Anatomy of liver
Reading File
Finding Sources
Searching Images
liver anatomy lobes segments
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Now I have comprehensive information from Schwartz's Principles of Surgery and Guyton & Hall. Let me compile the full anatomy answer.
Anatomy of the Liver
Overview
The liver is the largest organ in the body, weighing approximately 1,500 g (about 2% of total body weight). It resides in the right upper abdominal cavity beneath the diaphragm, protected by the rib cage, and has a reddish-brown color. It is surrounded by a fibrous sheath called Glisson's capsule.
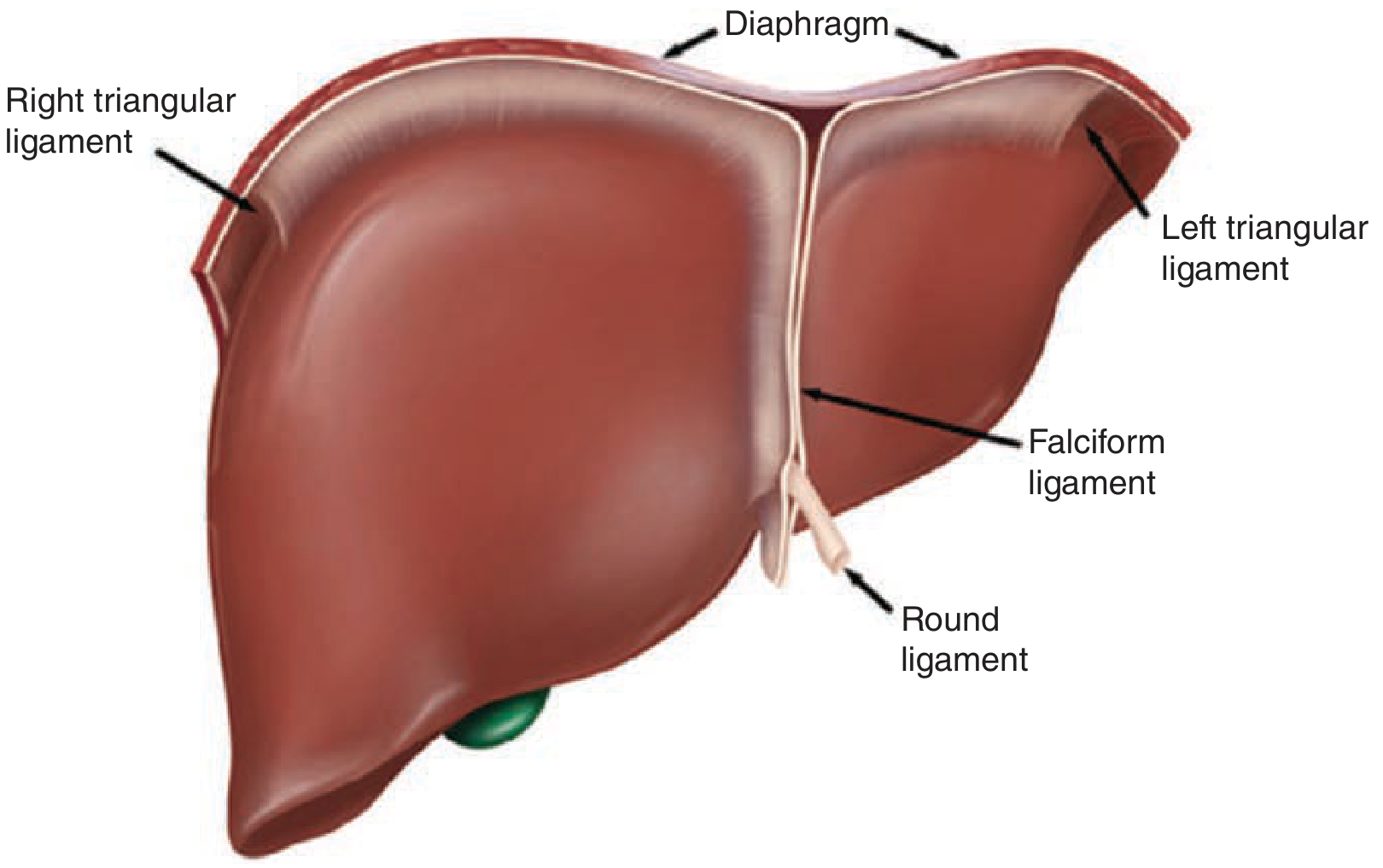
Ligaments & Peritoneal Attachments
The liver is held in place by several ligaments:
| Ligament | Description |
|---|---|
| Round ligament (ligamentum teres) | Remnant of the obliterated umbilical vein; enters the left liver hilum at the front edge of the falciform ligament |
| Falciform ligament | Separates the left lateral from the left medial segment along the umbilical fissure; anchors the liver to the anterior abdominal wall |
| Ligamentum venosum (Arantius' ligament) | Obliterated ductus venosus; lies deep between the caudate lobe and left lateral segment |
| Left & right triangular ligaments | Secure the two sides of the liver to the diaphragm |
| Coronary ligaments | Extend anteriorly from the triangular ligaments; the right coronary ligament also anchors the liver to the right retroperitoneum |
| Hepatoduodenal ligament (porta hepatis) | Contains the common bile duct, hepatic artery, and portal vein |
| Gastrohepatic ligament | Connects the liver to the lesser curvature of the stomach |
The foramen of Winslow (epiploic foramen) lies deep and to the right of the porta hepatis, connecting to the lesser sac. Clamping the hepatoduodenal ligament here (the Pringle maneuver) achieves complete vascular inflow control.
