Erbs palsy
Reading File
Finding Sources
Searching PubMed
"Erb palsy" OR "Erb's palsy" brachial plexus neonatal
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is a thorough overview of Erb's Palsy:
Erb's Palsy (Erb-Duchenne Palsy)
Definition
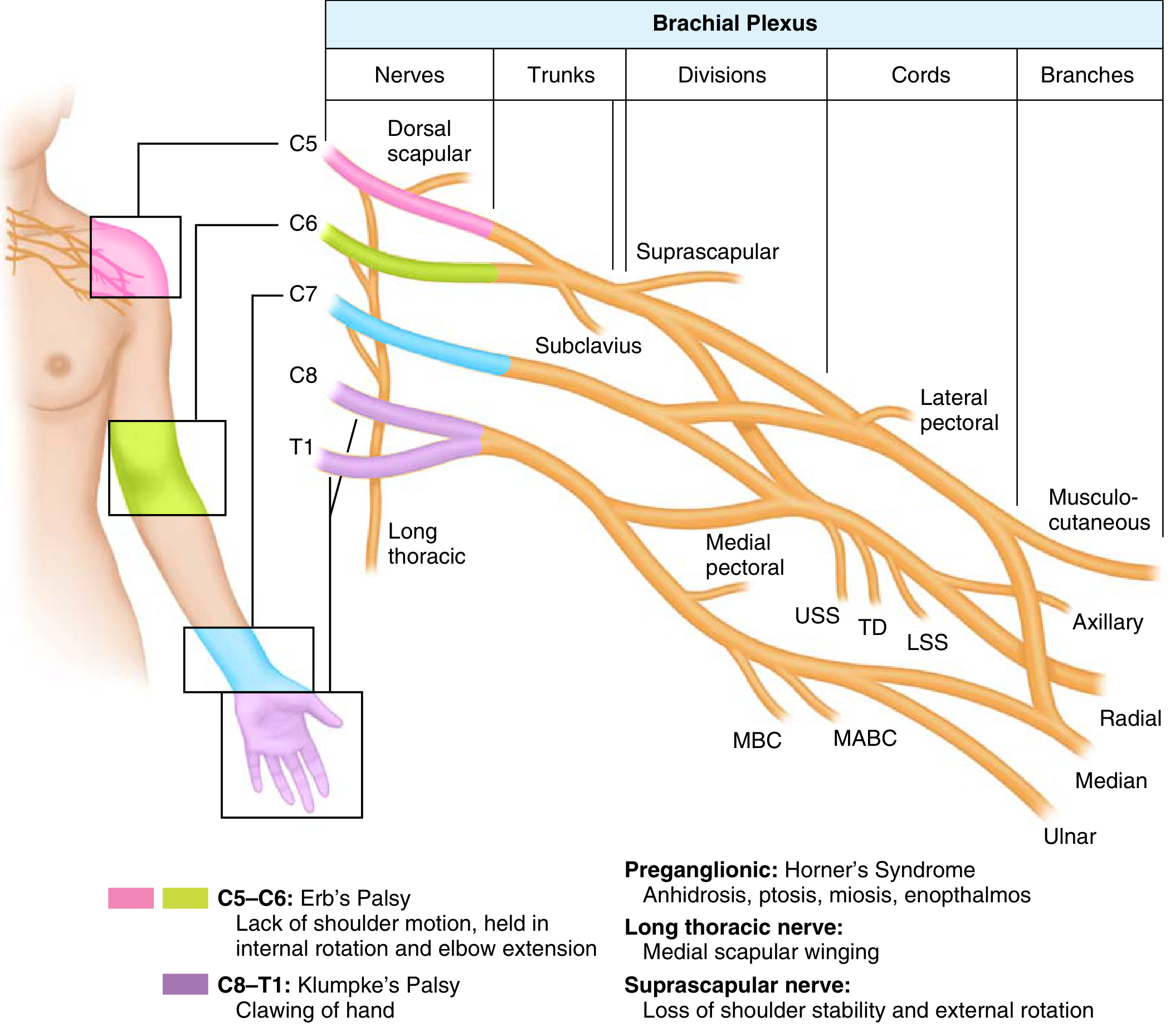
Erb's palsy is paralysis of the upper arm caused by injury to the upper trunk of the brachial plexus — C5 and C6 nerve roots (and sometimes C7). It is the most common form of brachial plexus injury and carries the best prognosis among the three recognized types.
