Explain dangerous area of face for my anatomy exam of 1st year MBBS
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, exam-ready answer. Here it is:
Dangerous Area of the Face
Definition and Boundaries
The dangerous area of the face (also called the "danger triangle" or "danger zone") is the region bounded by:
- Upper lip and nose - roughly a triangular zone with its apex at the root of the nose (glabella/nasion) and its base along the upper lip
Some sources extend it slightly to include the nasolabial folds. The key anatomical reason this area is dangerous is the valveless venous communication between the facial veins here and the intracranial cavernous sinus.
"The upper lip and nose are considered the danger area of the face because infections in this region may be transmitted in a retrograde fashion through a valveless venous system to the cavernous sinus."
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Why Is It Dangerous? - The Key Anatomy
The danger arises because infections (boils, furuncles, carbuncles, pimples, cellulitis) in this region can spread retrograde (backwards) through venous channels into the cavernous sinus, causing cavernous sinus thrombosis - a life-threatening complication.
The Critical Venous Pathway

There are two main routes by which infection spreads from this danger area to the cavernous sinus:
Route 1: Via the Angular Vein → Ophthalmic Vein → Cavernous Sinus
- Infection from upper lip/nose enters the facial vein
- The facial vein originates at the medial corner of the eye as the angular vein (formed by confluence of the supratrochlear and supraorbital veins)
- The angular vein communicates with the superior ophthalmic vein
- The superior ophthalmic vein drains directly into the cavernous sinus
Route 2: Via the Deep Facial Vein → Pterygoid Plexus → Cavernous Sinus
- The facial vein in the cheek communicates with the deep facial vein
- The deep facial vein connects with the pterygoid plexus of veins
- The pterygoid plexus communicates with the cavernous sinus via emissary veins passing through the foramen ovale and foramen lacerum
Why Can Blood Flow Backwards?
This is the critical point for your exam:
There are NO valves in the facial vein or any other venous channels of the head.
This means blood (and therefore infection) can flow in any direction - including retrograde (backwards) towards the cavernous sinus. Normally blood flows downward, but during infection with increased pressure, septic thrombi can travel upward intracranially.
Anatomy of the Cavernous Sinus (What Makes Its Thrombosis So Serious)
The cavernous sinus lies on either side of the sella turcica and pituitary gland. Its contents explain the catastrophic signs of cavernous sinus thrombosis:
| Structure | Location in/near Sinus | Clinical Effect if Involved |
|---|---|---|
| Internal carotid artery | Passes through sinus | Arterial compromise, stroke |
| Abducent nerve (CN VI) | Passes through the interior of the sinus | Lateral rectus palsy (most sensitive sign - eye cannot abduct) |
| Oculomotor nerve (CN III) | Lateral wall of sinus | Ptosis, dilated pupil, "down and out" eye |
| Trochlear nerve (CN IV) | Lateral wall of sinus | Superior oblique palsy |
| Ophthalmic nerve (CN V1) | Lateral wall of sinus | Loss of sensation over forehead/eye |
| Maxillary nerve (CN V2) | Lateral wall of sinus | Loss of sensation over cheek |
Memory tip: CN VI is MOST commonly and EARLIEST affected because it lies within the sinus itself (not protected by the wall), making lateral gaze palsy (inability to abduct the eye) the most sensitive sign.
Cavernous Sinus Thrombosis - Clinical Features
When infection spreads from the danger area to the cavernous sinus, the following features appear:
- Severe constitutional disturbance - high fever, rigors, toxemia
- Proptosis (forward protrusion of the eyeball) - due to venous obstruction
- Chemosis (conjunctival edema)
- Periorbital edema
- Ophthalmoplegia - paralysis of ocular muscles (squint)
- Lateral rectus palsy (CN VI affected first - most sensitive sign)
- Headache, nausea, vomiting
- Altered consciousness in severe cases
- Usually becomes bilateral (both sides) - distinguishes from orbital cellulitis
"Diagnosis of such complication is made by noting severe constitutional disturbances, proptosis, squint and paralysis of the ocular muscles, especially the rectus lateralis which is supplied by the abducent nerve."
