Describe the etiopathogenesis, diagnosis, management and prevention of rheumatic fever.
Reading File
Finding Sources
Searching PubMed
"rheumatic fever"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have all the information needed. Here is a comprehensive, textbook-grounded answer:
Acute Rheumatic Fever (ARF)
Sources: Harrison's Principles of Internal Medicine 22E (2025); Goldman-Cecil Medicine; Tintinalli's Emergency Medicine
Pathogenetic Pathway (Overview)
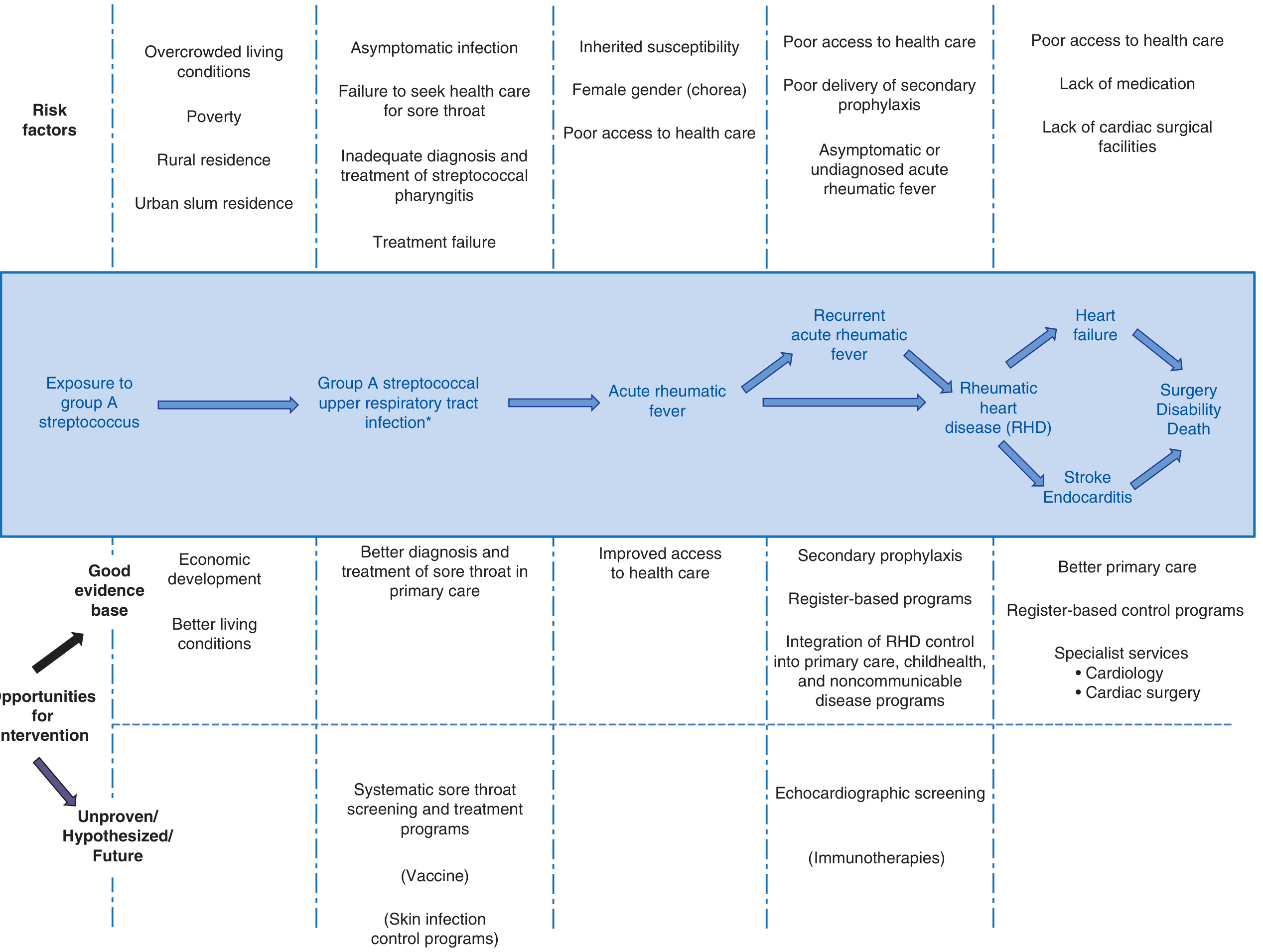
I. Etiopathogenesis
Causative Agent
ARF is a multisystem inflammatory disease resulting from an autoimmune reaction to group A β-hemolytic Streptococcus (GAS, S. pyogenes) pharyngitis (and possibly skin infection in some populations). Only certain strains — particularly those with mucoid capsule types (M-types 3, 5, 18) — are "rheumatogenic." Skin infection without pharyngitis has been epidemiologically linked to ARF in some endemic populations, though not proven beyond doubt.
