Audiometry
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Now I have comprehensive material. Here is a complete guide to interpreting audiograms.
Audiogram Interpretation
The Audiogram — Basic Layout
The audiogram plots frequency (Hz) on the horizontal axis (low pitch on the left → high pitch on the right: 125 to 8000 Hz) against hearing threshold level (dB HL) on the vertical axis — but crucially, worse hearing is downward (0 dB HL at top = normal; 120 dB HL at bottom = profound loss).
Step 1 — Assess Severity
Thresholds are classified per the ANSI standard:
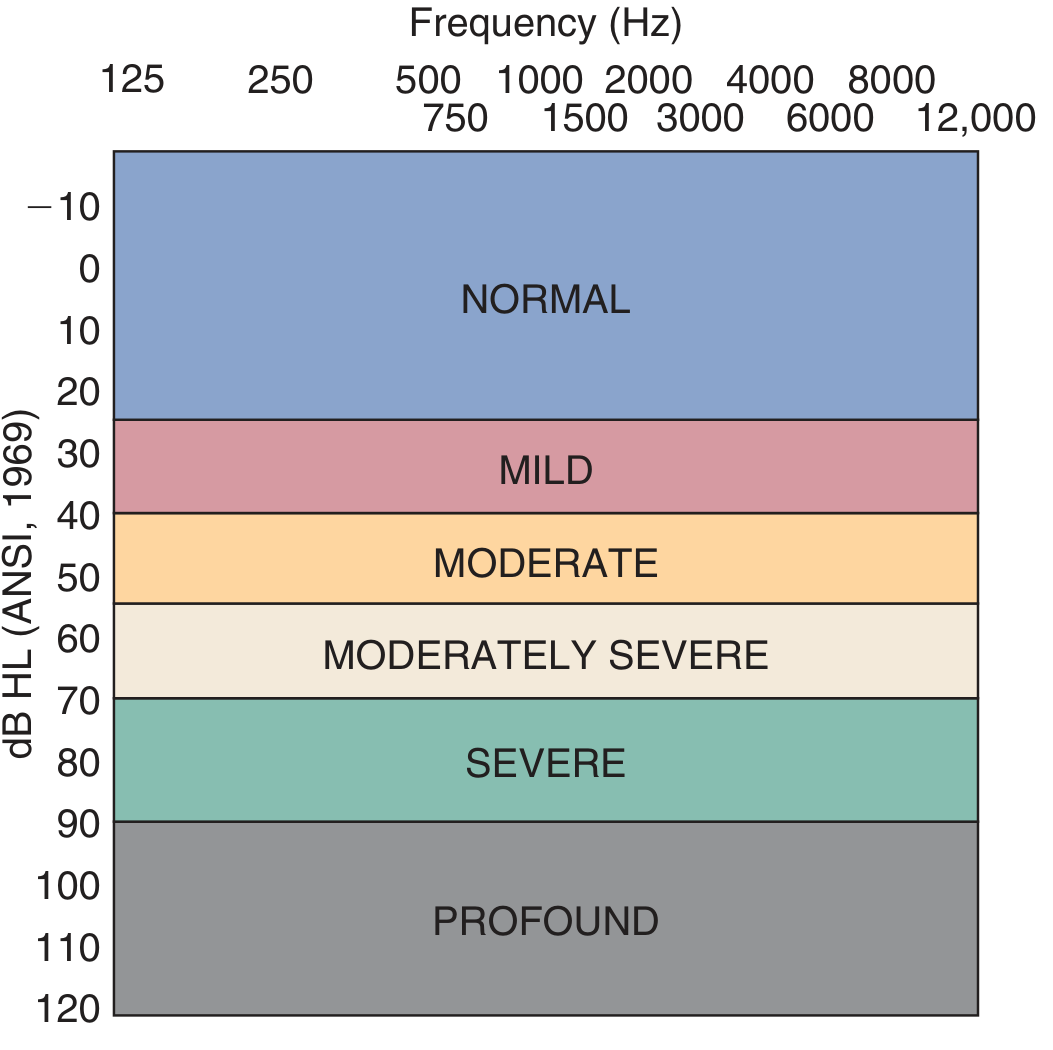
| Threshold (dB HL) | Grade |
|---|---|
| −10 to 25 | Normal |
| 26–40 | Mild |
| 41–55 | Moderate |
| 56–70 | Moderately severe |
| 71–90 | Severe |
| > 90 | Profound |
The pure-tone average (PTA) summarises severity: average of thresholds at 500, 1000, and 2000 Hz.
