Streptococcus
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a comprehensive overview of Streptococcus drawn from Medical Microbiology 9e and supporting textbooks.
Streptococcus
Classification and Overview
Streptococci are Gram-positive cocci arranged in chains (short chains in clinical specimens, longer chains in broth media). They are catalase-negative (distinguishing them from staphylococci) and are broadly classified by:
-
Hemolysis pattern on blood agar:
- α-hemolysis (partial/green): S. pneumoniae, viridans streptococci
- β-hemolysis (complete/clear): S. pyogenes (Group A), S. agalactiae (Group B)
- γ-hemolysis (none): enterococci
-
Lancefield grouping (cell-wall carbohydrate antigens): Groups A through H, K through V
Streptococcus pyogenes (Group A Streptococcus, GAS)
Trigger words: Group A, pharyngitis, pyoderma, rheumatic fever, glomerulonephritis, "flesh-eating bacteria"
Structure and Virulence
| Factor | Function |
|---|---|
| M protein (type-specific) | Resists opsonization; class I M proteins trigger rheumatic fever |
| Hyaluronic acid capsule | Antigenically similar to mammalian tissue; resists phagocytosis |
| C5a peptidase | Inactivates complement component C5a |
| Lipoteichoic acid + F protein | Bind fibronectin on host cells; mediate adhesion |
| Streptolysin O (SLO) | Oxygen-labile cytotoxin; antibodies = ASO titer |
| Streptolysin S (SLS) | Oxygen-stable; responsible for β-hemolysis on plates |
| Streptococcal pyrogenic exotoxins (SPE A, B, C) | Superantigens; cause scarlet fever and TSS |
| Streptokinase | Dissolves fibrin clots; spreads infection |
| DNases (A-D) | Depolymerize DNA in pus; anti-DNase B titer used for diagnosis |
| Streptokinase | Activates plasminogen, aiding spread |
Epidemiology
- Transient colonization of the upper respiratory tract and skin
- Spreads by respiratory droplets (pharyngitis) or direct skin contact (pyoderma)
- Highest-risk groups:
- Children 5-15 years: pharyngitis
- Children 2-5 years with poor hygiene: pyoderma
- Patients with prior pharyngitis: rheumatic fever, glomerulonephritis
Diseases
Suppurative (pus-forming):
- Pharyngitis - most common bacterial cause; exudative tonsillitis, fever, cervical lymphadenopathy
- Scarlet fever - pharyngitis + SPE-mediated diffuse erythematous rash, strawberry tongue
- Impetigo/Pyoderma - superficial skin infection; honey-crusted lesions
- Erysipelas - acute skin infection with raised, sharply demarcated borders; systemic signs; predominantly in young children and the elderly, now more common on the legs
- Cellulitis - deeper skin + subcutaneous tissue; borders less defined than erysipelas
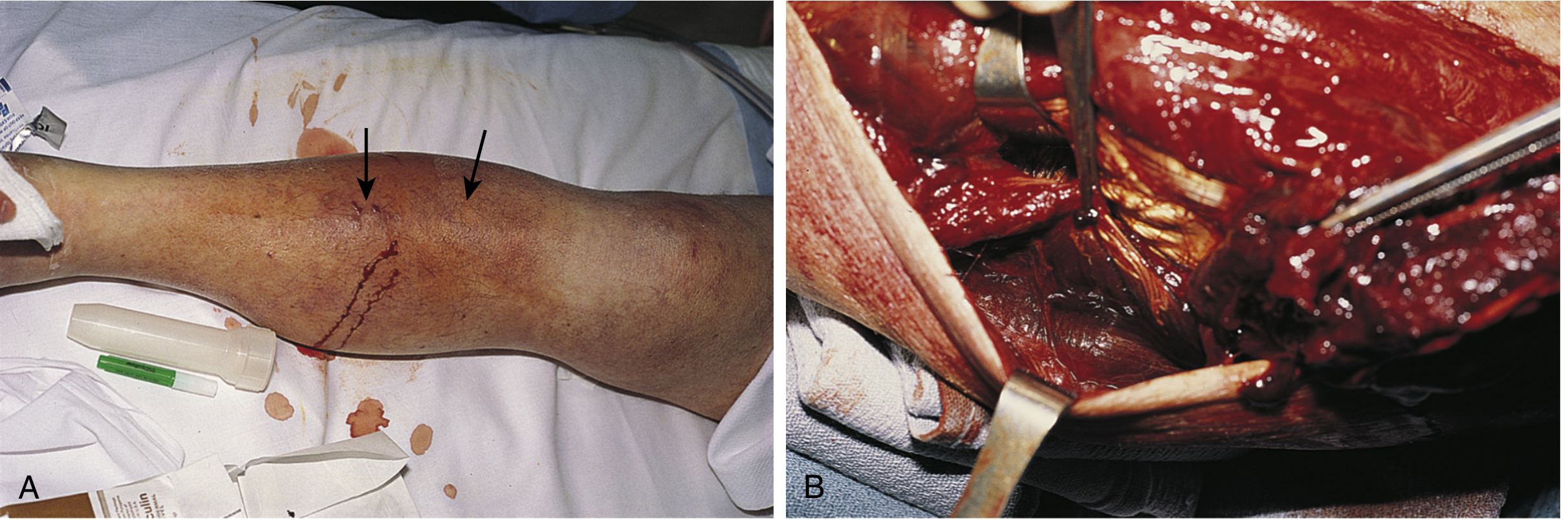
- Necrotizing fasciitis ("flesh-eating bacteria") - deep infection spreading along fascial planes; rapid destruction of fat and muscle; bullae, gangrene, multiorgan failure; requires urgent surgical debridement