Molecular Mimicry (Central Mechanism)
The dominant theory of ARF pathogenesis is molecular mimicry:
- GAS M protein (and other surface antigens) contain epitopes structurally similar to human proteins — particularly cardiac myosin, actin, tropomyosin, laminin, and keratin.
- After GAS pharyngitis, antigen-presenting cells present streptococcal antigens to T cells, triggering both humoral and cellular immunity.
- Cross-reactive antibodies bind to endothelial cells of heart valves, activating the adhesion molecule VCAM-1, and recruiting activated lymphocytes.
- Lysis of endothelial cells (in the presence of complement) releases laminin, keratin, and tropomyosin — activating cross-reactive T cells that invade the myocardium and valves, causing epitope spreading and amplifying damage.
- Carditis = antibody binding + T-cell infiltration; arthritis = immune complex deposition in joints; chorea = antibody binding to basal ganglia; skin manifestations = delayed hypersensitivity reactions.
An alternative hypothesis proposes that direct streptococcal invasion of epithelial surfaces, with M-protein binding to type IV collagen, renders host proteins immunogenic — but not through molecular mimicry.
Host Genetic Susceptibility
- Only ~3–6% of any population is susceptible to ARF after GAS infection.
- Familial clustering and 44% concordance in monozygotic twins (vs 12% in dizygotic) confirm a strong inherited component (heritability ~60%).
- Associations found with: HLA class II alleles (DQA and DQB loci), immunoglobulin heavy chain (IGHV4-61*02 allele), complement factor H, TNF polymorphisms, and mannose-binding lectin.
Risk Factors & Epidemiology
- Peak incidence: school-aged children (5–15 years); RHD peaks in the 3rd–4th decades of life.
- ARF is a disease of poverty — overcrowded housing, poor hygiene, limited healthcare access.
- ~40 million people worldwide have RHD; >300,000 deaths/year; 95% in LMICs (sub-Saharan Africa, Pacific, South/Central Asia, Australasia, China).
- Untreated, ARF lasts ~12 weeks on average.
II. Clinical Features
A latent period of ~3 weeks (range 1–5 weeks) separates GAS pharyngitis from ARF onset. Chorea and indolent carditis may have latent periods up to 6 months.
| Manifestation | Frequency | Key Features |
|---|---|---|
| Arthritis | 60–75% | Migratory polyarthritis; large joints (knees, ankles, hips, elbows); asymmetric; severe pain; sterile synovial fluid with lymphocyte predominance |
| Carditis | 50–75% | Pancarditis — endocarditis, myocarditis, pericarditis; mitral valve most commonly affected (regurgitation initially); PR prolongation on ECG |
| Chorea (Sydenham's) | 2–30% | Involuntary, non-rhythmic purposeless movements; asymmetric; stops during sleep; may appear late |
| Erythema marginatum | <5% | Pink, non-pruritic, blanching, serpiginous macules/papules; trunk and proximal limbs |
| Subcutaneous nodules | <5% | Painless, 0.5–2 cm; over bony prominences/extensor tendons; appear 2–3 weeks after onset; associated with carditis |
| Fever | Most cases | Usually high-grade (≥39°C); not present in pure chorea |
Subclinical (echocardiographic) carditis — valvular changes detectable on echo without clinical signs — is now recognized as a significant manifestation in the revised Jones criteria.