- S. Das, A Manual on Clinical Surgery
Key Exam Points Summary
| Point | Detail |
|---|---|
| Location | Triangle: apex at root of nose, base at upper lip (upper lip + nose) |
| Key reason | Valveless veins - no valves in facial vein or head veins |
| Route 1 | Facial vein → Angular vein → Superior ophthalmic vein → Cavernous sinus |
| Route 2 | Facial vein → Deep facial vein → Pterygoid plexus → Cavernous sinus (via foramen ovale/lacerum) |
| Most dangerous infection | Boil/furuncle on upper lip or nose - do NOT squeeze it |
| Complication | Cavernous sinus thrombosis (septic) |
| Earliest sign of CST | Lateral rectus palsy (CN VI - abducent nerve) |
| Why CN VI first? | It lies inside the sinus, not in its wall |
| Classic saying | "Never squeeze a pimple in the dangerous area of the face" |
Sources: Gray's Anatomy for Students (Gray's, p. 7334-7344); Scott-Brown's Otorhinolaryngology (vol. 1, p. 6419-6429); S. Das Manual on Clinical Surgery (p. 457-471); Color Atlas of Human Anatomy Vol. 2 (p. 1395-1400)
Explain circle of Willis for my 1st year anatomy exam
Finding Sources
Finding Sources
Reading File
Reading File
With its digram and image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have rich content and two excellent diagrams. Let me compile the comprehensive exam answer.
