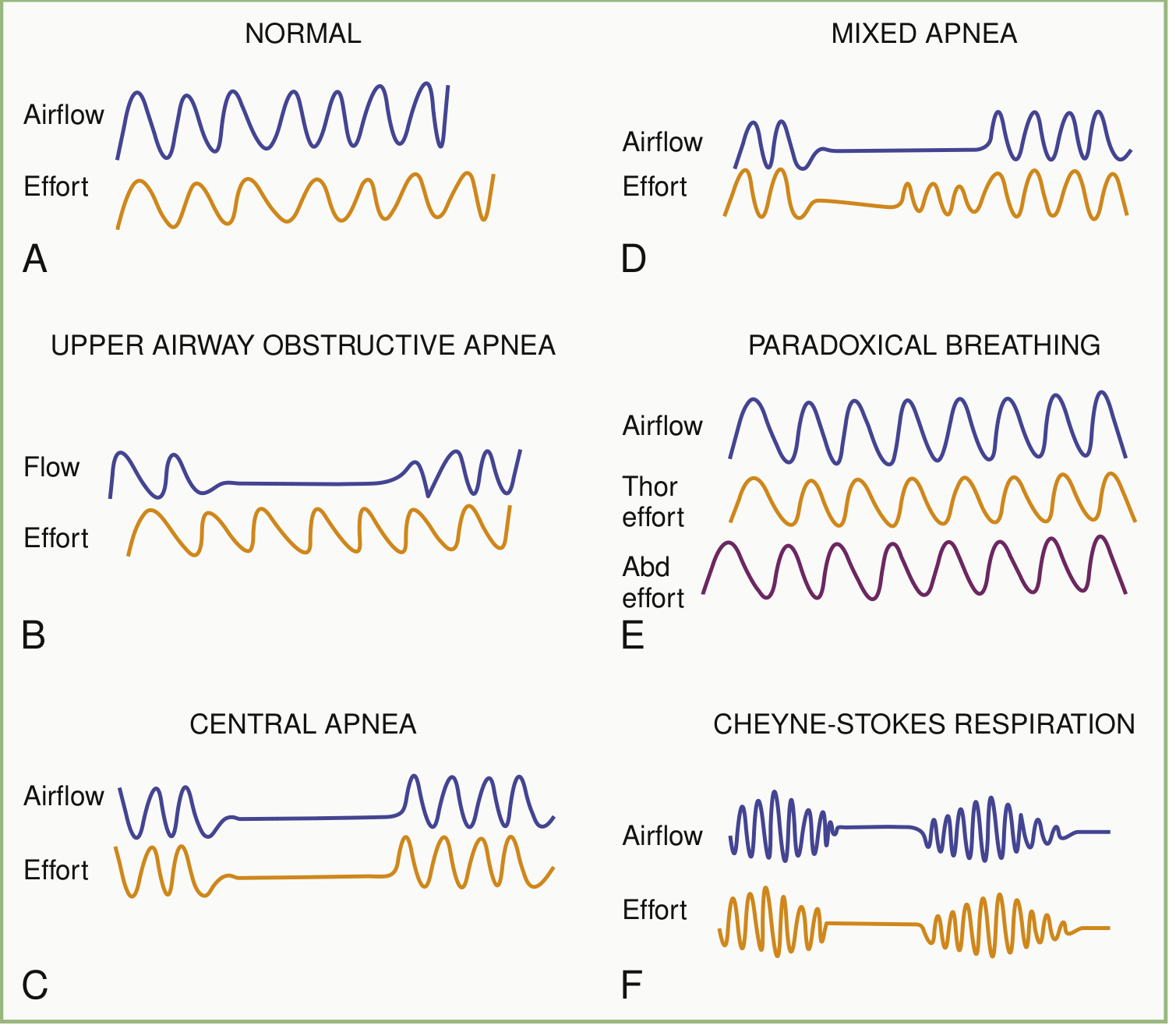
Types of Apnea
Apnea = cessation of airflow lasting at least 10 seconds (or >20 seconds in neonates, or any pause with bradycardia/cyanosis). There are three fundamental types based on mechanism, plus several clinically important subtypes.
1. Obstructive Apnea (OSA)
- Mechanism: The upper airway collapses during sleep. Airflow ceases despite continued - and increasingly forceful - thoracic and abdominal respiratory effort.
- Key feature on polysomnography: Airflow absent, but chest wall effort persists (see panel B in the diagram above).
- Pathophysiology: Chest wall restriction, upper airway narrowing, increased upper airway compliance, and impaired compensation for increased upper airway resistance. During REM sleep, descending neural inhibition of accessory ventilatory and upper airway muscles worsens obstruction.
- Clinical features: Loud chronic snoring, witnessed choking/gasping, excessive daytime somnolence (~50% of patients), morning headache, dry mouth, nocturia, mood disorders, and neurocognitive deficits.