III. Diagnosis
There is no pathognomonic test for ARF — it is a diagnosis of exclusion based on clinical criteria plus evidence of antecedent GAS infection.
Jones Criteria (Revised 2015 AHA — Risk-Stratified)
Evidence of preceding GAS infection is required (positive throat culture, rapid streptococcal antigen test, elevated/rising ASO or anti-DNase B titers, or history of scarlet fever).
| Low-Risk Populations (ARF incidence <2/100,000 school-aged children/yr) | Moderate/High-Risk Populations | |
|---|---|---|
| Major criteria | Carditis (clinical or subclinical/echo); polyarthritis; chorea; erythema marginatum; subcutaneous nodules | Same + monoarthritis or polyarthralgia counts as major |
| Minor criteria | Polyarthralgia; fever ≥38.5°C; ESR ≥60 mm/h and/or CRP ≥3.0 mg/dL; prolonged PR interval | Monoarthralgia; fever ≥38.5°C; ESR ≥30 mm/h and/or CRP ≥3.0 mg/dL; prolonged PR interval |
Diagnosis requires:
- Initial ARF: 2 major criteria, or 1 major + 2 minor
- Recurrent ARF: 2 major, or 1 major + 2 minor, or 3 minor
Investigations
- Always: ECG (PR interval), echocardiogram, CBC, CRP/ESR, streptococcal serology (ASO, anti-DNase B)
- As indicated: throat/skin swab culture, blood cultures, synovial fluid (cell count, MC&S, gonococcal PCR), pregnancy test, renal function (before NSAIDs)
- To exclude alternatives: autoantibodies (dsDNA, anti-CCP), STI testing, viral serology (parvovirus B19, CMV, hepatitis, arboviruses)
Echocardiographic Staging of RHD (2023 WHF Guidelines)
| Stage | Features |
|---|---|
| A (Minimal, ≤20 yrs) | Mild MR or AR without morphologic features |
| B (Mild RHD) | Mild regurgitation + ≥1 morphologic feature (≤20 yrs) or ≥2 features (>20 yrs) |
| C (Advanced, asymptomatic) | Moderate/severe MR or AR, any MS or AS, pulmonary HTN, ↓LV systolic function |
| D (Advanced, symptomatic) | Stage C changes + clinical complications (HF, arrhythmia, stroke, endocarditis) |
IV. Management
1. Eradication of GAS (Treatment of Precipitating Infection)
All patients receive antibiotics regardless of culture results:
- Benzathine penicillin G (single IM dose): 1.2 million units (≥27 kg) or 600,000 units (<27 kg) — preferred
- Oral alternatives: Phenoxymethyl penicillin 500 mg BD (250 mg if ≤27 kg) × 10 days; or amoxicillin 50 mg/kg/day (max 1 g) × 10 days
- Penicillin allergy: erythromycin or azithromycin (250 mg daily)
2. Anti-inflammatory Treatment
-
NSAIDs / Salicylates — for arthritis, arthralgia, and fever:
- Aspirin: 50–100 mg/kg/day (max 8 g/day) in 4–5 divided doses — traditional first-line; monitor for salicylate toxicity (tinnitus, nausea)
- Naproxen: 10–20 mg/kg/day BD — preferred by many clinicians due to better GI tolerability
- Continue full dose for ~2 weeks, then taper over 2–4 weeks
- NSAIDs are not of proven benefit for carditis or chorea
-
Corticosteroids — for severe carditis with heart failure:
- Prednisone 1–2 mg/kg/day (max 80 mg) for 2–4 weeks, then taper
- High-quality evidence is lacking; reserved for severe cases
-
Chorea management:
- Usually resolves spontaneously (weeks to months); NSAIDs ineffective
- Severe/persistent cases: sodium valproate or carbamazepine (first-line); haloperidol (alternative)
- IVIg may hasten resolution in severe refractory chorea but has no proven benefit on carditis
3. Carditis / Heart Failure
- Goal-directed heart failure therapy: diuretics, ACE inhibitors/ARBs
- Fluid restriction and bed rest
- Valve surgery is rarely needed acutely; may be required for acute leaflet rupture
4. Hospitalization
- All patients with ARF should be admitted, particularly to confirm the diagnosis and initiate secondary prophylaxis.
