Everything about local anaesthetics
Reading File
Finding Sources
Finding Sources
Searching PubMed
"local anesthetics"[MeSH Terms] AND pharmacology
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Local Anaesthetics - A Comprehensive Overview
Sources: Miller's Anesthesia 10e, Morgan & Mikhail's Clinical Anesthesiology 7e, Barash Clinical Anesthesia 9e, Tintinalli's Emergency Medicine, Bailey & Love's Surgery 28e
1. Definition and Classification
Local anaesthetics (LAs) are drugs that reversibly block nerve impulse conduction to abolish sensation in a specific region of the body without loss of consciousness. All clinically useful agents are either aminoesters or aminoamides.
The Local Anaesthetic Molecule
The typical LA molecule (e.g., lidocaine, procaine) has three parts:
- Lipophilic aromatic ring - gives the molecule its membrane-penetrating ability
- Intermediate chain - contains either an ester (-C-O-) or amide (-NHC-) linkage
- Hydrophilic tertiary amine - partially protonated at physiologic pH, giving it some positive charge
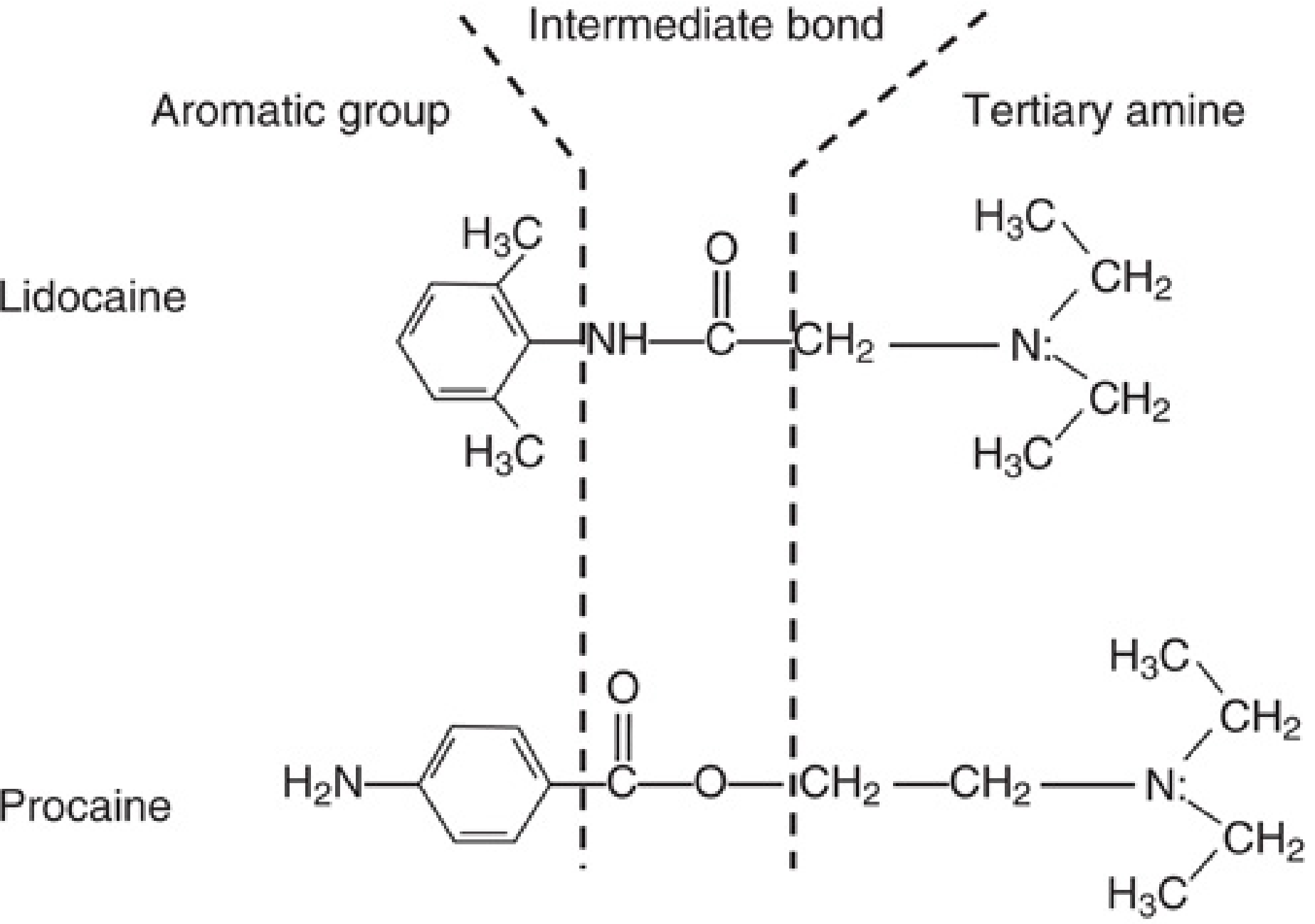
Fig: The aminoamide lidocaine and aminoester procaine. In both, a hydrophobic aromatic group is joined to a hydrophilic tertiary amine by an intermediate ester or amide bond.
