ABG
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
I now have comprehensive material from multiple textbooks. Let me compile the full reference guide.
Arterial Blood Gas (ABG) - Comprehensive Overview
Normal ABG Values
| Parameter | Normal Range |
|---|---|
| pH | 7.35 - 7.45 |
| PaO2 | 80 - 100 mmHg |
| PaCO2 | 35 - 45 mmHg |
| HCO3- | 22 - 26 mEq/L |
| SaO2 | 95 - 100% |
| Base Excess (BE) | -2 to +2 mEq/L |
- pH < 7.35 = acidemia; pH > 7.45 = alkalemia
- An arterial sample is the gold standard - it reflects the blood after pulmonary circulation, before any peripheral gas exchange.
Henderson-Hasselbalch Equation
The foundation of ABG interpretation:
pH = pK + log ([HCO3-] / [0.03 × PaCO2])
pH is determined by the ratio of HCO3- to CO2. This means:
- Lungs regulate CO2 (fast, minutes)
- Kidneys regulate HCO3- (slow, hours to days)
(Costanzo Physiology 7th Ed., p. 330 | Rosen's Emergency Medicine)
Step-by-Step ABG Interpretation
Step 1 - Assess the pH
| pH | Interpretation |
|---|---|
| < 7.35 | Acidemia |
| 7.35 - 7.45 | Normal |
| > 7.45 | Alkalemia |
Step 2 - Identify the Primary Disorder
Look at PaCO2 and HCO3- together with the pH:
| pH | PaCO2 | HCO3- | Disorder |
|---|---|---|---|
| ↓ | ↑ | Normal/↑ | Respiratory Acidosis |
| ↑ | ↓ | Normal/↓ | Respiratory Alkalosis |
| ↓ | Normal/↓ | ↓ | Metabolic Acidosis |
| ↑ | Normal/↑ | ↑ | Metabolic Alkalosis |
If pH is normal but PaCO2 and HCO3- are both abnormal in opposite directions, a combined/mixed disorder is likely. (Washington Manual, p. 467)
Step 3 - Check Compensation
Compensation attenuates but does not fully correct the pH. An inappropriate response reveals a second (mixed) disorder.
| Primary Disorder | Expected Compensation |
|---|---|
| Metabolic Acidosis | PaCO2 decreases 1.2 mmHg per 1 mEq/L drop in HCO3- (or: expected PaCO2 = last 2 digits of pH) |
