
1000445890.jpg
As per tjis format write examnation of recurrent patella dislocation
Here is the Examination of Recurrent Patella Dislocation written in the Knee Examination Proforma format shown in your image:
Knee Examination Proforma – Recurrent Patella Dislocation
1. Gait, Foot Progression Angle
- Antalgic gait or avoidance gait due to fear of giving way
- Toe-out gait (increased foot progression angle) suggesting external tibial torsion
- Trendelenburg gait if associated hip abductor weakness
2. Attitude
- Knee held in slight flexion to avoid quadriceps contraction
- Leg may be externally rotated
- If currently dislocated: patella visibly displaced laterally, knee held in slight flexion
3. Inspection
-
General findings: Overlying skin - bruising/ecchymosis after acute episode, swelling (hemarthrosis), old scar if previously operated, sinus if infected
-
Specific findings of inspection:a. From front:
- Deformity: Genu valgum (most common predisposing factor), increased Q angle
- Muscle wasting: Vastus medialis obliquus (VMO) wasting prominently
- Position of patella: Patella alta (high-riding patella), lateral tilt of patella, "grasshopper eye" appearance (bilateral lateral displacement)
- Limb length discrepancy
- Supra/parapatellar swelling (hemarthrosis or effusion)
- Pelvis position and ankle-foot: Pes planus, pronated foot, increased femoral anteversion
b. From side:- Sagittal plane deformity: Patella alta visible as high-riding patella
- Flexion deformity if acute episode
- Genu recurvatum (associated with ligamentous laxity)
c. From back:- Popliteal fossa - any swelling
- Spine - scoliosis if associated
- Calf muscle wasting
- Ankle-foot deformity (pes planus)
4. Palpation
- Local rise in temperature (if acute/recent dislocation)
- Tenderness:
- Medial retinaculum tenderness (torn MPFL - medial patellofemoral ligament)
- Lateral retinaculum tenderness
- Medial femoral condyle tenderness (MPFL femoral attachment)
- Lateral patellar facet tenderness
- Anterior knee tenderness
- Joint line tenderness (associated chondral damage)
- Patellar tap - effusion/hemarthrosis
- Crepitus on patellar movement (chondromalacia patellae)
- Synovial hypertrophy
- Retropatellar tenderness (patella-facet grinding)
- Hyperlaxity of joints (generalised ligamentous laxity - Beighton score)
- Confirmation of palpatory characteristics of swelling, scar, sinus, and deformities
5. Movements: Active and passive
- Flexion-extension range: usually full unless acute episode
