Hernia
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
I now have all the content and images needed for a complete overview. Here is the comprehensive answer:
Hernia - Overview: Types, Anatomy & Pathophysiology
A hernia is the protrusion of a viscus (or part of a viscus) through a defect in the wall of the cavity that normally contains it. Hernias may be congenital (present from birth due to a developmental failure) or acquired (from aging, muscle weakening, increased intraabdominal pressure, or previous surgery).
Classification
Hernias are broadly classified as:
| Category | Examples |
|---|---|
| External abdominal wall | Inguinal (direct & indirect), femoral, umbilical, epigastric, spigelian, incisional |
| Internal | Paraduodenal, foramen of Winslow, iatrogenic (post-bariatric surgery mesenteric defects) |
| Special variants | Richter hernia, pantaloon hernia, Littre hernia |
- Maingot's Abdominal Operations classifies hernia as: external abdominal wall (congenital or acquired), internal, and incisional.
Groin Hernias
1. Indirect Inguinal Hernia (most common overall)
- The hernia sac passes through the internal (deep) inguinal ring and travels along the inguinal canal, potentially reaching the scrotum.
- Located lateral to the inferior epigastric vessels.
- The developmental basis is a patent processus vaginalis - failure of this structure to close after testicular descent.
- More common in males; affects ~5% of full-term infants and up to 30% of preterm infants.
- 30% of hernias in children younger than 3 months become incarcerated - referral for elective repair is important even if asymptomatic.
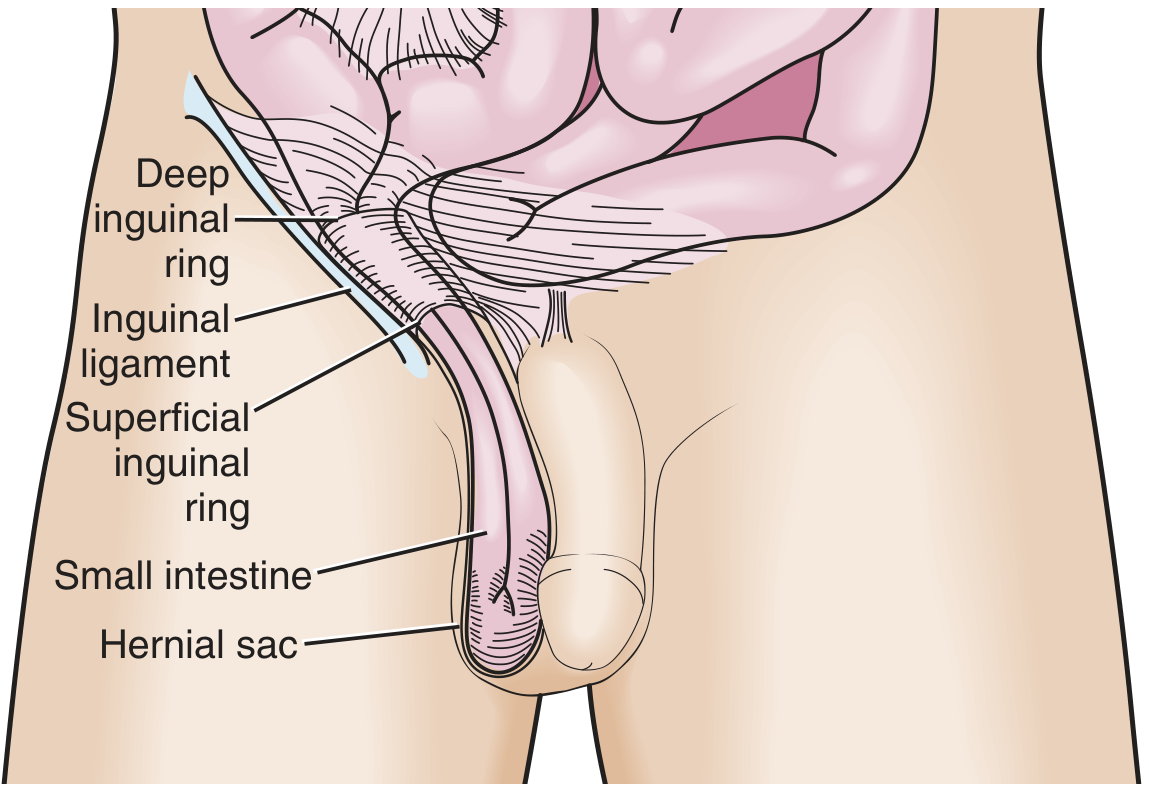
Indirect inguinal hernia - Roberts and Hedges' Clinical Procedures in Emergency
2. Direct Inguinal Hernia
- Protrudes directly through the muscular and fascial wall of the abdomen (Hesselbach's/inguinal triangle), medial to the inferior epigastric vessels.
