Fibroadenoma of breast
Reading File
Finding Sources
Searching PubMed
fibroadenoma breast
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
I now have comprehensive information to provide a thorough answer. Let me compile the complete response.
Fibroadenoma of the Breast
Definition & Overview
Fibroadenoma is the most common benign solid tumor of the female breast and the most frequent cause of a breast lump in women aged 15-25 years. It is a fibroepithelial tumor composed of benign proliferation of both glandular epithelial and stromal components arising from the terminal duct lobular unit (intralobular stroma).
Molecular Pathogenesis
-
MED12 mutations are the most common driver event (~two-thirds of cases). MED12 encodes a subunit of the mediator complex, which regulates RNA polymerase II-dependent transcription. Notably, uterine leiomyomas - another hormone-responsive stromal tumor - also strongly harbor MED12 mutations, suggesting a shared pathogenesis in hormonally driven stromal neoplasia.
-
Around one-third additionally harbor mutations in RARA (retinoic acid receptor alpha), an estrogen target gene that cooperates with ER in regulating transcription.
-
Hormonal responsiveness is central: tumors can grow during pregnancy and regress after menopause.
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 984
Epidemiology
| Feature | Detail |
|---|---|
| Peak age | 20-35 years (may occur in teenagers) |
| Multiplicity | Frequently multiple and bilateral |
| Regression | ~15% regress spontaneously |
| Postmenopausal | Rare; often calcified when found |
| Special population | ~50% of cyclosporin A recipients after renal transplant develop multiple bilateral fibroadenomas |
Gross & Microscopic Morphology
Gross appearance:
- Well-circumscribed, rubbery, gray-white nodule that bulges above surrounding tissue
- Usually 1-3 cm; occasionally very large ("giant fibroadenoma" >5 cm)
- Contains slit-like spaces lined by epithelium
- Sharply delineated from surrounding breast parenchyma (encapsulated)
Microscopic patterns:
- Pericanalicular pattern - delicate, often myxoid stroma surrounds patent (open) ducts
- Intracanalicular pattern - stroma compresses and distorts ductal elements into cleft-like spaces
In older women: stroma becomes densely hyalinized and epithelium becomes atrophic; calcifications may be present.
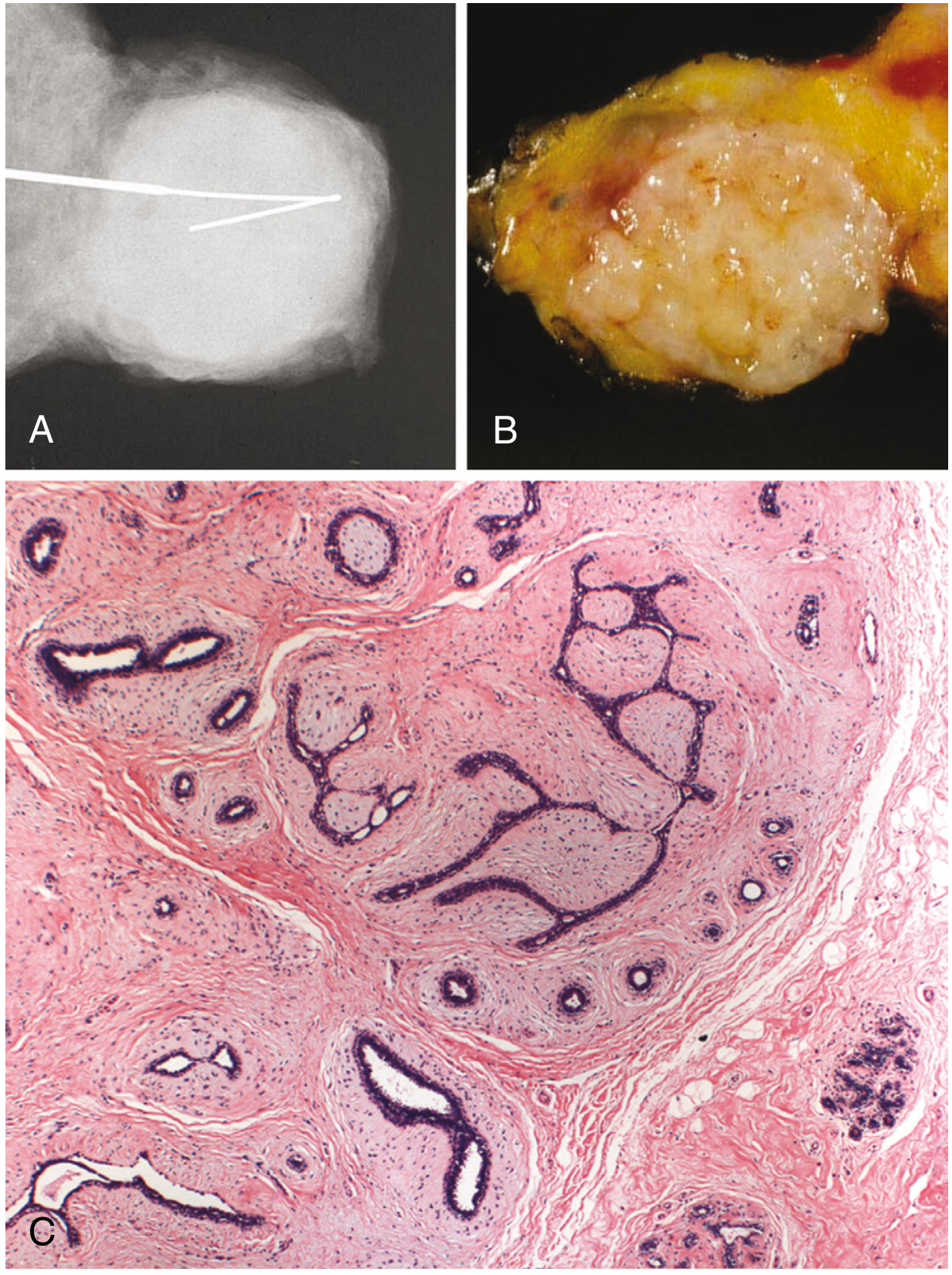