Circle of Willis - Complete 1st Year MBBS Anatomy Guide
Introduction
The Circle of Willis (cerebral arterial circle) is a polygonal anastomotic ring of arteries located at the base of the brain, in the interpeduncular cistern of the subarachnoid space. It connects the anterior circulation (from internal carotid arteries) with the posterior circulation (from vertebral-basilar system), providing collateral pathways to protect the brain from ischemia if one vessel is occluded.
Diagrams
Figure 1 - Circle of Willis and all major branches (inferior view of brain):
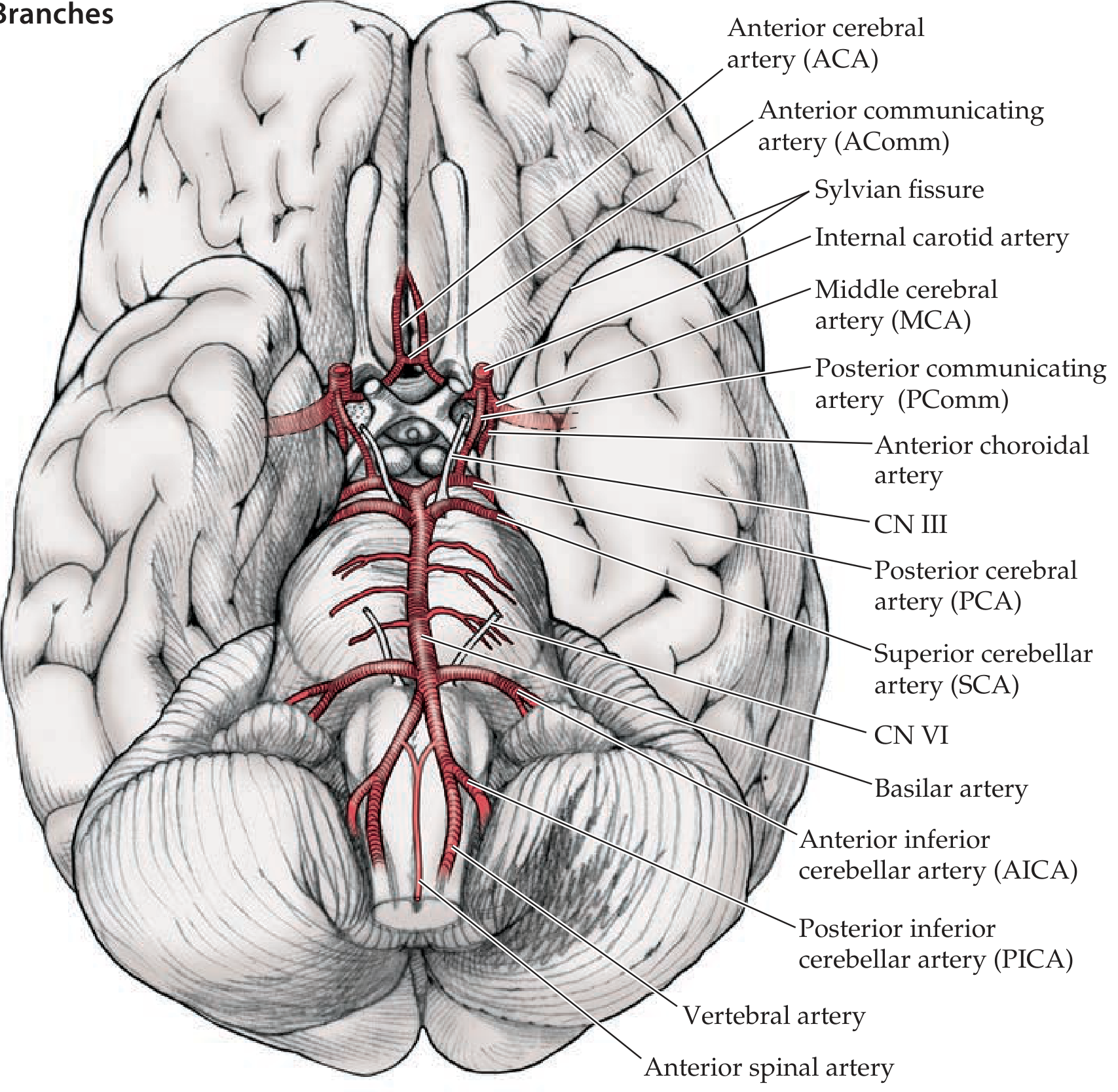
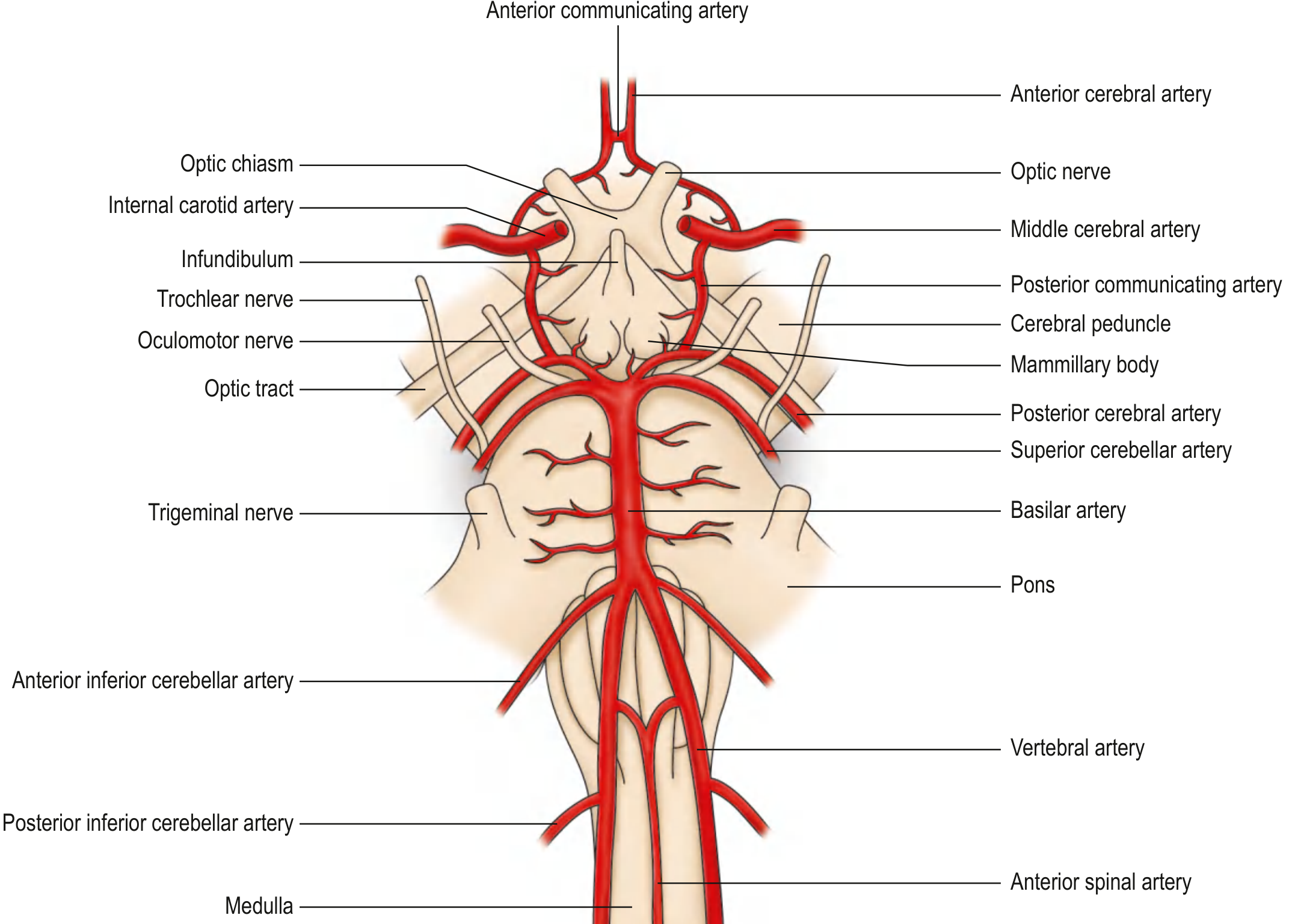
Figure 2 - Detailed schematic showing relationship to brainstem structures:
Blood Supply to the Brain - Two Circulations
The brain receives blood from two sources:
| Circulation | Source Vessels | Forms |
|---|---|---|
| Anterior | Left & Right Internal Carotid Arteries (ICA) | ACA + MCA |
| Posterior | Left & Right Vertebral Arteries → fuse to form Basilar Artery | PCA |
Both circulations meet and anastomose to form the Circle of Willis.
Components of the Circle of Willis