- Extensor lag (if VMO weak or acute injury)
- Flexion deformity
- Patellar tracking during active flexion-extension: J-sign (patella jumps laterally at terminal extension - pathognomonic of recurrent dislocation)
- Crepitus, clicks during movement
6. Measurements
- Limb length and thigh-calf circumference (VMO wasting quantified)
- Q angle: Increased (>15° in females, >10° in males) - most important measurement
- Intercondylar and intermalleolar distance (for genu valgum assessment)
- TT-TG distance (tibial tubercle to trochlear groove) - radiological, normal <20 mm
- Patellar height ratio (Insall-Salvati ratio) - for patella alta
7. Neurovascular Examination
- Distal pulses (dorsalis pedis, posterior tibial)
- Sensation over anterior knee, medial and lateral aspects
- Peroneal nerve assessment (foot dorsiflexion, first web space sensation)
8. Special Tests
a. Anterior stability tests for ACL: Anterior drawer test, Lachman test, pivot shift test (rule out combined instability)
b. Posterior stability test for PCL: Sag sign, posterior drawer test, Godfrey test, quadriceps active test
c. Tests for stability of posteromedial corner: Valgus stress test at 0° and 30°, Slocum (AMRI) test, external rotation test
d. Tests for stability of posterolateral corner: Varus stress test at 0° and 30°, external rotation recurvatum, Dial test
e. Meniscus test: McMurray's, Apley's grinding, Thessaly test, Payr's test
f. Patella stability and other tests (MOST IMPORTANT in this condition):
- Apprehension test (Clarke's sign): With knee at 30° flexion, examiner pushes patella laterally - positive if patient apprehends or contracts quadriceps in fear of dislocation (pathognomonic)
- Quadrant test: Patella displaced medially and laterally to assess retinacular tightness - lateral retinaculum tightness noted
- Patellar horizontal tilt test: Medial edge of patella cannot be elevated beyond neutral - indicates tight lateral retinaculum
- Patellar glide test: Patella displaced >2 quadrants laterally indicates MPFL laxity
- Patellar tracking: J-sign during active knee extension
- Fulkerson tilt test: Assess patellar tilt
- Beighton score: For generalised ligamentous laxity
g. Wilson test for osteochondritis dissecans (rule out associated osteochondral defect)
9. Joint Above (Hip, Spine) and Below (Ankle)
- Hip: Increased femoral anteversion (Craig's test), hip abductor weakness (Trendelenburg)
- Spine: Lumbosacral alignment
- Ankle-foot: Pes planus, subtalar pronation (increases Q angle dynamically)