Lobar & Segmental Anatomy (Couinaud)
Traditional Lobes
The liver is grossly divided into right and left lobes by Cantlie's line — an imaginary plane from the gallbladder fossa to the inferior vena cava (IVC). The right lobe accounts for 60–70% of liver mass; the left lobe and caudate lobe make up the remainder.
The falciform ligament does NOT separate right from left lobes — it divides the left lateral segment from the left medial segment.
Couinaud's 8 Segments
The French anatomist Couinaud (1950s) divided the liver into 8 functional segments, each with its own independent portal pedicle (portal vein branch + hepatic artery + bile duct) and drained by a hepatic vein. Segments are numbered clockwise beginning with the caudate lobe (I):
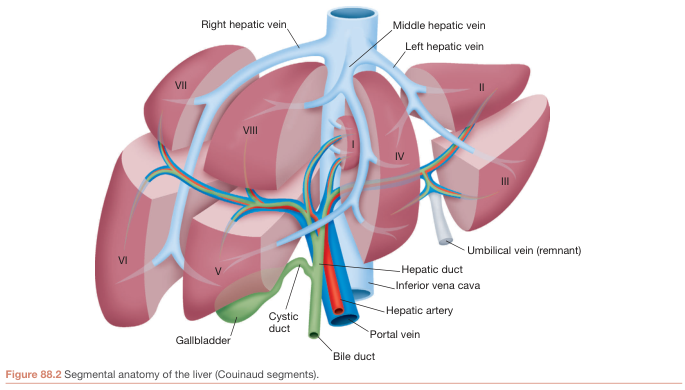
| Segment | Location |
|---|---|
| I | Caudate lobe (3 subsegments: Spiegel lobe, paracaval portion, caudate process) |
| II & III | Left lateral segment |
| IV (IVa/IVb) | Left medial segment; IVa = cephalad, IVb = caudad (near gallbladder) |
| V & VI | Right lobe, inferior (anterior and posterior sectors) |
| VII & VIII | Right lobe, superior (anterior and posterior sectors) |
Hepatic veins further subdivide the liver into four sectors (Bismuth):
- Right hepatic vein: separates right posterolateral from right anterolateral sector
- Middle hepatic vein: runs in the main fissure (Cantlie's line), separating right and left livers
- Left hepatic vein: separates left posterior from left anterior sector
Surgical relevance: a right hepatectomy removes segments V, VI, VII, VIII; leaving I–IV.
Blood Supply (Dual)
The liver receives ~1,350 mL/min of blood (≈27% of resting cardiac output):
| Vessel | Contribution | Source |
|---|---|---|
| Portal vein | ~75% (~1,050 mL/min) | Confluence of splenic vein + superior mesenteric vein (SMV) |
| Hepatic artery | ~25% (~300 mL/min) | Celiac trunk → common hepatic artery → hepatic artery proper → right & left hepatic arteries |
Hepatic Artery Variants
"Classic" anatomy (celiac → common hepatic → hepatic proper) is present in only ~76% of individuals. Common variants:
- Replaced/accessory right hepatic artery from SMA: 10–15% (travels posterior to portal vein)
- Replaced/accessory left hepatic artery from left gastric artery: 3–10% (runs in gastrohepatic ligament)
- Cystic artery usually arises from the right hepatic artery within Calot's triangle
Portal Pressure
- Portal vein pressure: ~9 mmHg
- Hepatic vein pressure: ~0 mmHg
- This low resistance gradient enables the enormous flow through sinusoids
Venous Drainage
Three hepatic veins drain into the inferior vena cava (IVC):
- Right hepatic vein — drains segments V–VIII
- Middle hepatic vein — drains segments IV, V, VIII
- Left hepatic vein — drains segments II, III
The caudate lobe (segment I) drains directly into the IVC via multiple small veins — making it functionally independent and often spared in Budd–Chiari syndrome.
