What is Murmurs? How Vitamin Deficiency Linked With It?
Reading File
Finding Sources
Finding Sources
Searching PubMed
heart murmur vitamin deficiency
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Searching the Web
vitamin deficiency heart murmur connection clinical evidence 2024 2025
I now have all the information needed to write a comprehensive, well-cited response. Here it is:
Heart Murmurs: What They Are and How Vitamin Deficiencies Are Linked
What Is a Heart Murmur?
A heart murmur is an audible sound produced by turbulent blood flow within or near the heart, heard between the normal "lub-dub" heart sounds (S1 and S2) during auscultation. The underlying mechanisms include:
- Accelerated blood flow through a normal or abnormal orifice
- Flow through a narrowed or irregular orifice into a dilated vessel or chamber (e.g., valvular stenosis)
- Backward (regurgitant) flow through an incompetent valve, ventricular septal defect (VSD), or patent ductus arteriosus (PDA)
"Heart murmurs are caused by audible vibrations that are due to increased turbulence from accelerated blood flow through normal or abnormal orifices; flow through a narrowed or irregular orifice into a dilated vessel or chamber; or backward flow through an incompetent valve, ventricular septal defect, or patent ductus arteriosus."
- Harrison's Principles of Internal Medicine 22E, Ch. 44
Classification of Heart Murmurs
Murmurs are classified by their timing in the cardiac cycle:
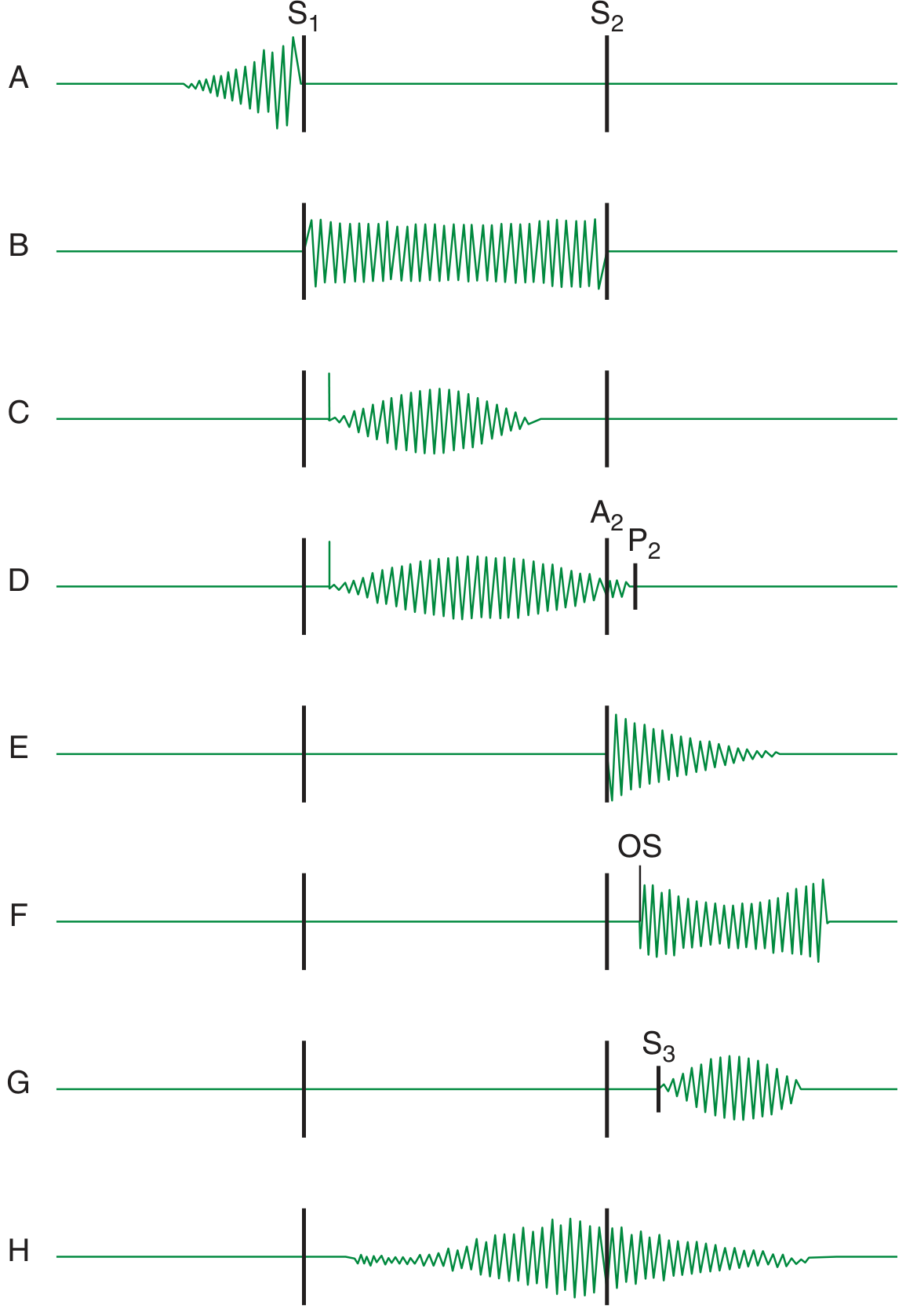
1. Systolic Murmurs
Begin with or after S1, end at or before S2.