10. Lymph Node Examination
- Inguinal lymphadenopathy (if infective etiology considered)
Key Predisposing Factors to Specifically Document:
- Trochlear dysplasia (flat/convex trochlea)
- Patella alta (Insall-Salvati >1.2)
- Increased TT-TG distance (>20 mm)
- MPFL insufficiency
- Increased Q angle / genu valgum
- Generalised ligamentous laxity
- VMO hypoplasia
How to check for genu varus or valgium deformity clinically
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Here is a complete clinical guide to assessing Genu Varum and Genu Valgum:
Clinical Assessment of Genu Varum and Genu Valgum
Definitions
| Term | Description | Common Name |
|---|---|---|
| Genu Varum | Knees bowed outward - center of knee lateral to mechanical axis | Bow legs |
| Genu Valgum | Knees angled inward - center of knee medial to mechanical axis | Knock knees |
Step 1 - Patient Position
- Patient stands barefoot, in light clothing, feet together (medial malleoli touching)
- Patellae facing forward (neutral rotation)
- Knees in full extension
- Examined from the front (AP view)
Step 2 - Visual Inspection (Standing)
For Genu Varum:
- Gap between the knees when feet/ankles are together
- Lower limbs appear bowed outward
- Feet may show lateral border loading / fallen pedal arch
For Genu Valgum:
- Gap between the ankles when knees are touching
- Lower limbs angle inward at the knee
- Associated pes planus, toe-out gait
Step 3 - Clinical Measurement (Key Step)
The standard bedside clinical test uses intercondylar and intermalleolar distances:
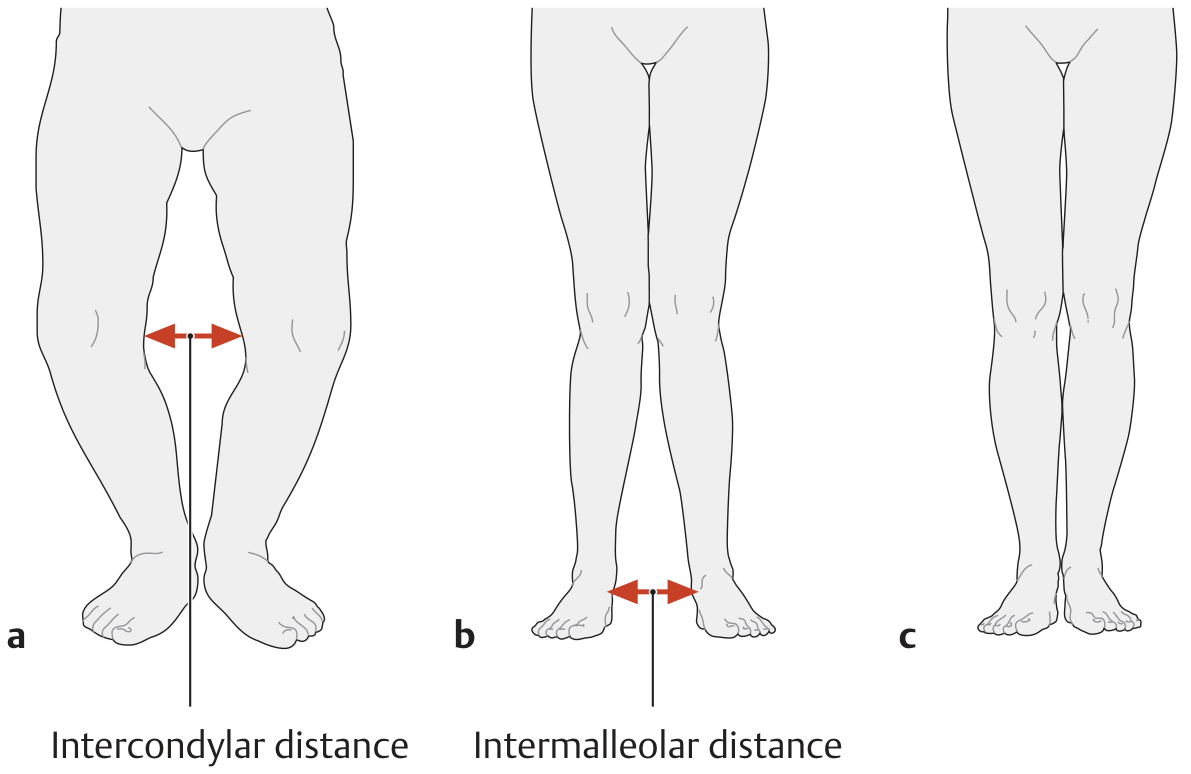
A. Intercondylar Distance - For Genu Varum
- Ask patient to stand with medial malleoli together
- Measure the gap between the medial femoral condyles at the knee
- Use a tape measure or ruler between the most prominent medial condyle points
- Normal: condyles touch (0 cm)
- Abnormal: >3 cm is considered pathological
B. Intermalleolar Distance - For Genu Valgum
- Ask patient to stand with knees together (medial condyles touching)
- Measure the gap between the medial malleoli at the ankle
- Normal: malleoli touch (0 cm)
- Abnormal: >5 cm is considered pathological
(Source: THIEME Atlas of General Anatomy and Musculoskeletal System)
Step 4 - Mechanical Axis Assessment
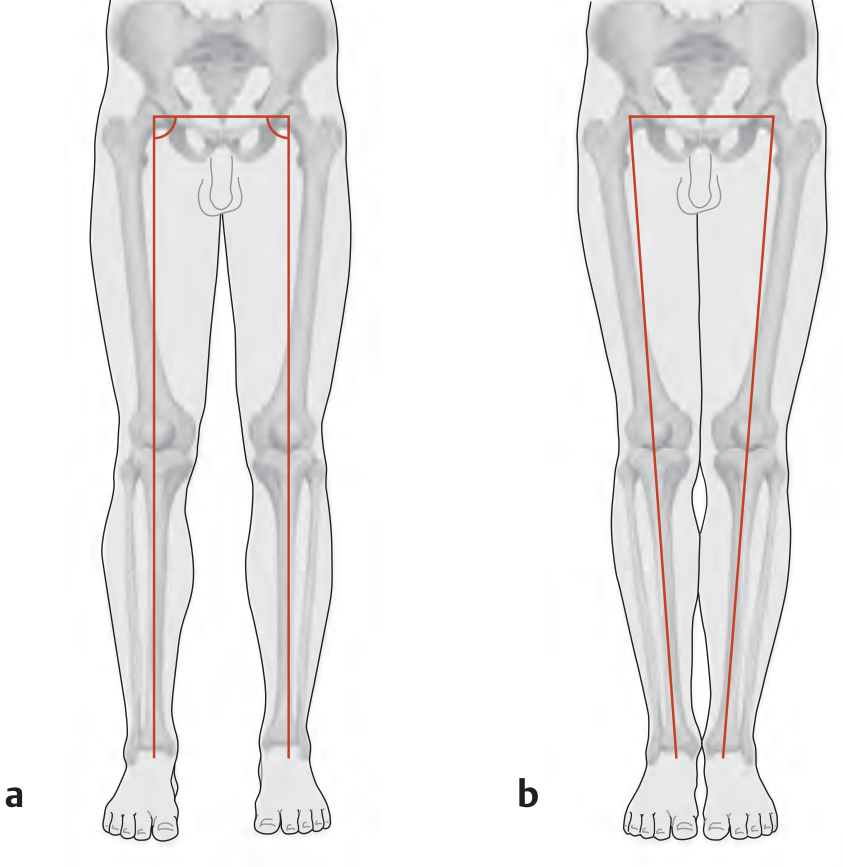
- Normal: The mechanical axis (from center of femoral head to center of ankle) passes through the center of the knee. The femorotibial angle is 174° (a slight physiological valgus).