Biliary Drainage
- Bile canaliculi between adjacent hepatocytes → bile ductules → intrahepatic bile ducts
- Right hepatic duct + Left hepatic duct → common hepatic duct
- Common hepatic duct + cystic duct (from gallbladder) → common bile duct
- The left hepatic duct has a longer extrahepatic course than the right
- 30–40% of individuals have non-standard bile duct confluence (accessory or aberrant ducts)
The gallbladder sits adherent to segments IVb (left lobe) and V (right lobe).
Microanatomy: The Liver Lobule
The basic functional unit is the hepatic lobule — a cylindrical structure 0.8–2 mm in diameter. The human liver contains 50,000–100,000 lobules.
Structure:
- Central vein at the core → drains to hepatic veins → IVC
- Hepatic cell plates radiate outward (each plate is ~2 cells thick)
- Hepatic sinusoids lie between the plates; blood flows from portal tracts → sinusoids → central vein
- Portal tracts at the periphery (portal venule + hepatic arteriole + bile duct)
- Bile canaliculi run between hepatocytes in the opposite direction to blood flow → to bile ducts at the periphery
Special cells lining the sinusoids:
- Endothelial cells — have very large pores (~1 µm), allowing plasma proteins to pass freely
- Kupffer cells (resident macrophages) — phagocytize bacteria and foreign matter
- Space of Disse — perisinusoidal space between endothelium and hepatocytes; connects with lymphatic vessels
Innervation
| Type | Source |
|---|---|
| Parasympathetic | Left vagus (anterior hepatic branch) + right vagus (posterior hepatic branch) |
| Sympathetic | Greater thoracic splanchnic nerves via celiac ganglia |
The right phrenic nerve is a common source of referred pain to the right shoulder and scapula from liver/diaphragm irritation. Notably, the denervated liver after transplantation functions with normal capacity.
Sources: Schwartz's Principles of Surgery 11e, pp. 1374–1378; Guyton and Hall Textbook of Medical Physiology, p. 860; Gray's Anatomy for Students, p. 401; Bailey and Love's Short Practice of Surgery 28e, p. 1618.
Anatomy of pancreas
Finding Sources
Searching Images
pancreas anatomy parts relations blood supply
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive information from Mulholland & Greenfield's Surgery, Yamada's Textbook of Gastroenterology, and Guyton & Hall. Let me compile the full anatomy answer.
Anatomy of the Pancreas
Overview
The pancreas is a soft, tan-colored retroperitoneal organ serving both exocrine (digestive enzyme secretion) and endocrine (hormonal regulation of glucose) functions. It lies deep in the upper retroperitoneum, posterior to the stomach and transverse colon, and anterior to the great vessels of the abdomen. Its intimate relationship with major vessels and neighboring organs makes it one of the most surgically challenging abdominal organs.
- Exocrine tissue: ~90–95% of gland mass (acinar + ductal cells)
- Endocrine tissue: ~1–2% of mass, but receives 15% of pancreatic blood flow (islets of Langerhans)
Parts of the Pancreas
The pancreas has five parts — head, neck, body, tail, and the uncinate process:
| Part | Location & Key Relations |
|---|---|
| Head | Nestled in the concavity of the 2nd and 3rd parts of the duodenum; contains the common bile duct and the main pancreatic duct |
| Uncinate process | Hook-like extension of the head projecting behind the superior mesenteric vessels |
| Neck | Short segment overlying the superior mesenteric vein (SMV) and portal vein confluence |
| Body | Extends to the left, lies posterior to the stomach; crossed anteriorly by the transverse mesocolon |
| Tail | Passes anterior to the left kidney and adrenal gland; terminates near the splenic hilum (intraperitoneal, in the splenorenal ligament) |
Relations
Posterior Relations
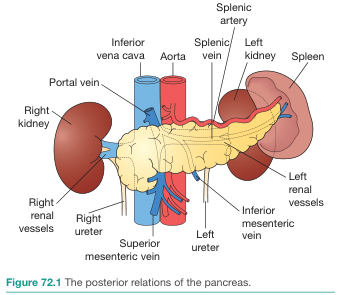
| Posterior Structure | Related Part of Pancreas |
|---|---|
| Inferior vena cava (IVC) | Head |
| Aorta | Head/neck |
| Portal vein (formed behind neck) | Neck |
| Superior mesenteric vein & artery | Behind neck / uncinate |
| Splenic vein (runs along superior border) | Body and tail |
| Left kidney & adrenal gland | Tail |
| Bilateral ureters | Body (deep) |
The Superior mesenteric artery (SMA) and Superior mesenteric vein (SMV) run directly behind the neck of the pancreas. The SMV joins the splenic vein here to form the portal vein — a critical surgical landmark.