| Metabolic Alkalosis | PaCO2 increases 0.7 mmHg per 1 mEq/L rise in HCO3- |
| Respiratory Acidosis (Acute) | HCO3- rises 1 mEq/L per 10 mmHg rise in PaCO2 |
| Respiratory Acidosis (Chronic) | HCO3- rises 3.5 mEq/L per 10 mmHg rise in PaCO2 |
| Respiratory Alkalosis (Acute) | HCO3- falls 2 mEq/L per 10 mmHg drop in PaCO2 |
| Respiratory Alkalosis (Chronic) | HCO3- falls 5 mEq/L per 10 mmHg drop in PaCO2 |
(Washington Manual of Medical Therapeutics, Table 12-2)
Winter's Formula (for metabolic acidosis): Expected PaCO2 = (1.5 × HCO3-) + 8 ± 2 (Roberts and Hedges' Clinical Procedures in Emergency Medicine)
Step 4 - Calculate the Anion Gap (if metabolic acidosis is present)
AG = Na+ - (Cl- + HCO3-) Normal AG = 8-12 mEq/L (some labs use 10 ± 2)
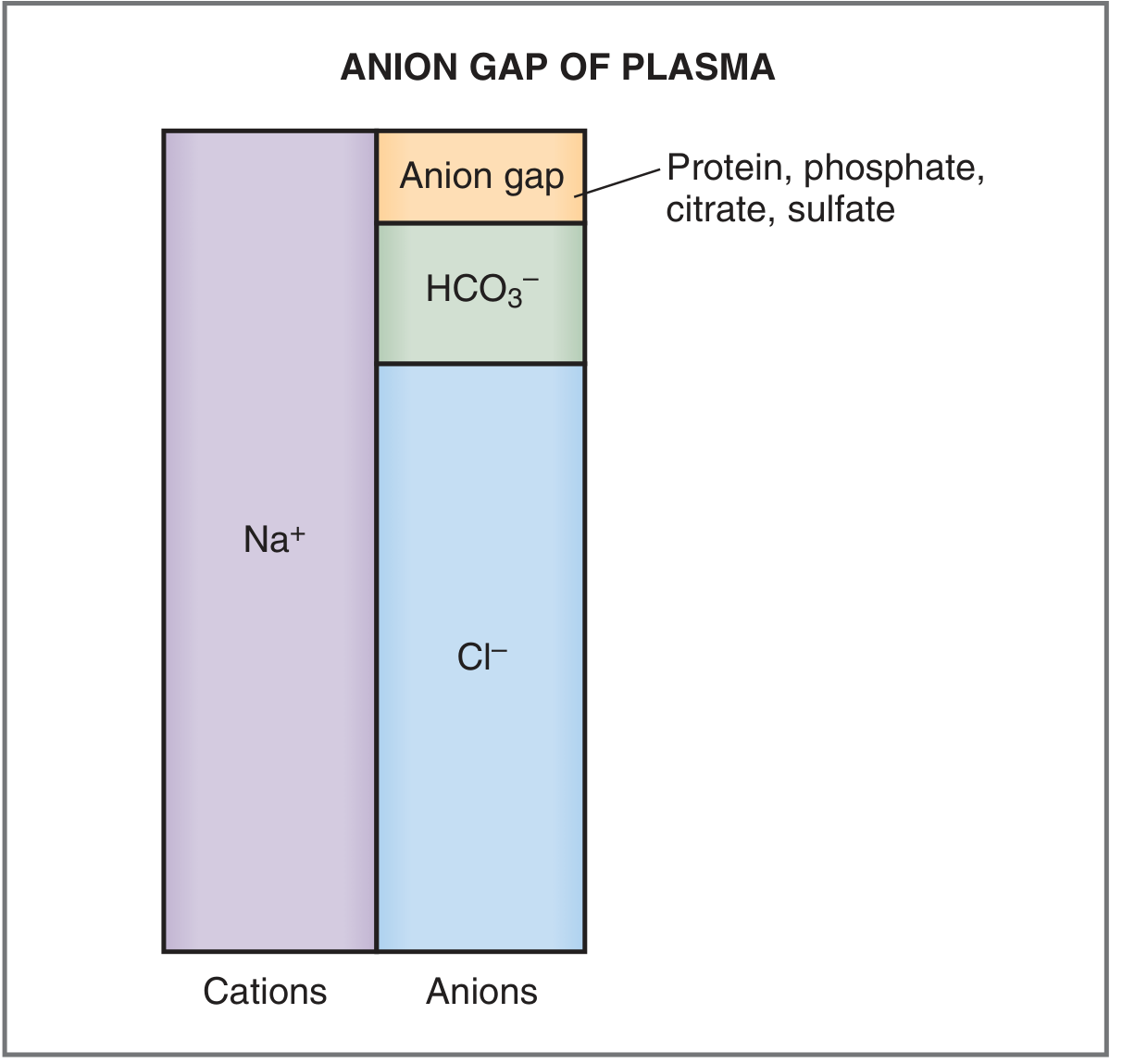
(Costanzo Physiology 7th Ed., Fig. 7.9)
The 4 Primary Acid-Base Disorders
1. Metabolic Acidosis
- Definition: Primary decrease in HCO3-, pH falls
- Compensation: Hyperventilation (lowers PaCO2)
- Two subtypes by anion gap:
High Anion Gap (AG > 12-15) - Mnemonic: MUDPILES
| Letter | Cause |
|---|---|
| M | Methanol |
| U | Uremia |
| D | DKA / Alcoholic ketoacidosis |
| P | Paraldehyde / Polyethylene glycol / Paracetamol (acetaminophen) |
| I | Iron |
| L | Lactic acidosis (most common, ~50% of cases) |
| E | Ethylene glycol |
| S | Salicylates |
Normal Anion Gap (Hyperchloremic) - Mnemonic: HARDUP
| Letter | Cause |
|---|---|
| H | Hyperalimentation / Hospital saline |
| A | Acid infusion / Addison disease / Carbonic Anhydrase Inhibitors |
| R | Renal tubular acidosis (RTA) |
| D | Diarrhea |
| U | Ureterosigmoidostomy |
| P | Pancreatic drainage / fistula |
(Rosen's Emergency Medicine)
Osmolar gap tip: If high AG acidosis + osmolar gap → suspect methanol or ethylene glycol poisoning. High molecular weight acids (lactate, ketoacids, salicylate) typically do NOT produce osmolar gaps.
