Gynecology examination according to bereks and Novak. Book
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of the Gynecologic Examination as presented in Berek & Novak's Gynecology (Chapter 1: Initial Assessment and Communication).
Gynecologic Examination — Berek & Novak's Gynecology
Overview
A thorough gynecologic physical examination is performed at the initial visit, periodically, and as needed throughout the course of treatment. The scope of the examination is dictated by the patient's primary concerns and symptoms. For healthy adolescents without symptoms requesting contraception before sexual activity, a pelvic exam is not necessarily required.
The ACOG continues to recommend an annual visit as an opportunity for shared decision-making about whether a pelvic examination is appropriate.
1. History
The history precedes any physical examination and includes:
- Chief complaint and present illness (using the structured technique in Table 1-5)
- Complete medical and surgical history
- Reproductive history (menstrual and obstetric)
- Current medications (including OTC and complementary/alternative)
- Family and social history
2. Physical Examination
A. General Examination
A complete physical examination includes assessment of vital signs, height, weight, and BMI. Body habitus, signs of endocrine or metabolic disease, skin changes, hair distribution, and breast examination are all components.
B. Abdominal Examination
The abdomen is inspected, auscultated, and palpated for:
- Organomegaly, masses, ascites
- Tenderness (direct and rebound)
- Surgical scars and hernias
3. Pelvic Examination
A. External Genitalia (Vulvar Inspection)
The patient is placed in the dorsal lithotomy position. The vulva, perineum, and perianal area are inspected systematically:
- Mons pubis, labia majora and minora, clitoris, urethral meatus, introitus
- Look for lesions, ulcers, condylomata, erythema, discharge, or atrophic changes