Here are the classic imaging and histologic appearances (Robbins, Fig. 23.24):
Subtypes
| Subtype | Features | Significance |
|---|---|---|
| Pericanalicular | Open patent ducts surrounded by stroma | Routine |
| Intracanalicular | Stroma compresses ducts into clefts | Routine |
| Myxoid | Myxoid stroma; may be sporadic or associated with Carney complex (PRKAR1A germline mutations, AD) | Consider genetic screening |
| Complex | Contains cysts >0.3 cm, sclerosing adenosis, epithelial calcifications, or papillary apocrine change | Slightly elevated breast cancer risk |
| Giant | >5 cm; occurs during puberty; rapidly growing | Requires surgical excision |
| Juvenile | Adolescent girls; may grow rapidly | Clinical surveillance needed |
Clinical Features
- Detected as a discrete, firm, smooth, rubbery, freely mobile mass - the classic "breast mouse"
- No skin dimpling, no nipple retraction, no inflammatory signs
- Often bilobed (groove palpable on examination)
- Young woman typically notices it while bathing or dressing
- May grow rapidly during pregnancy (including infarction, mimicking carcinoma)
- Regression post-menopause
Investigations
Imaging
- Ultrasound (modality of choice in young women): solid, uniformly hypoechoic, smoothly marginated, oval/round, wider than tall
- Mammography: well-circumscribed density; in older women - "popcorn" calcifications (dystrophic)
- Classic imaging appearance in women <25 may not require biopsy; a biopsy should be obtained if the patient is >25 years or there are atypical features
Histology / Biopsy
- Image-guided core needle biopsy is the standard for confirmation
- Triple assessment (clinical + imaging + pathology) is the principle
- Note: "cellular fibroepithelial lesion" on core biopsy cannot reliably distinguish fibroadenoma from phyllodes tumor - surgical excision required in that case
Risk of Malignancy
| Type | Relative Risk (RR) of Breast Cancer |
|---|---|
| Simple fibroadenoma | 1.5 - 1.7x |
| With epithelial hyperplasia | 3.4 - 3.7x |
| Complex fibroadenoma + family history | 3.0 - 4.0x (especially lobular carcinoma) |
| No family history, simple | No significantly increased risk (some sources say no increased risk) |
- Bailey and Love's Short Practice of Surgery 28th Edition, p. XX
The increased risk in complex fibroadenoma is partly because complex changes are often associated with adjacent "at-risk" lesions (e.g., atypical hyperplasia) in the surrounding breast tissue.