Step 2 — Read the Symbols
| Symbol | Meaning |
|---|---|
| O (circle, right) | Right ear, air conduction (unmasked) |
| X (cross, left) | Left ear, air conduction (unmasked) |
| △ (triangle) | Air conduction, masked |
| [ ] (bracket pointing right) | Right ear, bone conduction (unmasked) |
| ] [ (bracket pointing left) | Left ear, bone conduction (unmasked) |
| < > (angle brackets) | Bone conduction, masked |
Step 3 — Determine Type of Loss
Air-Bone Gap (ABG)
The key concept:
- Air conduction (AC) tests the entire auditory pathway (outer ear → middle ear → cochlea → auditory nerve → brain)
- Bone conduction (BC) bypasses the outer and middle ears and stimulates the cochlea directly
ABG = AC threshold − BC threshold at a given frequency. An ABG > 10 dB is significant.
Conductive Hearing Loss
BC is normal; AC is elevated → air-bone gap is present
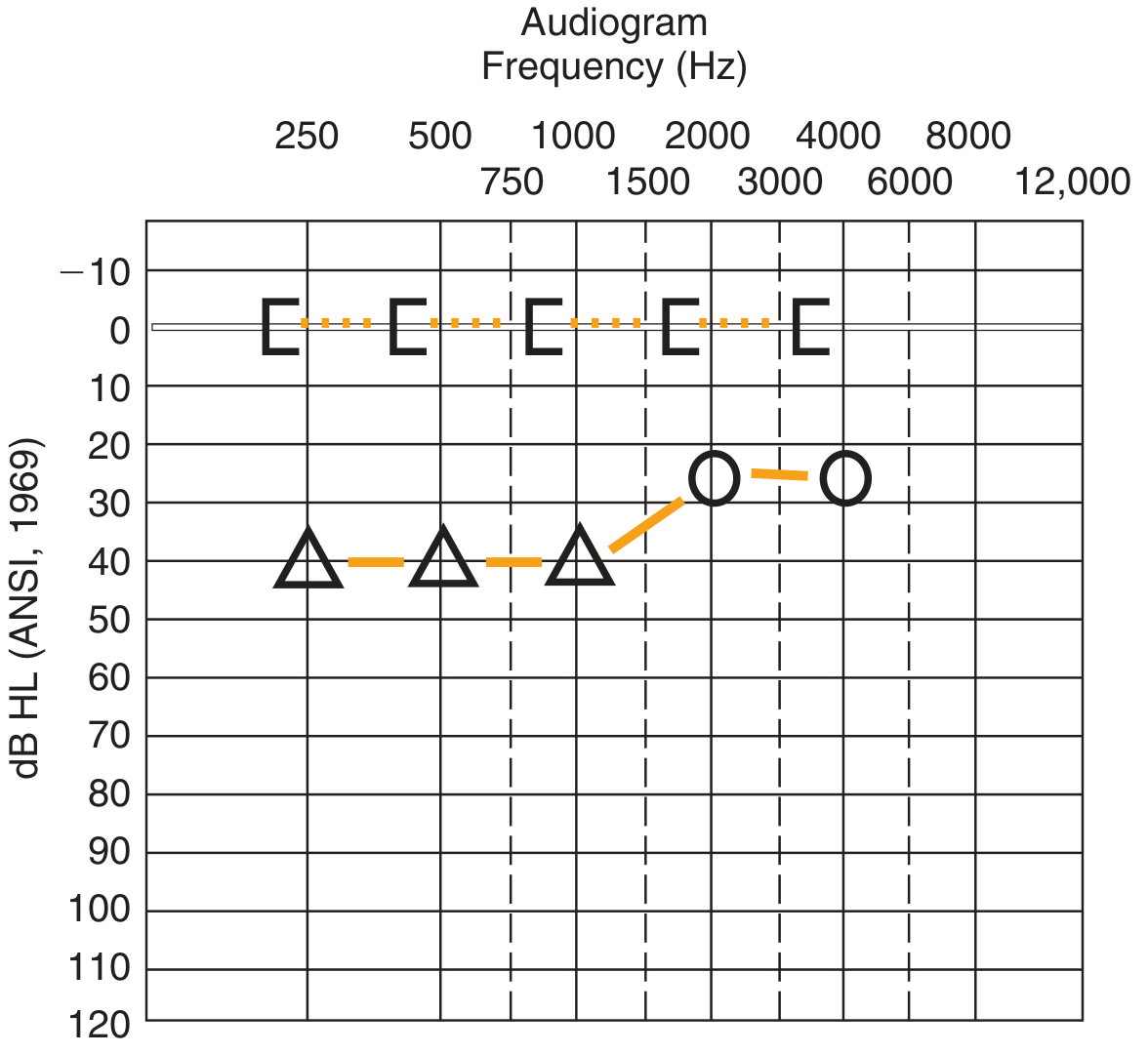
- Bone-conduction thresholds (brackets) sit at 0 dB — normal cochlear function
- Air-conduction thresholds (circles/triangles) are depressed by 30–40 dB
- The vertical gap between the two lines is the air-bone gap
- Implies outer or middle ear pathology (e.g., cerumen impaction, otitis media, otosclerosis, ossicular discontinuity)
- Speech discrimination scores are typically preserved once stimuli are loud enough
Sensorineural Hearing Loss (SNHL)
Both BC and AC are equally elevated → no air-bone gap
- Air-conduction and bone-conduction thresholds track each other (both circles and angle brackets overlap or are very close)
- No gap because the cochlea itself (or the auditory nerve) is impaired