- Genu Varum: Center of knee joint is lateral to the mechanical axis - medial compartment overloaded
- Genu Valgum: Center of knee joint is medial to the mechanical axis - lateral compartment overloaded
Step 5 - Q Angle Measurement
- Patient: Supine, quadriceps relaxed, knee in full extension
- Line 1: From ASIS (anterior superior iliac spine) to center of patella
- Line 2: From center of patella to tibial tubercle
- The angle between these two lines = Q angle
| Normal | Abnormal | |
|---|---|---|
| Male | 10-14° | >15° suggests valgus tendency |
| Female | 15-17° | >20° suggests valgus tendency |
- Increased Q angle is associated with genu valgum and patellar instability
- Decreased/negative Q angle suggests genu varum
Step 6 - Supine Examination
- Ask patient to lie supine, legs extended and relaxed
- Bring both knees together - confirm deformity persists (structural) vs disappears (postural/flexible)
- Check for fixed vs correctable deformity
- Assess whether deformity is symmetrical or asymmetrical
Step 7 - Gait Assessment
| Finding | Suggests |
|---|---|
| Waddling, wide-based gait | Genu varum |
| Scissor-like, knees crossing | Genu valgum |
| Lateral border foot wear | Genu varum |
| Medial border foot wear, pes planus | Genu valgum |
Step 8 - Associated Findings to Document
| Condition | Genu Varum | Genu Valgum |
|---|---|---|
| Compartment stress | Medial overload | Lateral overload |
| Ligament stress | Lateral collateral lax | Medial collateral lax |
| Foot | Fallen lateral arch | Pes planus |
| Pelvis | Wider-based stance | Narrow-based stance |
| Patella | Facing inward (squinting) | Laterally tilted |
Physiological (Normal) Age-Related Changes
| Age | Normal Finding |
|---|---|
| First year of life | Up to 20° genu varum is normal |
| Around age 2 | Up to 10° genu valgum is normal |
| School age (~6-7 yrs) | Legs straighten - normal adult alignment |
Any deformity persisting or worsening beyond these age norms warrants investigation for rickets, Blount's disease, or metabolic bone disease.
Summary - Quick Bedside Reference
| Test | Genu Varum | Genu Valgum |
|---|---|---|
| Feet together | Gap at knees | Normal or touching at knees |
| Knees together | Normal at ankles | Gap at ankles |
| Intercondylar distance | >3 cm = abnormal | Not applicable |
| Intermalleolar distance | Not applicable | >5 cm = abnormal |
| Q angle | Decreased/normal | Increased (>15° M, >20° F) |
| Mechanical axis deviation | Lateral to knee center | Medial to knee center |
How to measure Q angle precisely during knee examination?
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Here is a complete, precise guide to measuring the Q angle:
Q Angle - Precise Clinical Measurement
What is the Q Angle?
The Quadriceps (Q) angle is the angle formed at the patella between:
- Line 1 (Proximal): From the Anterior Superior Iliac Spine (ASIS) to the center of the patella - represents the line of pull of the quadriceps muscle
- Line 2 (Distal): From the center of the patella to the tibial tubercle - represents the line of the patellar tendon
It reflects the net lateral force vector of the quadriceps on the patella. A higher Q angle = greater lateral pull on the patella.