Management
Conservative (Observation)
The majority of fibroadenomas do not require surgical intervention. Conservative management with serial imaging is standard for:
- Typical clinical and imaging features
- Size <3 cm
- No rapid growth
- Patient age <25-30 years
- No atypia on biopsy
About 15% regress spontaneously; most are static at 2-3 cm.
Medical
- Tamoxifen and ormeloxifene (anti-estrogens) have shown some regression effects - not routinely used but documented (Bailey & Love)
Surgical Excision Indications
| Indication | Details |
|---|---|
| Age >30 years | Higher risk, lower spontaneous regression |
| Large size | >3 cm (Current Surgical Therapy) or >5 cm (Bailey & Love) |
| Rapid growth | >20% increase in 6 months |
| Suspicious imaging features | Microlobulation, irregular margins |
| Atypia on core biopsy | |
| Family history of breast cancer | |
| Symptomatic / patient preference | Anxiety, cosmetic concern |
| Elderly patients | Excise with a rim of normal tissue (may contain malignancy or phyllodes tumor) |
Giant fibroadenomas (>5 cm) can be enucleated through a submammary incision.
Minimally Invasive Options
- Percutaneous vacuum-assisted biopsy (ultrasound-guided)
- Percutaneous cryoablation - emerging option (a 2025 systematic review, PMID 41061430 confirmed it is safe and effective for management of benign fibroadenomas)
Fibroadenoma vs. Phyllodes Tumor (Key Differential)
| Feature | Fibroadenoma | Phyllodes Tumor |
|---|---|---|
| Age | 20-35 years | 30s-50s |
| Size | Usually 1-3 cm | Often larger |
| Growth | Slow | Can be rapid |
| Stroma | Delicate, myxoid | Cellular, mitotically active |
| Bilaterality | Common | Rare |
| MED12/RARA mutations | Yes | Yes (+ TERT, TP53, RB in malignant) |
| Management | Observe or excise | All types require excision with clear margins |
A core biopsy reporting "cellular fibroepithelial lesion" must be excised surgically to distinguish the two.

Recent Evidence (2025-2026)
- Cryoablation for fibroadenoma: A 2025 systematic review (PMID 41061430) confirms it is safe and effective as a minimally invasive alternative to surgery.
- Multiple fibroadenomas: A 2026 systematic review (PMID 41919577) characterizes clinical features and management strategies specifically for multiple fibroadenomas - noting they are relatively common but management data have been scarce.
Summary
Fibroadenoma is a benign fibroepithelial neoplasm driven primarily by MED12 mutations in hormonally responsive stromal cells. It presents as a mobile, rubbery, painless breast lump in young women and is managed conservatively unless it is large, growing rapidly, histologically atypical, or the patient is older. The complex subtype carries slightly elevated cancer risk, but simple fibroadenoma in an otherwise low-risk woman requires no more than surveillance. Cryoablation is an emerging minimally invasive option for women seeking treatment without open surgery.
- Robbins, Cotran & Kumar Pathologic Basis of Disease
- Bailey and Love's Short Practice of Surgery, 28th Ed.
- Current Surgical Therapy, 14th Ed.
- Berek & Novak's Gynecology
This is a shared conversation. Sign in to Orris to start your own chat.