- Implies cochlear or retrocochlear pathology (e.g., noise-induced, presbycusis, ototoxicity, acoustic neuroma, Menière's disease)
- Speech discrimination scores are often reduced, especially in retrocochlear lesions
Mixed Hearing Loss
Both BC and AC are elevated, but an air-bone gap is still present
- BC is elevated (cochlear component)
- AC is elevated further (additional conductive component)
- The gap between AC and BC represents the conductive overlay on top of SNHL
- Example: patient with presbycusis who also develops chronic otitis media
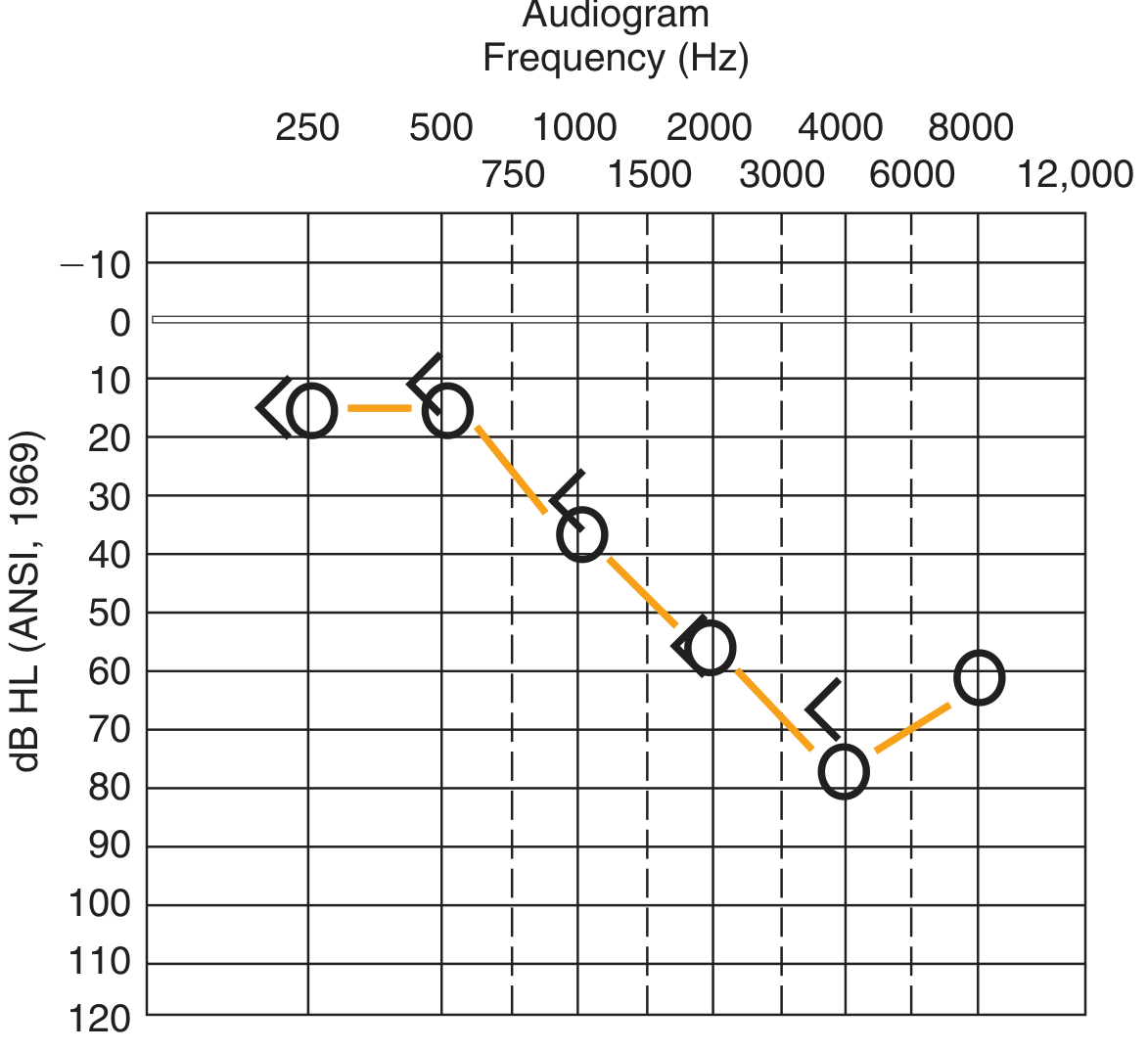
Step 4 — Recognise Audiogram Patterns
Common shapes point to specific diagnoses:
| Pattern | Appearance | Typical Cause |
|---|---|---|
| High-frequency notch at 4 kHz | Dip at 4000 Hz, recovery at 8000 Hz | Noise-induced hearing loss (NIHL) |
| High-frequency sloping loss | Progressive drop from 2–8 kHz | Presbycusis (age-related) |
| Low-frequency loss | Elevated thresholds at 250–1000 Hz | Menière's disease (early stage) |
| Flat loss | Equal elevation across all frequencies | Otosclerosis, hereditary SNHL |
| Cookie-bite / U-shaped | Mid-frequency notch (1–2 kHz) | Hereditary/genetic loss |
| Rising loss (low-freq worst) | Worst at low, better at high | Endolymphatic hydrops |
Step 5 — Speech Tests
Three tests complement the pure-tone audiogram:
| Test | What it measures | Key facts |
|---|---|---|
| Speech Detection Threshold (SDT) | Lowest level to detect presence of speech | ~equals PTA |