Equipment Needed
- Standard long-arm goniometer (preferred)
- Skin marker/pen
- Measuring tape
- Patient in appropriate position (see below)
Patient Positioning (Critical for Accuracy)
Standard Method - Supine:
- Patient supine on a flat examination table
- Knee in full extension (0°)
- Quadriceps relaxed (not contracted)
- Hip in neutral rotation - patella facing directly upward
- Feet in neutral position - not internally or externally rotated
Note: Hip rotation significantly affects the Q angle - internal rotation increases it, external rotation decreases it. Always ensure neutral hip position.
Step-by-Step Measurement Technique
Step 1 - Identify and mark 3 bony landmarks with a skin marker:
| Landmark | How to Locate |
|---|---|
| ASIS | Palpate the iliac crest anteriorly - the most prominent anterior bony point of the pelvis |
| Center of patella | Midpoint of the patella - palpate all four borders and mark the center |
| Tibial tubercle | Bony prominence on the anterior tibia just below the knee - most prominent point |
Step 2 - Draw two reference lines (optional but helps with accuracy):
- Line from ASIS to center of patella
- Line from center of patella to tibial tubercle
Step 3 - Place the goniometer:
- Fulcrum (center): Over the center of the patella
- Proximal arm: Aligned toward the ASIS
- Distal arm: Aligned toward the tibial tubercle
Step 4 - Read the angle formed between the two arms at the patella
Normal Values
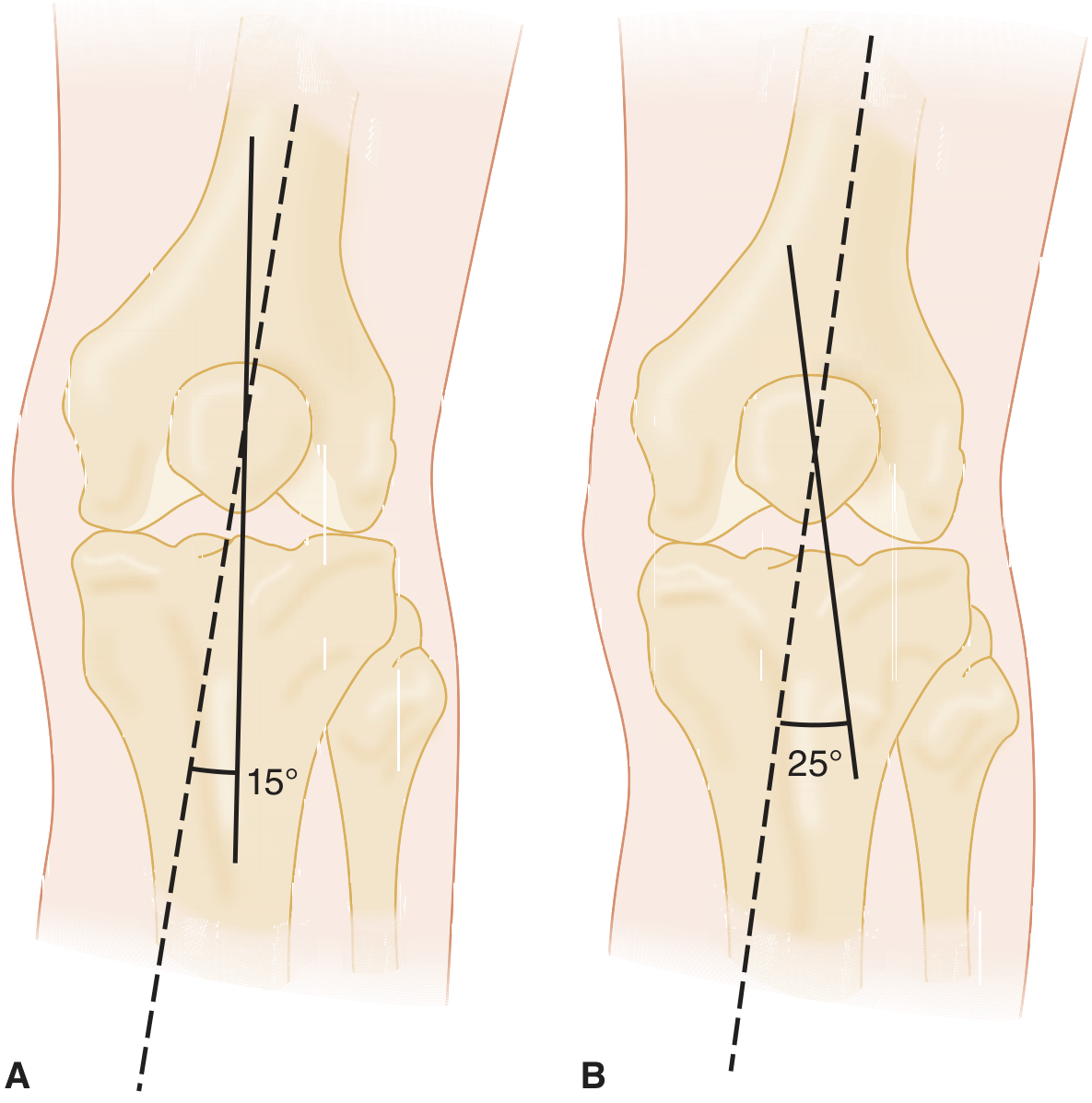
(A - Normal Q angle ~15°. B - Abnormal Q angle ~25° with increased lateral subluxation force - Tintinalli's Emergency Medicine)
| Population | Normal Range | Abnormal |
|---|---|---|
| Males | 10-14° (avg ~13°) | >15° |
| Females | 15-18° (avg ~18°) | >20° |
Females have a higher Q angle due to their broader pelvis (wider pelvis → more lateral ASIS position → greater angle).
(Source: Rheumatology 2-Volume Set, Elsevier 2022)
Why Q Angle is Higher in Females - Anatomy
| Factor | Effect |
|---|---|
| Wider pelvis | ASIS displaced more laterally → increases proximal line angle |
| Increased femoral anteversion | Adds to lateral vector |