Streptococcal Toxic Shock Syndrome (STSS):
- SPE superantigens activate massive T-cell cytokine release
- Fever, hypotension, multiorgan failure
- Bacteremia often detectable
Nonsuppurative (post-infectious):
| Complication | Trigger | Mechanism |
|---|---|---|
| Rheumatic fever | Pharyngitis only (NOT skin) | Molecular mimicry: anti-M protein antibodies cross-react with cardiac tissue; only class I M protein strains implicated |
| Acute glomerulonephritis | Pharyngitis OR pyoderma | Immune complex deposition in glomeruli |
Diagnosis
- Rapid antigen detection test (RADT) - for pharyngitis; quick, specific
- Throat culture on blood agar - gold standard for pharyngitis; β-hemolytic colonies, susceptible to bacitracin, PYR-positive
- ASO titer - elevated after pharyngitis; confirms rheumatic fever or glomerulonephritis from throat infection
- Anti-DNase B titer - elevated after both pharyngitis and pyoderma; used when glomerulonephritis follows skin infection (ASO may be negative)
- Culture from impetigo - scrape under crusted lesion; do not swab open draining pustules (risk of staphylococcal contamination)
Treatment
- Drug of choice: Oral penicillin V or amoxicillin (S. pyogenes has never developed penicillin resistance)
- Penicillin allergy: oral cephalosporin or macrolide (note increasing erythromycin/azithromycin resistance)
- Severe systemic infections: IV penicillin + clindamycin (clindamycin inhibits toxin synthesis)
- Necrotizing fasciitis: urgent surgical debridement + IV penicillin + clindamycin
- No vaccine currently available
Streptococcus agalactiae (Group B Streptococcus, GBS)
Key features: Neonatal disease (sepsis, meningitis, pneumonia); UTI and bacteremia in pregnant women and immunocompromised adults.
- Treatment: Penicillin G (drug of choice); empirical broad-spectrum coverage (cephalosporin + aminoglycoside) until identified
- Prevention: Intrapartum penicillin given at least 4 hours before delivery in colonized mothers; no vaccine available
Streptococcus pneumoniae (Pneumococcus)
Trigger words: Diplococci, capsule, pneumonia, meningitis, vaccine
Structure and Virulence
| Factor | Function |
|---|---|
| Polysaccharide capsule | Primary virulence factor; resists phagocytosis; basis of serotyping (>90 serotypes) |
| Pneumolysin | Cytotoxin; stimulates inflammation |
| IgA protease | Destroys secretory IgA; aids mucosal colonization |
| Teichoic acid (C polysaccharide) | Activates complement; drives inflammation |
Morphology
Elongated Gram-positive cocci in pairs (diplococci) and short chains. Identified by: catalase-negative, susceptibility to optochin (distinguishes from viridans streptococci), bile solubility, α-hemolysis.