| Type | Description | Causes |
|---|---|---|
| Midsystolic (ejection) | Crescendo-decrescendo, peaks in mid-systole | Aortic stenosis, pulmonic stenosis, flow murmur |
| Holosystolic (pansystolic) | Constant intensity throughout systole | Mitral regurgitation, tricuspid regurgitation, VSD |
| Late systolic | Starts after ejection, peaks late | Mitral valve prolapse |
2. Diastolic Murmurs
Begin with or after S2, end before the next S1.
| Type | Description | Causes |
|---|---|---|
| Early diastolic | High-pitched, blowing, decrescendo | Aortic regurgitation, pulmonic regurgitation |
| Mid-diastolic | Low-frequency rumble | Mitral stenosis, tricuspid stenosis |
| Presystolic | Just before S1, in patients with sinus rhythm | Mitral/tricuspid stenosis |
3. Continuous Murmurs
Span both systole and diastole without interruption.
- Classic cause: Patent Ductus Arteriosus (PDA) - the "machinery murmur"
- Also: A-V fistula, ruptured sinus of Valsalva
Grading (Levine Scale I-VI)
- I/VI: Barely audible
- II/VI: Faint but immediately heard
- III/VI: Moderate intensity, no thrill
- IV/VI: Loud with palpable thrill
- V/VI: Very loud, heard with stethoscope partially off chest
- VI/VI: Heard without stethoscope
Innocent vs. Pathological Murmurs
The majority of murmurs in asymptomatic children and young adults are midsystolic, soft (grade I-II/VI), and benign - requiring no further workup if there is no other evidence of heart disease. Echocardiography is indicated for:
- Loud systolic murmurs (grade ≥III/VI), especially holosystolic or late systolic
- Most diastolic or continuous murmurs (Harrison's, Ch. 243)
How Vitamin (and Nutritional) Deficiencies Are Linked to Murmurs
The link between vitamins/nutritional deficiencies and murmurs operates through multiple pathways:
1. Thiamine (Vitamin B1) Deficiency - Beriberi Heart Disease
This is the most direct vitamin-murmur connection.
Mechanism: Thiamine is essential for cellular energy metabolism. Deficiency causes tissues to fail to properly extract nutrients from blood, triggering compensatory peripheral vasodilation. Total peripheral resistance can fall to as little as half of normal. The heart responds with a marked increase in cardiac output (sometimes double the normal value).
Result: High-output heart failure with:
- Hyperdynamic circulation
- Tachycardia
- Dilated cardiomyopathy
- Flow murmurs from elevated cardiac output (turbulence across valves)
- If untreated, progresses to low-output heart failure
"This disease is initially a vasodilated state with very-high-output heart failure that can later progress to a low-output state; thiamine repletion can lead to prompt recovery of cardiovascular function."
- Harrison's Principles of Internal Medicine 22E, Ch. 269
At-risk groups: Malnourished populations, alcoholics, patients deriving most calories from processed foods or alcohol.
(Goldman-Cecil Medicine; Guyton & Hall Medical Physiology)
2. Iron Deficiency (Anemia)
Mechanism: Iron deficiency anemia causes two effects:
- Reduced blood viscosity (fewer red cells)
- Tissue hypoxia triggers local vasodilation
Both decrease total peripheral resistance, raising cardiac output. Severe anemia produces a characteristic high-pitched systolic flow murmur across the pulmonary or aortic valve due to turbulent, low-viscosity, fast-moving blood.