- Does not travel along the inguinal canal.
- An acquired condition caused by progressive weakening of the myofascial wall due to aging and repetitive stress from raised intraabdominal pressure.
- Carries a lower risk of incarceration because the hernia orifice is typically wide.
- Second most common groin hernia.
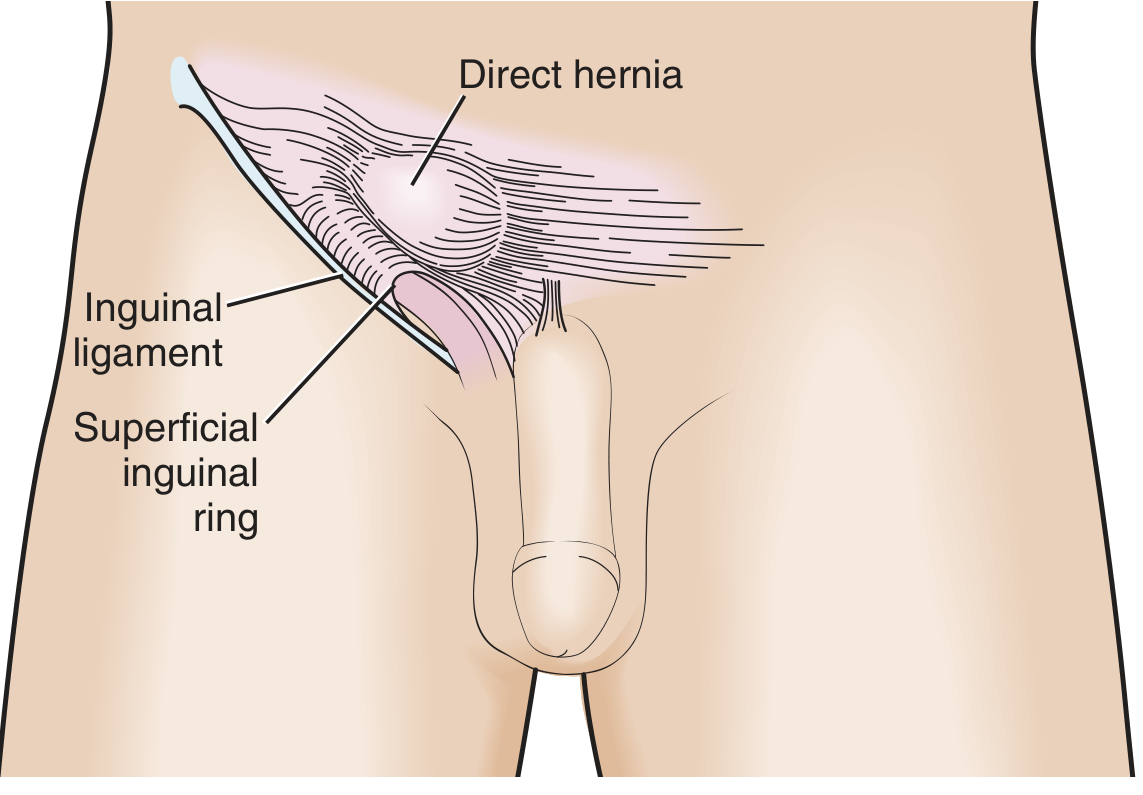
Direct inguinal hernia - Roberts and Hedges' Clinical Procedures in Emergency
Distinguishing direct from indirect on examination:
- Indirect starts lateral to the inferior epigastric vessels; direct is medial.
- Indirect hernia contents strike the tip of an examining finger (travels down the canal); direct hernia bulges against the pad of the finger.