V. Prevention
Primary Prevention
The goal is to prevent the initial episode of ARF by preventing or treating GAS pharyngitis.
- Prompt antibiotic treatment of GAS sore throat: If commenced within 9 days of sore throat onset, a full course of penicillin prevents almost all cases of ARF.
- Clinical algorithms are used in resource-limited settings where microbiologic diagnosis is unavailable.
- Improving living conditions — reducing overcrowding, improving hygiene — has historically been the most impactful intervention.
- A GAS vaccine is under active development but not yet available.
Secondary Prevention (Most Critical)
Because patients with a prior ARF episode are at dramatically higher risk of recurrence after any subsequent GAS infection, long-term prophylaxis is mandatory:
| Drug | Dose | Route | Interval |
|---|---|---|---|
| Benzathine penicillin G (preferred) | 1.2 million units (≥27 kg); 600,000 units (<27 kg) | IM | Every 4 weeks (every 3 or 2 weeks in high-risk) |
| Phenoxymethyl penicillin | 250 mg | Oral | Twice daily |
| Azithromycin | 250 mg | Oral | Daily |
Duration of secondary prophylaxis (AHA Recommendations):
| Category | Duration |
|---|---|
| RF without carditis | 5 years after last attack, or until age 21 (whichever is longer) |
| RF with carditis, no residual valvular disease | 10 years after last attack, or until age 21 (whichever is longer) |
| RF with persistent valvular disease (clinical or echo) | 10 years after last attack, or until age 40 (whichever is longer); sometimes lifelong |
- Secondary prophylaxis is best delivered through coordinated RHD control programs based on patient registries, which improve follow-up and adherence tracking.
Tertiary Prevention
- Echocardiographic screening programs in endemic populations to detect subclinical RHD
- Integration of RHD management into primary care and non-communicable disease programs
- Access to cardiology and cardiac surgical services for advanced RHD
Key Points Summary
| Aspect | Core Fact |
|---|---|
| Causative agent | Group A Streptococcus pharyngitis |
| Mechanism | Molecular mimicry → cross-reactive autoimmunity |
| Genetic factor | HLA class II alleles; ~60% heritability |
| Diagnosis | Revised Jones Criteria + evidence of GAS infection |
| Most important valve | Mitral (regurgitation acutely; stenosis with recurrences) |
| Eradication | Benzathine penicillin G single IM dose |
| Arthritis treatment | Aspirin or naproxen |
| Chorea treatment | Valproate / carbamazepine |
| Secondary prophylaxis | Benzathine penicillin G IM every 4 weeks |
| Key complication | Rheumatic heart disease (35–70% of cases) |
Recent evidence note: A 2024 Cochrane systematic review (PMID 39312290) confirmed the role of long-term antibiotic prophylaxis in preventing ARF recurrence and progression to RHD, supporting current guideline recommendations. A 2025 meta-analysis (PMID 40333929) characterized severe adverse reactions to benzathine penicillin G — anaphylaxis remains rare, reinforcing its continued use as the prophylaxis of choice.
- Harrison's Principles of Internal Medicine 22E, Chapter 371
- Goldman-Cecil Medicine, Chapter 269
- Tintinalli's Emergency Medicine, Chapter 141
Classify cyanotic congenital heart disease. How you will manage cyanotic spell in a Tetralogy of Fallot patient
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.