The circle has 3 paired vessels and 2 unpaired communicating vessels = 8 vessels total forming the ring:
Anterior Part (from Internal Carotid Arteries)
- Anterior Cerebral Artery (ACA) - right and left (paired) - terminal branches of ICA
- Anterior Communicating Artery (ACoA) - single, unpaired - connects the two ACAs across the midline
Middle Part (the lateral "struts")
- Internal Carotid Artery (ICA) - right and left supraclinoid portions (the "inflow" vessels)
- Posterior Communicating Artery (PCoA) - right and left (paired) - links ICA to PCA, joining anterior to posterior circulation
Posterior Part (from Basilar Artery)
- Posterior Cerebral Artery (PCA) - right and left (paired) - terminal branches of the basilar artery
"The two anterior cerebral arteries are connected by the anterior communicating artery. The posterior communicating arteries connect the supraclinoid internal carotid arteries with the proximal posterior cerebral arteries."
- Goldman-Cecil Medicine, 22E
Schematic of the Circle
ACoA (anterior communicating artery)
|
ACA ——[left]——[right]—— ACA
| |
ICA (left) ICA (right)
| |
PCoA (left) PCoA (right)
| |
PCA (left) ——Basilar—— PCA (right)
|
Vertebral arteries (L + R)
The shape is roughly a hexagon (some say heptagon) when drawn out.