- Pressure over the internal ring after reduction prevents recurrence of an indirect hernia during Valsalva, but not a direct hernia.
- A hernia filling the scrotum is almost always indirect.
3. Pantaloon Hernia
A combined direct + indirect hernia occurring simultaneously. It is difficult to diagnose in the ED, difficult to reduce, and is often discovered during surgical exploration. - Roberts and Hedges'
4. Femoral Hernia
- Occurs inferior to the inguinal ligament through a defect in the transversalis fascia.
- Contents enter the femoral canal (medial to femoral vein, lateral to the lacunar ligament), presenting as a medial thigh mass below the inguinal ligament.
- More common in women.
- The small fascial defect creates a very high incarceration risk - up to 45% are incarcerated at presentation.
- Up to 40% are strangulated at first presentation (far higher than inguinal or incisional hernias).
Ventral (Abdominal Wall) Hernias
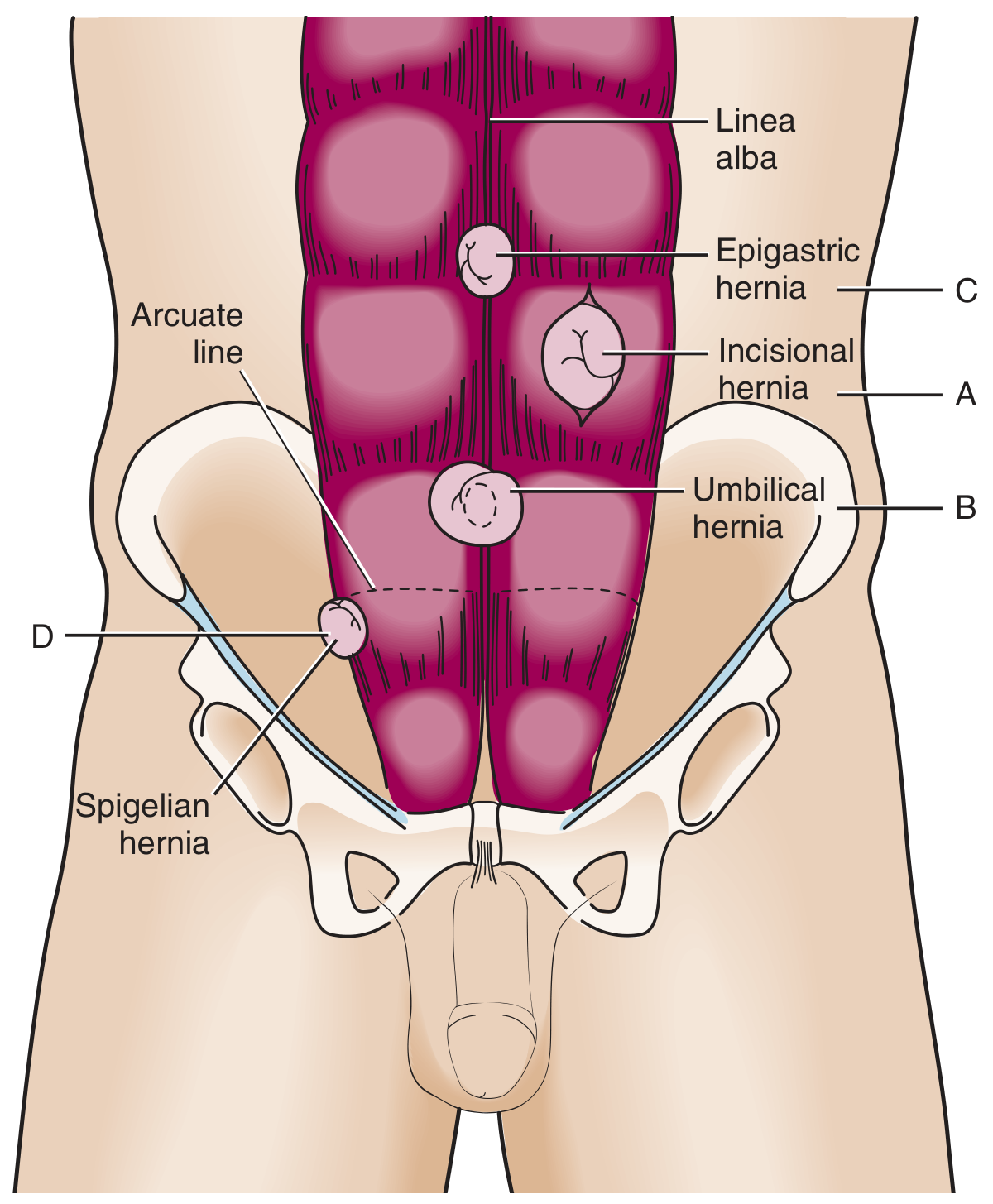
Ventral hernias - Roberts and Hedges' Clinical Procedures in Emergency
5. Umbilical Hernia
- Traverses the fibromuscular ring of the umbilicus.