| Genu valgum | Common in females → increases Q angle |
| Pes planus / pronated foot | Dynamic increase in Q angle during gait |
Common Errors to Avoid
| Error | Effect on Reading |
|---|---|
| Hip internally rotated | Falsely increases Q angle |
| Hip externally rotated | Falsely decreases Q angle |
| Knee not in full extension | Changes patellar position, alters reading |
| Quadriceps contracted | Patella shifts superiorly, alters angle |
| Marking tibial tubercle inaccurately | Most common source of error |
| Patient obese/difficult landmark palpation | Use fluoroscopy or CT for accuracy |
Q Angle in Standing vs Supine
| Position | Notes |
|---|---|
| Supine (standard) | Most reproducible, eliminates weight-bearing variables |
| Standing | More functional but harder to standardize; Q angle typically slightly higher due to weight-bearing and dynamic muscle activity |
| 30° knee flexion | Patella engages trochlear groove - more clinically relevant for patellar tracking assessment |
Clinical Significance of an Increased Q Angle
| Q Angle | Implication |
|---|---|
| >15° (male) / >20° (female) | Pathological lateral patellar pull |
| High Q angle | Risk of: patellofemoral syndrome, recurrent patellar dislocation, chondromalacia patellae |
| Very high Q angle (>25°) | Likely underlying structural cause - genu valgum, femoral anteversion, lateral tibial torsion, or lateralized tibial tubercle (high TT-TG distance) |
A high Q angle increases the resultant lateral subluxation force on the patella - this is the biomechanical basis for patellar instability and patellofemoral pain syndrome. (Miller's Review of Orthopaedics 9th Ed; Tintinalli's Emergency Medicine)
Associated Radiological Measurement - TT-TG Distance
When Q angle is elevated, confirm with imaging:
- TT-TG (tibial tubercle - trochlear groove) distance on CT or MRI
- Normal: <20 mm
-
20 mm: indication for tibial tubercle medialization (Fulkerson osteotomy)
- This is the radiological equivalent and more precise version of the Q angle
This is a shared conversation. Sign in to Orris to start your own chat.