Anterior Relations
- Stomach (lesser sac separates it from the body of the pancreas)
- Transverse colon/mesocolon
- First part of the duodenum (head)
Ductal Anatomy
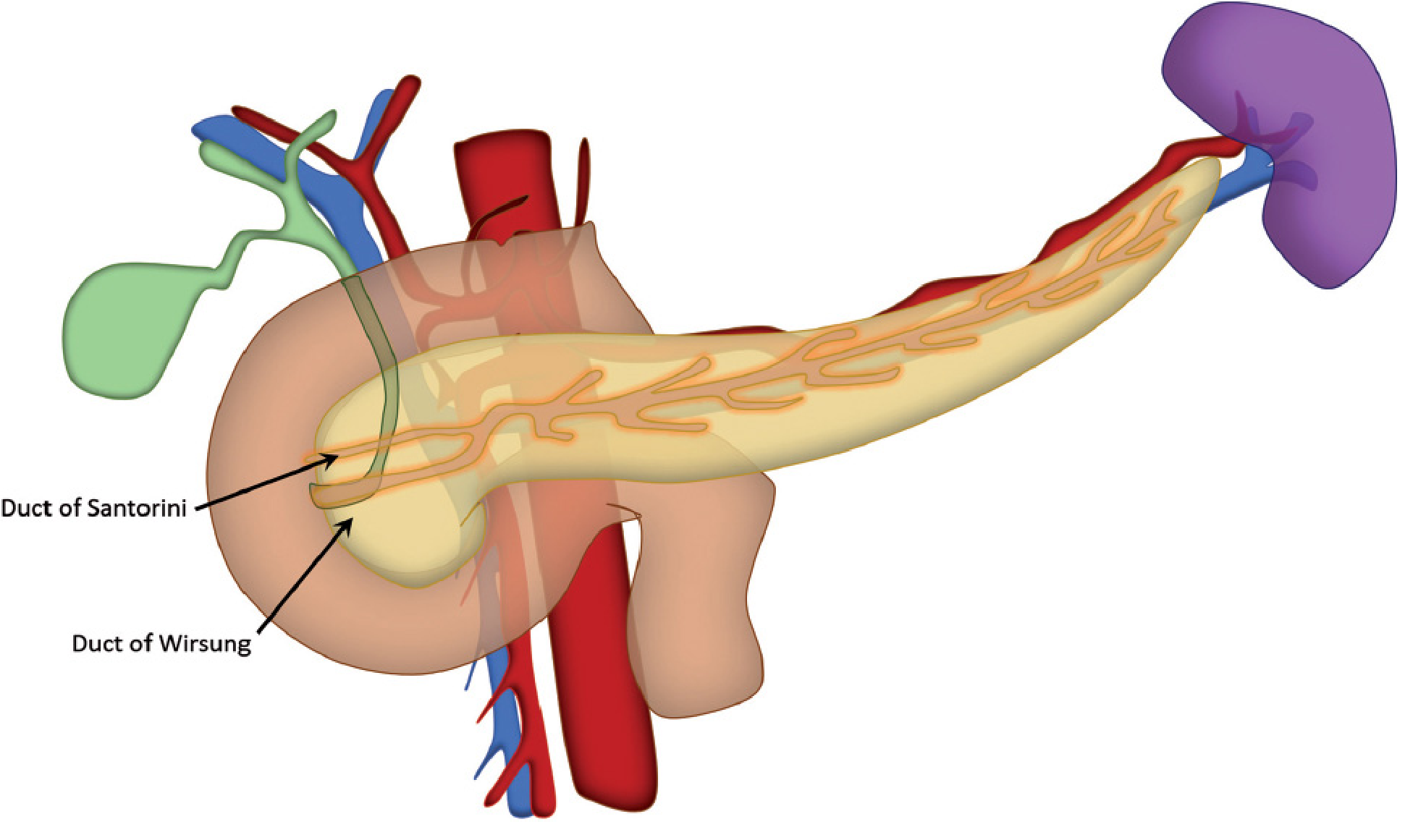
| Duct | Description |
|---|---|
| Duct of Wirsung (main pancreatic duct) | Runs the full length of the gland; joins the common bile duct at the ampulla of Vater → drains via the major papilla into the 2nd part of the duodenum |
| Duct of Santorini (accessory pancreatic duct) | Proximal remnant of the dorsal bud duct; drains via the minor papilla, ~2 cm proximal to the major papilla |
The main duct diameter is normally ≤3 mm in the head and ≤2 mm in the body/tail; dilation suggests obstruction.