"Iron-deficiency anemia can cause pale skin and, in severe cases, a rapid heartbeat or heart murmur." - JAMA Network, 2024
This is the most commonly encountered vitamin/nutritional murmur in clinical practice, especially in children and pregnant women.
3. Calcium Deficiency
Mechanism: Calcium is essential for excitation-contraction coupling in cardiac myocytes. Chronic calcium deficiency (from hypoparathyroidism, GI malabsorption, or post-bariatric surgery) directly impairs myocardial contractility, leading to dilated cardiomyopathy and heart failure. Compensatory hemodynamic changes in this context can produce murmurs.
"Calcium is essential for excitation-contraction coupling. Chronic deficiencies of calcium, such as can occur with hypoparathyroidism or intestinal dysfunction, can cause severe chronic heart failure."
- Harrison's, Ch. 269
4. Phosphate and Magnesium Deficiency
- Hypophosphatemia (alcoholism, refeeding syndrome, hyperalimentation) reduces myocardial contractility
- Magnesium depletion may present with left ventricular dysfunction
- Both can contribute indirectly to hemodynamic changes that produce flow murmurs (Goldman-Cecil Medicine)
5. Selenium Deficiency - Keshan's Disease
Selenium deficiency causes Keshan's disease - a dilated cardiomyopathy seen in selenium-poor geographic regions (e.g., parts of China). The resulting dilated ventricle causes mitral regurgitation, producing a holosystolic murmur.
(Harrison's, Ch. 269)
6. Vitamin D Deficiency - Emerging Evidence
Mechanism: Vitamin D receptors are present in cardiac muscle and vascular smooth muscle. Deficiency is associated with:
- Increased risk of hypertension (leading to aortic and mitral valve stress)
- Left ventricular hypertrophy
- Impaired myocardial contractility
- A 2025 AHA study showed adults with heart disease who optimized Vitamin D levels reduced their risk of heart attack by 52%
A 2025 case report in PMC also documented resolution of complete heart block after Vitamin D supplementation, suggesting an electrophysiological role.
While vitamin D deficiency does not directly cause a murmur in isolation, it contributes to structural cardiac changes that can lead to valvular dysfunction over time.
7. B Vitamins (B12, Folate) - Indirect Link
- Vitamin B12/Folate deficiency causes megaloblastic anemia, which - like iron deficiency anemia - produces high-output circulation and flow murmurs
- Additionally, B12 deficiency raises homocysteine levels, which damages the vascular endothelium and may accelerate valve calcification
Summary Table
| Deficiency | Mechanism | Cardiac/Murmur Effect |
|---|---|---|
| Thiamine (B1) | Peripheral vasodilation, high cardiac output | High-output failure, flow murmurs, dilated cardiomyopathy |
| Iron | Anemia - low viscosity, high output | Systolic flow murmur (functional) |
| Calcium | Impaired excitation-contraction coupling | Dilated cardiomyopathy, secondary murmurs |
| Selenium | Keshan's disease (DCM) | Mitral regurgitation murmur |
| Phosphate/Magnesium | Reduced myocardial contractility | Secondary LV dysfunction, flow murmurs |
| Vitamin D | LVH, impaired myocardial function | Indirect structural valve changes |
| B12/Folate | Megaloblastic anemia + endothelial injury | Flow murmurs, accelerated valve calcification |
Key Clinical Takeaway
Most vitamin/nutritional deficiency murmurs are functional (flow) murmurs - they arise from increased cardiac output compensating for the metabolic deficit, NOT from primary valve disease. They typically resolve with treatment of the underlying deficiency. However, in the case of selenium deficiency (Keshan's) and calcium deficiency cardiomyopathy, structural cardiac damage can become permanent if the deficiency is prolonged and severe.
Sources:
- Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill)
- Goldman-Cecil Medicine, International Edition
- Guyton and Hall Textbook of Medical Physiology
- Tintinalli's Emergency Medicine
- American Heart Association Scientific Sessions 2025 (Vitamin D and heart attack risk)
This is a shared conversation. Sign in to Orris to start your own chat.