- Most common in infants and children (congenital); often resolves spontaneously by age 5. Repair is indicated if it persists beyond 5 years, is larger than 2 cm, or becomes incarcerated.
- In adults, acquired umbilical hernias arise from increased intraabdominal pressure (obesity, ascites, pregnancy).
- Umbilical hernias account for ~15% of emergency hernia surgery, with up to 60% showing strangulation at the time of surgery.
6. Incisional Hernia
- Occurs in up to 1 in 5 patients following abdominal surgery.
- Risk is increased by poor wound healing (e.g., wound infection).
- Recurrence rates of 20-50% after repair.
- Incarceration risk is inversely related to defect size - larger defects have lower incarceration risk.
7. Epigastric Hernia
- Occurs in the midline through the linea alba, typically between the xiphoid and umbilicus.
- Usually small; in adults, contains preperitoneal fat rather than bowel.
- Found in ~4% of pediatric patients evaluated for hernias.
8. Spigelian Hernia
- Rare. Protrudes through a defect at the lateral edge of the rectus muscle at the semilunar line near the arcuate line (through the spigelian fascia).
- Typically affects patients aged 40-70.
- Incarceration rate (often with omentum) reported as high as 20%.
- Ultrasound may be a useful adjunct for diagnosis.
Internal Hernias
- Herniation of bowel at an opening in the peritoneum, mesentery, or omentum.
- Congenital types: mostly paraduodenal or through the foramen of Winslow (posterior to the porta hepatis).
- The most common type today is iatrogenic - resulting from operations dividing the mesentery (Roux-en-Y gastric bypass, colectomy, pancreaticoduodenectomy).
- Also include: obturator canal hernias and sciatic notch hernias.
- Internal hernias are sometimes diagnosed on CT but often found at laparotomy for presumed adhesive small bowel obstruction (SBO). - Sleisenger & Fordtran's Gastrointestinal and Liver Disease
Pathophysiology: Key States
| State | Definition | Risk |
|---|---|---|
| Reducible | Contents return spontaneously or manually to normal position | Low immediate risk |
| Incarcerated | Contents cannot be reduced; but vascular supply may still be intact | Moderate - not automatically an emergency |
| Strangulated | Any ischemia/obstruction from compression within the hernia neck | Surgical emergency - may progress to bowel necrosis |
| Richter hernia | Only a portion of the bowel wall is incarcerated - obstruction may be incomplete or absent, masking severity | High missed diagnosis risk |
Strangulation risk is inversely proportional to hernia size - smaller hernias are more dangerous (femoral > indirect inguinal > incisional). Among patients requiring surgery for SBO due to incarcerated hernia, intestinal ischemia occurs in up to 75% and intestinal necrosis in more than 25%. - Sleisenger & Fordtran's
Epidemiology & Predisposing Factors
- Hernias of all types are the second most common cause of bowel obstruction in Western countries, after adhesions.
- Factors raising intraabdominal pressure that predispose to acquired hernias include: chronic cough, chronic constipation, straining to urinate (e.g., BPH), obesity, ascites, and pregnancy.
- Congenital hernias are related to developmental failures (patent processus vaginalis for inguinal; umbilical ring closure failure for umbilical hernias).
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine; Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Mulholland and Greenfield's Surgery - Scientific Principles and Practice 7e; Maingot's Abdominal Operations.
This is a shared conversation. Sign in to Orris to start your own chat.