Blood Supply
Arterial Supply
The pancreas has a rich, dual arterial supply:
Head & Uncinate Process — supplied by pancreaticoduodenal arcades:
- Superior pancreaticoduodenal artery (anterior + posterior branches) — from the gastroduodenal artery (branch of common hepatic artery)
- Inferior pancreaticoduodenal artery (anterior + posterior branches) — from the superior mesenteric artery (SMA)
Neck, Body & Tail — supplied by branches of the splenic artery:
- Dorsal pancreatic artery
- Great pancreatic artery (arteria pancreatica magna) — largest branch to the body
- Caudal pancreatic arteries
- Transverse (inferior) pancreatic artery
Venous Drainage
Mirrors the arterial supply; veins drain into:
- Portal vein / SMV (head and neck)
- Splenic vein (body and tail)
The splenic vein runs in a groove along the posterior surface of the pancreas body and tail before joining the SMV behind the neck to form the portal vein.
Lymphatic Drainage
The central retroperitoneal position of the pancreas allows lymphatic drainage along several major routes:
- Splenic nodes (body and tail)
- Hepatic nodes (head)
- Superior mesenteric nodes (head and uncinate)
- Aortocaval nodes and other posterior abdominal wall lymphatics
This multi-directional drainage explains the early and widespread lymph node involvement in pancreatic cancer.
Innervation
- Parasympathetic: Vagus nerve (stimulates both exocrine and endocrine secretion)
- Sympathetic: Greater thoracic splanchnic nerves via the celiac plexus → pancreatic nerve plexus (posterior to pancreas)
- The celiac plexus surrounds the celiac axis and is the target of celiac plexus neurolysis for intractable pancreatic cancer pain
Microanatomy
Exocrine Component (~90–95% of mass)
| Cell Type | Location | Function |
|---|---|---|
| Acinar cells | Central acinus | Produce and secrete digestive enzymes (amylase, lipase, proteases) |
| Centroacinar cells | Junction of acinus and duct | Secrete NaHCO₃ solution |
| Ductal cells | Ductal network | Secrete bicarbonate-rich fluid; flush enzymes into duodenum |
Endocrine Component — Islets of Langerhans (~1–2% of mass)
The human pancreas contains 1–2 million islets, each ~0.3 mm in diameter, organized around small capillaries.