| Speech Reception Threshold (SRT) | Level at which 50% of words are correctly repeated | ~8–9 dB above SDT |
| Speech Discrimination / Word Recognition | % of monosyllabic words correctly recognised | Presented 50 dB above SRT |
Interpretation rule:
- Conductive loss → discrimination near normal once volume is sufficient
- Cochlear SNHL → reduced discrimination
- Retrocochlear (CN VIII, auditory cortex) → disproportionately poor discrimination even with near-normal thresholds ("rollover" phenomenon)
Step 6 — Masking
Masking is noise delivered to the non-test ear to prevent it from responding to signals intended for the test ear (called crossover).
When to mask:
- Air conduction: mask when AC stimulus to test ear exceeds the BC threshold of the non-test ear by ≥40 dB (supra-aural headphones) or ≥70 dB (insert earphones)
- Bone conduction: mask whenever the test ear has an air-bone gap > 10 dB (because BC interaural attenuation is essentially 0 dB — the oscillator stimulates both cochleas simultaneously)
Summary Table
| Feature | Conductive | Sensorineural | Mixed |
|---|---|---|---|
| AC threshold | Elevated | Elevated | Elevated |
| BC threshold | Normal | Elevated | Elevated |
| Air-bone gap | Present (>10 dB) | Absent | Present |
| Site of lesion | Outer/middle ear | Cochlea/CN VIII | Both |
| Speech discrimination | Good | Reduced | Variable |
| Typical examples | Otitis media, otosclerosis | Presbycusis, NIHL, Menière's | Otosclerosis + presbycusis |
Sources: Cummings Otolaryngology Head and Neck Surgery; K.J. Lee's Essential Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.