Three Types of Brachial Plexus Birth Palsy
| Type | Roots | Prognosis | Features |
|---|---|---|---|
| Erb-Duchenne | C5, C6 | Best | Waiter's tip deformity; most common |
| Klumpke | C8, T1 | Poor | Claw hand; associated with Horner syndrome |
| Total plexus palsy | C5–T1 | Worst | Complete arm paralysis |
Epidemiology & Causes
- Occurs in approximately 2 per 1,000 births
- Obstetric (neonatal) — the most common setting:
- Shoulder dystocia in large-for-gestational-age infants
- Forceps or assisted delivery
- Breech position
- Prolonged labor
- Cephalopelvic disproportion
- Adult/traumatic:
- Glenohumeral joint dislocation (most common adult mechanism)
- Motorcycle accidents with traction/avulsion
- Falls where arm is outstretched
- Iatrogenic (improper arm positioning under anesthesia)
- Apical (Pancoast) lung tumor compressing the plexus
- Burners/stingers in athletes (compression of plexus between shoulder pad and superior medial scapula at the Erb point, superior to the clavicle)
Clinical Features
Characteristic posture — "Waiter's tip" / "Bellhop's tip":
- Arm hangs at the side, internally rotated
- Elbow extended (loss of elbow flexion)
- Forearm pronated
- Wrist and finger extension also lost (if C7 involved)
- Hand movements are preserved (intrinsic muscles intact)
Reflexes & signs:
- Absent or diminished biceps reflex on the affected side
- Asymmetric Moro reflex in neonates
- If C7 is involved: loss of wrist and finger extension
Associated injuries (neonatal):
- Diaphragmatic paralysis (phrenic nerve, C3–C5)
- Horner syndrome (sympathetic chain involvement — suggests preganglionic/avulsion)
- Fractured clavicle or humerus
- Facial palsy
- Progressive glenoid hypoplasia in 70% of children with significant internal rotation contracture
Investigations
- Clinical examination is the primary basis for diagnosis
- EMG/NCS (performed ≥4–6 weeks after injury for Wallerian degeneration):
- Evaluates extent of denervation and monitors recovery
- Fibrillation potentials = active denervation
- Normal SNAPs with sensory loss = preganglionic injury
- Paraspinal denervation on EMG = nerve root avulsion
- Imaging:
- CT myelography: detects nerve root avulsions (pseudomeningoceles)
- MRI: peripheral neuroma, pseudomeningoceles, mass lesions
- Plain X-ray (cervical spine, chest, shoulder): transverse process fractures suggest avulsion; elevated hemidiaphragm suggests phrenic nerve injury
- Axillary lateral X-ray: assesses humeral head position (posterior subluxation/glenoid erosion)
- Somatosensory evoked potentials: assess nerve root continuity
Prognosis
- Rate of initial improvement is the key prognostic factor
- Improved arm function within 2–4 weeks → full recovery expected
- Deficits persist in approximately 25% of patients
- Poor prognostic signs:
- Absence of biceps function at 6 months
- Presence of Horner syndrome
- No biceps/deltoid contraction within 3–6 months
- Complete recovery possible if biceps and deltoid are at least M1 (contraction without movement) by 2 months
- Muscle fibrosis sets in after 18–24 months — a critical window
Treatment
Conservative (First-line)
- Physical and occupational therapy at a specialized multidisciplinary centre by 1 month of age
- Passive range-of-motion (ROM) exercises: focus on shoulder elevation, abduction, external rotation, and elbow motion
- Goal: maintain passive ROM while awaiting return of motor function (up to 18 months)
- >90% of cases eventually resolve without surgical intervention
Surgical
Timing:
| Timing | Indication |
|---|---|
| Immediate | Penetrating trauma, iatrogenic injury, vascular injury, progressive deficits |
| 3–12 weeks | Incomplete/near-complete injuries from high-energy mechanism |
| 3–6 months | Incomplete upper plexus lesion from low-energy mechanism or recovery plateau |
| >3 months (neonatal) | No evidence of spontaneous recovery |
| >6 months | Nerve repair has less predictable outcome |
Nerve reconstruction options:
- Direct repair (limited by tension — usually requires grafting)
- Neuroma excision + nerve cable grafting (donor: sural, medial brachial cutaneous, medial antebrachial cutaneous nerves)
- Best outcomes: young patients treated within 3 months of injury
- Nerve transfers (when proximal axons insufficient, e.g., avulsions):
- Oberlin transfer: ulnar nerve fascicle → musculocutaneous nerve (restores elbow flexion)
- Spinal accessory nerve (CN XI) → suprascapular nerve (restores shoulder abduction)
- Triceps motor branch (radial) → axillary nerve (shoulder abduction/elevation — Leechavengvong procedure)
Priorities for reconstruction: Elbow flexion > Shoulder stabilization > Hand function
Late/deformity surgery:
- Tendon/muscle transfers if no meaningful recovery after 6–12 months
- Addressing internal rotation contracture and posterior glenoid subluxation
Key Mnemonics
- "REEDA" roots: C5, C6 (upper trunk) → Erb's palsy
- "Waiter's tip" posture: arm adducted, internally rotated, elbow extended, forearm pronated
- Most reliable sign of nerve recovery: advancing Tinel sign
Sources: Bradley and Daroff's Neurology in Clinical Practice; Miller's Review of Orthopaedics 9th Ed.; Schwartz's Principles of Surgery 11th Ed.; Color Atlas of Human Anatomy; Creasy & Resnik's Maternal-Fetal Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.