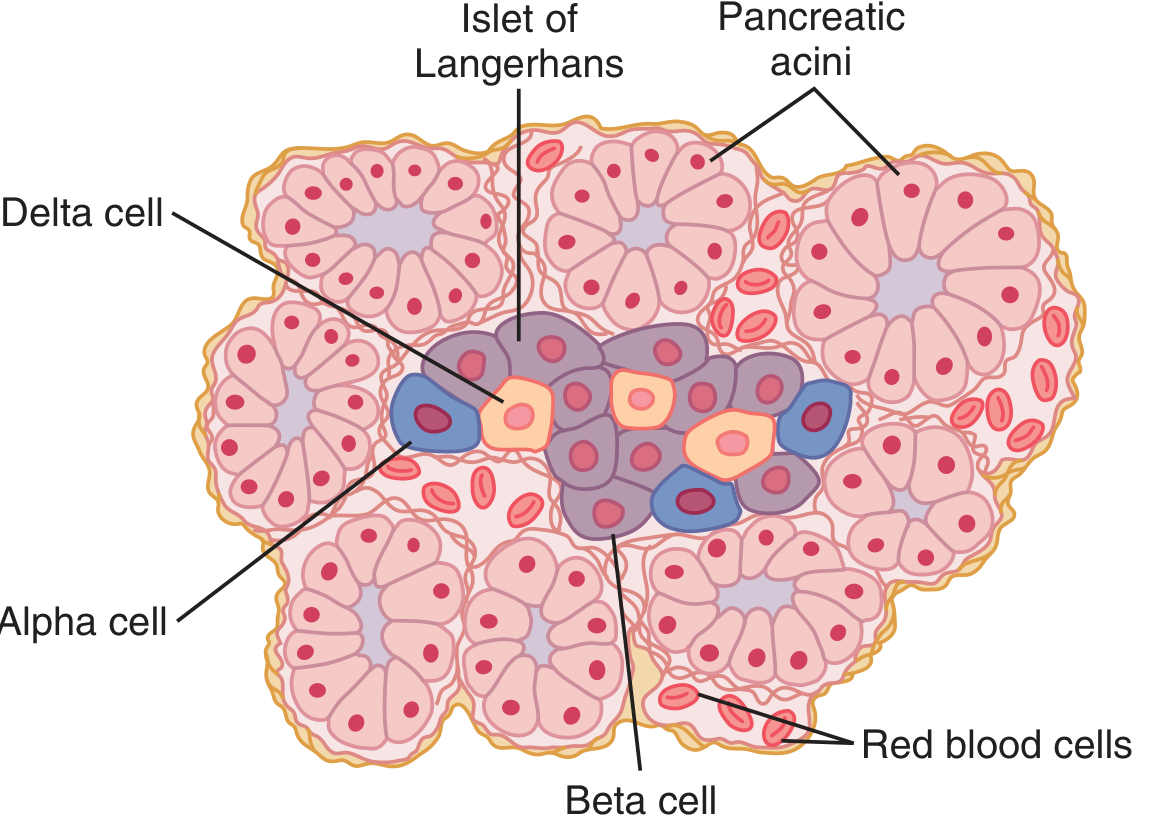
| Cell Type | % of Islet Cells | Hormone Secreted | Function |
|---|---|---|---|
| Beta (β) cells | ~60% (center of islet) | Insulin + Amylin (IAPP) | Lowers blood glucose; promotes glycogen/fat storage |
| Alpha (α) cells | ~25% (periphery) | Glucagon | Raises blood glucose (glycogenolysis, gluconeogenesis) |
| Delta (δ) cells | ~10% | Somatostatin | Inhibits both insulin and glucagon secretion; slows intestinal transit |
| PP cells | Small | Pancreatic polypeptide | Inhibits pancreatic exocrine secretion |
Paracrine interactions: Insulin inhibits glucagon; amylin inhibits insulin; somatostatin inhibits both.
Embryology
The pancreas develops from two endodermal buds at the junction of foregut and midgut (first apparent at 4 weeks gestation):
| Bud | Gives rise to |
|---|---|
| Dorsal bud (larger) | Superior head, neck, body, and tail; duct of Santorini |
| Ventral bud | Inferior head and uncinate process; duct of Wirsung |
As the duodenum rotates, the ventral bud rotates clockwise to fuse with the dorsal bud. The two ducts fuse, with the main duct draining through the ampulla of Vater (major papilla).
Congenital Variants
| Anomaly | Mechanism | Clinical Significance |
|---|---|---|
| Pancreas divisum | Incomplete fusion of dorsal + ventral ducts (<5% of population) | Dorsal duct drains via minor papilla; ~5% develop pancreatitis |
| Annular pancreas | Bifid ventral bud rotates in opposite directions, encircling the 2nd part of duodenum (~1/1,000) | Can cause duodenal obstruction; associated with Down syndrome |
Surgical Landmarks
- Kocher maneuver: Mobilization of the duodenum and pancreatic head by incising the lateral peritoneum; exposes the IVC, right renal vein, and retropancreatic common bile duct
- Whipple procedure (pancreaticoduodenectomy): Removes the head, neck, uncinate process, duodenum, and distal bile duct; preservation of the SMA/SMV is the key resectability criterion
- Distal pancreatectomy: Removes body + tail, usually with splenectomy
Sources: Mulholland & Greenfield's Surgery 7e, pp. 2585–2587; Yamada's Textbook of Gastroenterology 7e, pp. 114–130; Guyton and Hall Textbook of Medical Physiology, p. 962; Bailey and Love's Short Practice of Surgery 28e, p. 1281.
This is a shared conversation. Sign in to Orris to start your own chat.