The Three Main Cerebral Arteries and What They Supply
These are the branches that arise FROM the circle and actually supply the brain tissue:
1. Anterior Cerebral Artery (ACA)
- Passes anteriorly then curves back over the corpus callosum through the interhemispheric fissure
- Supplies: Medial frontal lobe, medial parietal lobe, sensorimotor cortex for the lower limb
- Deep branches (lenticulostriate/Heubner's artery): anterior limb of internal capsule, head of caudate, anterior putamen
- Stroke effect: Contralateral leg weakness/sensory loss (leg cortex is on medial surface)
2. Middle Cerebral Artery (MCA)
- Largest branch of ICA; passes laterally into the Sylvian (lateral) fissure
- Supplies: Entire lateral surface of the cerebral hemisphere - face, arm, and trunk sensorimotor cortex; Broca's area (dominant hemisphere); Wernicke's area; visual radiation
- Deep branches: lenticulostriate arteries supplying internal capsule (posterior limb) and basal ganglia
- Stroke effect: Contralateral face + arm weakness, aphasia (if dominant side)
3. Posterior Cerebral Artery (PCA)
- Terminal branch of basilar artery; wraps around the cerebral peduncle
- Supplies: Occipital lobe (primary visual cortex), medial-inferior temporal lobe, thalamus, midbrain
- Stroke effect: Contralateral homonymous hemianopia (visual field defect); thalamic infarct
Mnemonic for Branches of ICA (Supraclinoid)
OPAAM
- O - Ophthalmic artery
- P - Posterior communicating artery
- A - Anterior choroidal artery
- A - Anterior cerebral artery
- M - Middle cerebral artery
Function of the Circle of Willis
The circle acts as an equalizer and collateral safety net:
- Under normal conditions, blood from anterior and posterior circulations does not mix (pressures are equal)
- When one vessel is occluded, the circle allows collateral flow to bypass the blockage
- In a person with a complete circle of Willis, "the entire intracranial circulation can be supplied by a single patent internal carotid artery or vertebral artery" - Goldman-Cecil Medicine
Important Variations (Exam Favourite)
A complete circle of Willis exists in only ~34% of individuals. Common variants:
| Variant | Description |
|---|---|
| Hypoplastic A1 segment | One ACA's proximal part is small/absent; both ACAs fed from one ICA |
| "Fetal" PCA | P1 segment absent; PCA territory supplied by ICA via PCoA instead of basilar |
| Hypoplastic PCoA | Reduces communication between anterior & posterior circulation |
Clinical Importance - Key Exam Points
1. Berry (Saccular) Aneurysms
- Most common site for intracranial aneurysms
- Form at bifurcation points of the circle due to haemodynamic stress and congenital medial weakness
- Common sites: ACoA > PCoA > MCA bifurcation
- Rupture causes subarachnoid haemorrhage (SAH) - "worst headache of life"
2. PCoA Aneurysm and CN III Palsy
- An enlarging PCoA aneurysm can compress the oculomotor nerve (CN III) as it passes nearby
- Signs: ptosis, dilated pupil, "down and out" eye - a neurosurgical emergency
3. Stroke Localization
- Knowing what each artery supplies allows you to localize a stroke from clinical signs
Summary Table for Quick Revision
| Vessel | Origin | Supplies | Stroke Deficit |
|---|---|---|---|
| ACA | ICA | Medial frontal/parietal (leg area) | Contralateral leg weakness |
| MCA | ICA | Lateral hemisphere (face, arm, speech) | Face + arm weakness, aphasia |
| PCA | Basilar | Occipital lobe, thalamus | Homonymous hemianopia |
| ACoA | Between ACAs | Communicating vessel only | Aneurysm - SAH, personality change |
| PCoA | ICA to PCA | Communicating vessel only | Aneurysm - CN III palsy |
Sources: Neuroanatomy through Clinical Cases, 3rd Ed. (p. 5772-5817); Goldman-Cecil Medicine, 22E (p. 1861-1883); Miller's Anesthesia, 10E (p. 1655-1665); Gray's Anatomy for Students (eFig. 9.35)
Generate a quick reference PDF of Circle of Willis anatomy for exam prep
Reading File
Running Command
Running Command
Writing File
Running Command
Running Command
Your PDF is ready! Here it is:
Circle of Willis Quick Reference
PDF Document · PDF
Here's what's packed into the single A4 page reference:
- Title banner - colour-coded header with subtitle
- Schematic diagram - hand-drawn style Circle of Willis with all vessels labelled and colour-coded:
- Red = anterior circulation (ICA, ACA, MCA)
- Orange = communicating arteries (ACoA, PCoA)
- Purple = posterior/vertebrobasilar (vertebrals, basilar, PCA)
- Components table - all 9 vessels, their origin and position in the circle
- Three main cerebral arteries - course, cortical supply, deep supply, and stroke deficit for ACA / MCA / PCA
- Mnemonics - OPAAM for branches of ICA; vessel count memory aid
- Clinical correlates - berry aneurysm, PCoA/CN III palsy, stroke syndromes, incomplete circle
- Quick revision summary - 10 high-yield bullet points for last-minute review
- Source citations at the footer
This is a shared conversation. Sign in to Orris to start your own chat.