Delta-Delta Ratio (for high AG metabolic acidosis)
- Checks for a hidden concurrent metabolic alkalosis or normal AG acidosis
- Delta-Delta = (AG - 12) / (24 - HCO3-)
- < 0.4: pure non-AG acidosis
- 0.4-0.8: mixed AG + non-AG acidosis
- 1-2: pure AG metabolic acidosis
-
2: AG metabolic acidosis + metabolic alkalosis
2. Metabolic Alkalosis
- Definition: Primary rise in HCO3-, pH rises
- Compensation: Hypoventilation (raises PaCO2)
- Causes divided by urine chloride response:
Chloride-Responsive (urine Cl- < 20 mEq/L - responds to NS):
- Vomiting, NG suction
- Chloride-wasting diarrhea
- Villous adenoma
- Diuretic use
Chloride-Unresponsive (urine Cl- > 20 mEq/L - does NOT respond to NS):
- Primary hyperaldosteronism
- Cushing syndrome
- Bartter / Gitelman syndrome
- Severe hypokalemia
(Rosen's Emergency Medicine)
3. Respiratory Acidosis
- Definition: Primary rise in PaCO2 (hypoventilation), pH falls
- Compensation: Renal HCO3- retention (takes 3-5 days for chronic)
- Causes: COPD exacerbation, neuromuscular disease, opioid overdose, chest wall disorders, severe pneumonia, upper airway obstruction
4. Respiratory Alkalosis
- Definition: Primary fall in PaCO2 (hyperventilation), pH rises
- Compensation: Renal HCO3- excretion
- Causes: Anxiety, pain, fever, PE, salicylate toxicity (early), pregnancy, liver failure, iatrogenic hyperventilation
ABG vs Venous Blood Gas (VBG)
| Parameter | Correlation |
|---|---|
| pH | VBG closely correlates with ABG (±0.05 units) - usually acceptable substitute |
| PaCO2 | VBG trends along with ABG (varies up to ±20 mmHg); normal VBG CO2 reliably predicts normal PaCO2 |
| PaO2 | VBG cannot substitute for ABG oxygenation assessment |
| Lactate | Venous works for normal/markedly elevated values; mildly elevated venous lactate may not correlate |
(Tintinalli's Emergency Medicine)
Important Clinical Pearls
-
Pulse oximetry cannot detect hypoventilation in patients on supplemental oxygen - the oxyhemoglobin dissociation curve's flat upper portion means PaO2 can fall significantly with rising PaCO2 while SpO2 remains normal. An ABG or capnography is required in that setting.
-
pH normal with abnormal PaCO2 and HCO3- = always suspect a mixed disorder.
-
Lactic acidosis is the most common cause of high AG metabolic acidosis (~50% of cases).
-
Bicarbonate therapy in metabolic acidosis: commonly used to target pH > 7.10 in severe cases, or > 7.20 with concurrent AKI. Optimal use remains debated.
-
Acute vs. Chronic respiratory disorders: renal compensation takes days, so acute respiratory acidosis will show a more abnormal pH (less HCO3- compensation) than the same degree of chronic hypercapnia.
Sources: Costanzo Physiology 7th Ed. | Rosen's Emergency Medicine | Tintinalli's Emergency Medicine | Washington Manual of Medical Therapeutics | Murray & Nadel's Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.