Epidemiology and Diseases
- Disease arises from endogenous spread from colonized nasopharynx/oropharynx (person-to-person spread via droplets is rare)
- Colonization highest in young children and their contacts
- Risk factors: viral respiratory infection, functional asplenia, sickle cell disease, hematologic malignancy
- Diseases: Pneumonia, otitis media, sinusitis, meningitis, bacteremia/sepsis
- Children and elderly at greatest risk for meningitis
- Asplenic patients at risk for fulminant pneumococcal sepsis
Diagnosis
- Gram stain (highly sensitive) + culture on sheep blood agar
- Antigen tests for C polysaccharide: sensitive in CSF (meningitis), but NOT reliable in urine
- Nucleic acid-based tests preferred for meningitis (especially post-antibiotic)
Treatment and Prevention
- Empirical therapy for meningitis: vancomycin + ceftriaxone
- Susceptible isolates: cephalosporin, fluoroquinolone, or vancomycin as monotherapy
- Vaccines:
- PCV13 (13-valent conjugated): Recommended for all children < 2 years and certain adults
- PPSV23 (23-valent polysaccharide): Recommended for adults at risk (elderly, asplenic, immunocompromised)
Viridans Streptococci
- α-hemolytic or non-hemolytic; optochin-resistant (distinguishes from S. pneumoniae)
- Normal flora of the oropharynx, GI tract, and genitourinary tract
- Five groups: Mutans, Salivarius, Anginosus, Mitis, Sanguinis
- Key diseases:
- Infective endocarditis - especially after dental procedures in patients with valvular abnormalities
- Dental caries - S. mutans
- Intraabdominal/brain abscesses - Anginosus group
Comparative Summary Table
| Feature | S. pyogenes (Gp A) | S. agalactiae (Gp B) | S. pneumoniae | Viridans |
|---|---|---|---|---|
| Hemolysis | β | β | α | α/γ |
| Lancefield | A | B | None (C polysaccharide) | None |
| Optochin | Resistant | Resistant | Sensitive | Resistant |
| Bacitracin | Sensitive | Resistant | Resistant | Resistant |
| PYR | Positive | Negative | Negative | Negative |
| Key disease | Pharyngitis, RF, GN | Neonatal sepsis | Pneumonia, meningitis | Endocarditis |
| Vaccine | No | No | Yes (PCV13/PPSV23) | No |
| Treatment | Penicillin V | Penicillin G | Vancomycin + ceftriaxone (meningitis) | Penicillin |
Sources: Medical Microbiology 9e (Murray et al.); Goldman-Cecil Medicine; Robbins & Kumar Basic Pathology
Short and important
Streptococcus - High-Yield Summary
Classification
| Group | Species | Hemolysis | Key ID |
|---|---|---|---|
| A | S. pyogenes | β | Bacitracin-S, PYR+ |
| B | S. agalactiae | β | CAMP test+ |
| - | S. pneumoniae | α | Optochin-S, bile soluble |
| - | Viridans | α/γ | Optochin-R |
| D | Enterococcus | γ | PYR+, bile-R |
S. pyogenes (Group A) - Most Tested
Virulence factors to memorize:
- M protein - antiphagocytic; class I M protein → Rheumatic fever
- Streptolysin O (SLO) - oxygen-labile; ASO titer measures antibodies
- Streptolysin S (SLS) - β-hemolysis on blood agar plates
- SPE (A,B,C) - superantigens → scarlet fever, STSS
- Hyaluronic acid capsule - antiphagocytic
Diseases:
- Pharyngitis → Rheumatic fever (throat only, NOT skin)
- Pyoderma/Impetigo → Glomerulonephritis (throat OR skin)
- Scarlet fever, Erysipelas, Cellulitis
- Necrotizing fasciitis (surgical emergency)
Diagnosis:
- Rapid antigen test (pharyngitis)
- ASO titer → RF or GN after pharyngitis
- Anti-DNase B → GN after skin infection
Treatment: Penicillin V (never resistant); severe = Penicillin + Clindamycin
S. pneumoniae - Most Common Cause Of
- Community-acquired pneumonia
- Bacterial meningitis (adults)
- Otitis media (children)
Key features: Diplococci, optochin-sensitive, bile soluble, polysaccharide capsule (>90 serotypes), IgA protease
Risk: Asplenia → fulminant sepsis
Treatment: Vancomycin + Ceftriaxone (meningitis)
Vaccine: PCV13 (children), PPSV23 (adults at risk)
S. agalactiae (Group B)
- Neonatal sepsis/meningitis/pneumonia
- UTI in pregnant women
- CAMP test positive
- Prevention: intrapartum penicillin (≥4 hrs before delivery)
- Treatment: Penicillin G
Key Distinctions (Exam Traps)
| Point | Answer |
|---|---|
| RF after skin infection? | Never - only pharyngitis |
| GN after skin infection? | Yes |
| Penicillin-resistant? | Never for S. pyogenes |
| Optochin sensitive = ? | S. pneumoniae |
| PYR positive = ? | S. pyogenes, Enterococcus |
| Bacitracin sensitive = ? | S. pyogenes only |
| CAMP test positive = ? | S. agalactiae |
This is a shared conversation. Sign in to Orris to start your own chat.