- The urethra and Skene glands are palpated; the Bartholin glands are evaluated for enlargement or tenderness
B. Urethral and Bartholin Gland Assessment
- Skene (paraurethral) glands are palpated for tenderness or discharge
- Bartholin glands (posterolateral walls of the introitus) are assessed for cysts or abscesses
C. Vagina and Cervix — Speculum Examination
A bivalve speculum (Graves or Pederson) is inserted to visualize:
| Structure | What to Assess |
|---|---|
| Vaginal walls | Color, discharge, lesions, rugae, atrophy |
| Cervix | Color, position, os (size/shape), discharge, lesions, ectropion |
| Fornices | Masses, tenderness |
Procedures performed at this stage:
- Cervical cytology (Pap smear) — technique and frequency per Chapter 16
- Cultures — for any purulent discharge from vagina or cervix (STI screening is routine in adolescents and young adults per CDC guidelines)
- Biopsy — for any visible lesions on the cervix or vaginal walls
- Endometrial biopsy — performed with a flexible cannula when indicated
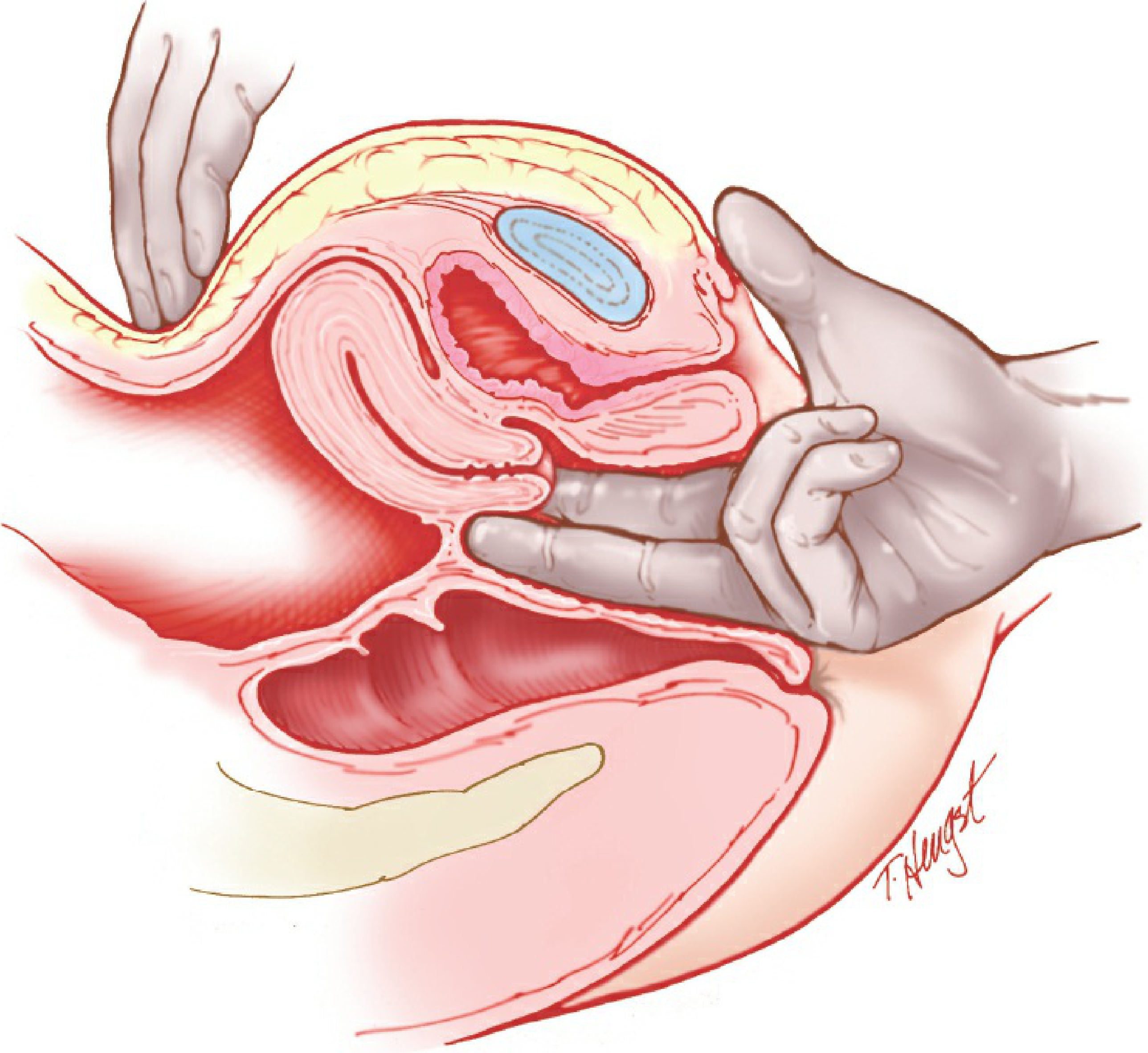
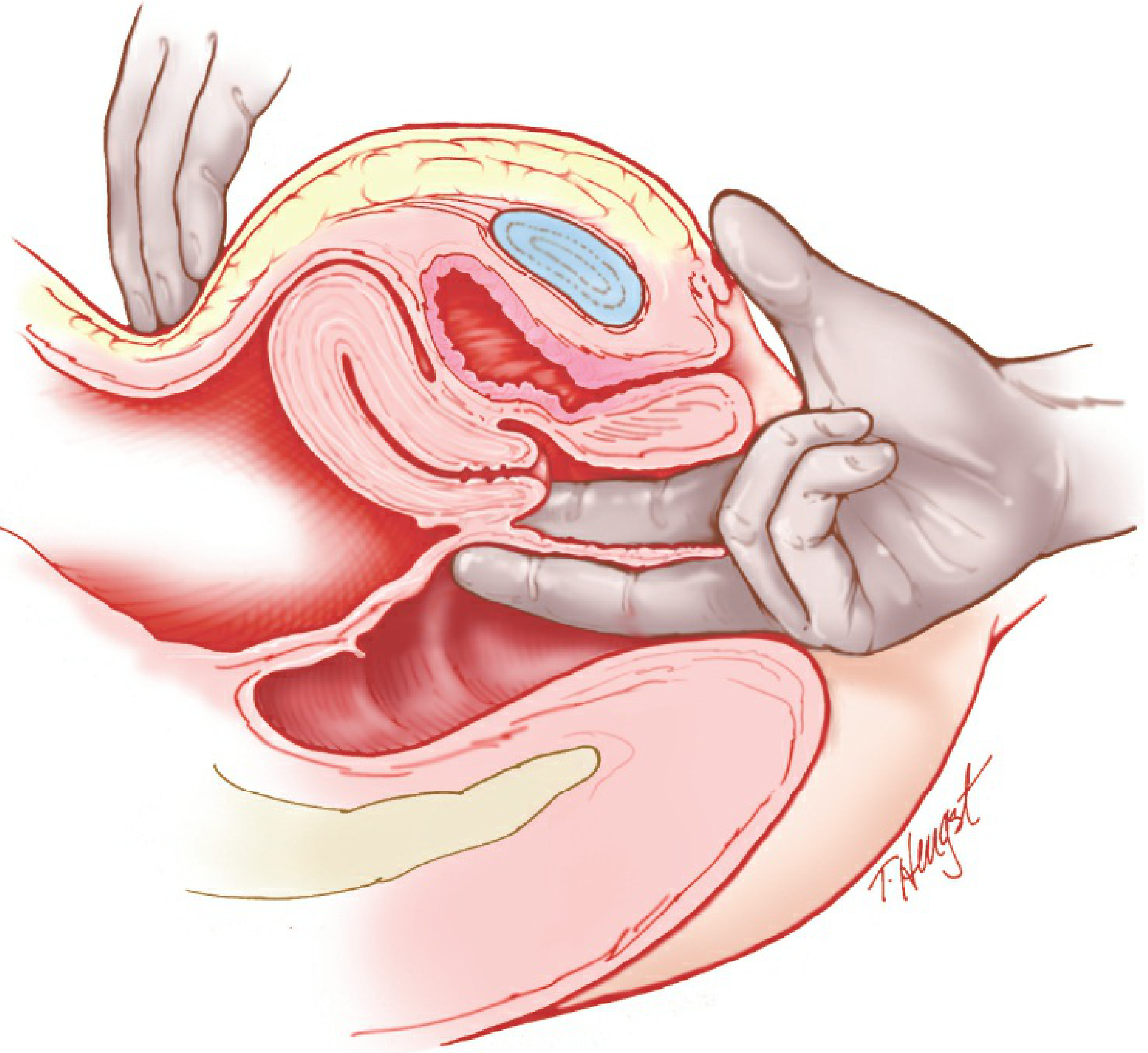
D. Bimanual Palpation
After removing the speculum, a lubricated gloved hand is used:
- One or two fingers (index ± middle) inserted into the vagina
- The opposite hand placed on the lower abdomen to provide counter-pressure
Uterus assessment:
- Size, shape, contour, consistency, position, and mobility
- Presence of tenderness (patient provides verbal feedback; facial expressions are observed)
Adnexal assessment:
- Both adnexa palpated gently
- Note any enlargement, mass, tenderness, or irregularity
- Document size, shape, mobility, and consistency
For patients with pelvic pain, a structured "functional pelvic examination" is performed — sequential palpation of:
- Vaginal introitus
- Pelvic floor muscles (spasm is a common concomitant of pelvic pain)
- Bladder
- Rectum
- Cervix
- Cul-de-sac
E. Rectovaginal Examination
Performed when indicated — one finger in the vagina, one in the rectum:
Structures assessed:
- Rectovaginal septum
- Posterior uterine surface
- Uterosacral ligaments → nodularity suggests endometriosis
- Posterior cul-de-sac → implants of ovarian cancer
- Adnexal structures (palpable from behind)
- Rectum: hemorrhoids, fissures, sphincter tone, polyps, carcinoma
A single stool fecal occult blood test obtained during rectal exam is not adequate for colorectal cancer screening and is not recommended.
4. Special Populations
Pediatric Patients
- The approach is modified based on age, symptoms, and the indication for examination
- A chaperone/parent is present
- Non-invasive techniques are preferred; vaginoscopy may be used under anesthesia when necessary
Adolescent Patients
- Pelvic examination is not required before prescribing contraception in asymptomatic adolescents
- STI screening is performed per CDC recommendations
- Confidentiality should be addressed
5. After the Examination
At the completion of the examination, the patient should be informed of findings:
- Normal results → reassure the patient
- Possible abnormality → discuss with the patient clothed after the examination, in clear understandable language
- Outline a plan for evaluation, explain proposed procedures (e.g., biopsy), and inform the patient when results will be available
Key Points Summary
| Component | Key Action |
|---|---|
| External genitalia | Systematic vulvar inspection (labia, clitoris, urethra, introitus) |
| Speculum exam | Visualize vaginal walls, cervix; collect Pap, cultures, biopsy as needed |
| Bimanual exam | Assess uterine size/position/mobility; palpate adnexa bilaterally |
| Rectovaginal exam | Evaluate uterosacral ligaments, posterior uterus, cul-de-sac; indicated for suspected endometriosis or malignancy |
| Communication | Inform patient of findings at conclusion; discuss abnormalities with patient clothed |
— Berek & Novak's Gynecology, Chapter 1: Initial Assessment and Communication
This is a shared conversation. Sign in to Orris to start your own chat.