- Cardiovascular consequences: Each obstructive event increases left and right ventricular afterload, decreases left ventricular compliance, raises pulmonary artery pressure, decreases coronary blood flow, and increases myocardial oxygen demand. The termination of each event causes a spike in heart rate and systemic blood pressure.
- Diagnosis: Apnea-Hypopnea Index (AHI) ≥5 events/hour on polysomnography (clinically significant cutoff, interpreted in context of symptoms and comorbidities).
2. Central Apnea (CSA)
- Mechanism: Absent or reduced respiratory effort from the brainstem - airflow and effort both disappear (see panel C in diagram).
- Key feature: PaCO2 falls to or below the apnea threshold during sleep, removing the chemical drive to breathe. Either PaCO2 falls too low, or the apnea threshold rises.
- Two major subtypes (classified by CO2 level):
A. Hypercapnic CSA
Impaired central respiratory drive or neuromuscular weakness affecting respiratory muscles. Wakefulness normally provides extra drive to breathe; when this "waking drive" is withdrawn at sleep onset, hypoventilation and apnea ensue. Most prominent during REM sleep.
B. Non-hypercapnic CSA
Augmented central respiratory drive leads to hyperventilation, which drives PaCO2 below the apnea threshold, triggering alternating periods of hyperventilation and apnea. Most prominent during NREM sleep.
- Cheyne-Stokes Respiration (CSR): The most clinically important form of non-hypercapnic CSA. Characterized by a waxing-waning (crescendo-decrescendo) breathing pattern separated by central apneas or hypopneas (see panel F in diagram). Most commonly associated with heart failure, where altered circulatory timing and augmented ventilatory responses to CO2 drive oscillation between apnea and hyperpnea. Associated with increased mortality.
- Complex/Treatment-emergent CSA: CSA that arises after CPAP treatment of OSA, or persists after treating a combination of obstructive, mixed, and central events.
3. Mixed Apnea
- Mechanism: Begins as a central apnea (no effort), followed by resumed respiratory effort against an obstructed airway (obstructive component). An initial central apnea followed by obstructive apnea (see panel D in diagram).
- Common in end-stage kidney disease, where the distribution of all three types (obstructive, central, mixed) is broader than in the general population.
4. Neonatal Apnea
A distinct clinical entity defined as a respiratory pause >20 seconds, or a shorter pause associated with cyanosis, pallor, hypotonia, or bradycardia <100 bpm. The same three mechanical subtypes apply:
| Subtype | Feature |
|---|---|
| Central | No diaphragmatic activity |
| Obstructive | Upper airway obstruction with effort present |
| Mixed | Combination of both |
- Apnea of prematurity: Occurs in most infants born at <28 weeks' gestation, ~20% born at 34 weeks, and <10% beyond 34 weeks. Usually resolves by 34-36 weeks postmenstrual age but may persist past term in those born at <25 weeks.
- Common causes: CNS abnormalities (seizures, meningitis, IVH), metabolic disturbances, sepsis, anemia, patent ductus arteriosus, reflux, thermal instability.
- Treatment: Caffeine (loading dose 5-6 mg/kg IV, maintenance 1-2 mg/kg/dose Q6-8h), CPAP, or mechanical ventilation.
5. Posthyperventilation Apnea
A brief central apnea occurring after voluntary hyperventilation causes a transient fall in PaCO2. Observed in comatose or neurologically impaired patients; the duration of apnea reflects the degree to which PaCO2 was lowered.
Special Neurological Breathing Patterns Related to Apnea
These occur with brainstem lesions and can include periods of apnea:
| Pattern | Mechanism/Location |
|---|---|
| Ataxic breathing | Clusters of cyclic breathing followed by apnea (apnea > ventilatory phase); brainstem lesion |
| Biot's breathing | Variant of ataxic: 2-3 equal breaths separated by long apneas |
| Apneustic breathing | Prolonged inspiration; caudal pontine lesion disconnecting apneustic center from pneumotaxic center |
| Cheyne-Stokes | Crescendo-decrescendo + central apneas; heart failure, bilateral cerebral lesions |
Summary Table
| Type | Airflow | Respiratory Effort | Key Association |
|---|---|---|---|
| Obstructive | Absent | Present (increasing) | Obesity, upper airway narrowing, snoring |
| Central | Absent | Absent | Heart failure (Cheyne-Stokes), opioids, brainstem disease |
| Mixed | Absent | Absent then present | Combination; common in ESKD |
| Neonatal | Pause >20 s | Variable | Prematurity; treated with caffeine |
| Posthyperventilation | Brief pause | Absent (transient) | Neurological impairment |
- Bradley and Daroff's Neurology in Clinical Practice, Section 101
- Murray & Nadel's Textbook of Respiratory Medicine, Chapter 121 (CSA) and Chapter 120 (OSA)
- Goldman-Cecil Medicine, Chapter 374
- The Harriet Lane Handbook, 23rd ed., Chapter 18
This is a shared conversation. Sign in to Orris to start your own chat.