2. Classification of Local Anaesthetics
Aminoesters
Metabolized by pseudocholinesterase (butyrylcholinesterase) in plasma. Rapid metabolism. Metabolized to p-aminobenzoic acid (PABA), which is responsible for rare allergic reactions.
| Drug | Duration | Notes |
|---|---|---|
| Cocaine | - | Topical only; vasoconstrictor; metabolized in liver |
| Procaine | Short | Spinal, local infiltration |
| Chloroprocaine | Short | Fastest onset due to low toxicity allowing high concentration (3%); epidural, infiltration |
| Tetracaine (amethocaine) | Long | Spinal, topical eye; max dose 3 mg/kg |
| Benzocaine | - | Topical only; causes methemoglobinemia |
Aminoamides
Metabolized by hepatic microsomal P-450 enzymes (N-dealkylation, hydroxylation). Slower metabolism: prilocaine > lidocaine > mepivacaine > ropivacaine > bupivacaine. No PABA production; allergic reactions are extremely rare.
| Drug | Duration | Max dose | Notes |
|---|---|---|---|
| Lidocaine (lignocaine) | Medium | 4.5 mg/kg (7 with epi) | Most versatile; epidural, spinal, IV regional, topical, infiltration, nerve block |
| Mepivacaine | Medium | 4.5 mg/kg (7 with epi) | Similar to lidocaine; epidural, peripheral nerve blocks |
| Prilocaine | Medium | 6 mg/kg | EMLA cream; causes methemoglobinemia at higher doses |
| Bupivacaine | Long | 3 mg/kg | Widely used epidural; superior sensory/motor differential block; most cardiotoxic |
| Ropivacaine | Long | 3 mg/kg | Less motor block than bupivacaine; 30-40% less cardiotoxic than bupivacaine |
| Levobupivacaine | Long | 3 mg/kg | S-enantiomer of bupivacaine; less cardiotoxic than racemic bupivacaine |
3. Mechanism of Action
Sodium Channel Blockade
LAs work primarily by blocking voltage-gated sodium (Na+) channels in nerve cell membranes, preventing the inward Na+ current that underlies the action potential.
Normal physiology: At rest, the neural membrane maintains a resting potential of -60 to -90 mV. The Na+/K+ ATPase pump sustains this by extruding Na+ in exchange for K+. Upon depolarization, voltage-gated Na+ channels open transiently, allowing Na+ influx and propagating the action potential.
LA action: By blocking these Na+ channels, LAs prevent membrane depolarization and thus block impulse conduction entirely.
The Na+ Channel Binding Site
The Na+ channel alpha subunit has four homologous domains (D-1 to D-4), each with six transmembrane helices (S1-S6). The LA binding site is Site 9 on the inner face of the channel (inside the pore). This is distinct from Site 1 where tetrodotoxin (TTX) binds.
- S4 segments carry positive charges that move outward during depolarization (voltage sensing)
- S6 segments form the inner gate; their conformational changes open/close the channel
- D-3 to D-4 inactivation loop binds the cytoplasmic face to inactivate the channel
State-Dependent (Use-Dependent) Block
LAs bind more avidly to open and inactivated channels than to channels in the resting state. This is described by two complementary models:
- Guarded receptor model - binding sites become accessible during activation (open state)
- Modulated receptor model - drug dissociation from inactivated channels is slower than from resting channels
The result: the more frequently a nerve fires, the more LA binding occurs - this is called phasic or use-dependent block. It explains why rapidly firing neurons (pain fibers, ectopic foci) are more sensitive to LAs.
Ionic Form and Activity
LAs are weak bases. They exist in two forms:
- Uncharged (neutral) form - lipid-soluble, crosses nerve sheaths and membranes
- Charged (cationic) form - actually blocks the Na+ channel from the inside
The pKa determines the balance between these forms at physiologic pH (7.4). A drug with pKa closer to 7.4 has more uncharged drug available at tissue pH, giving faster onset.
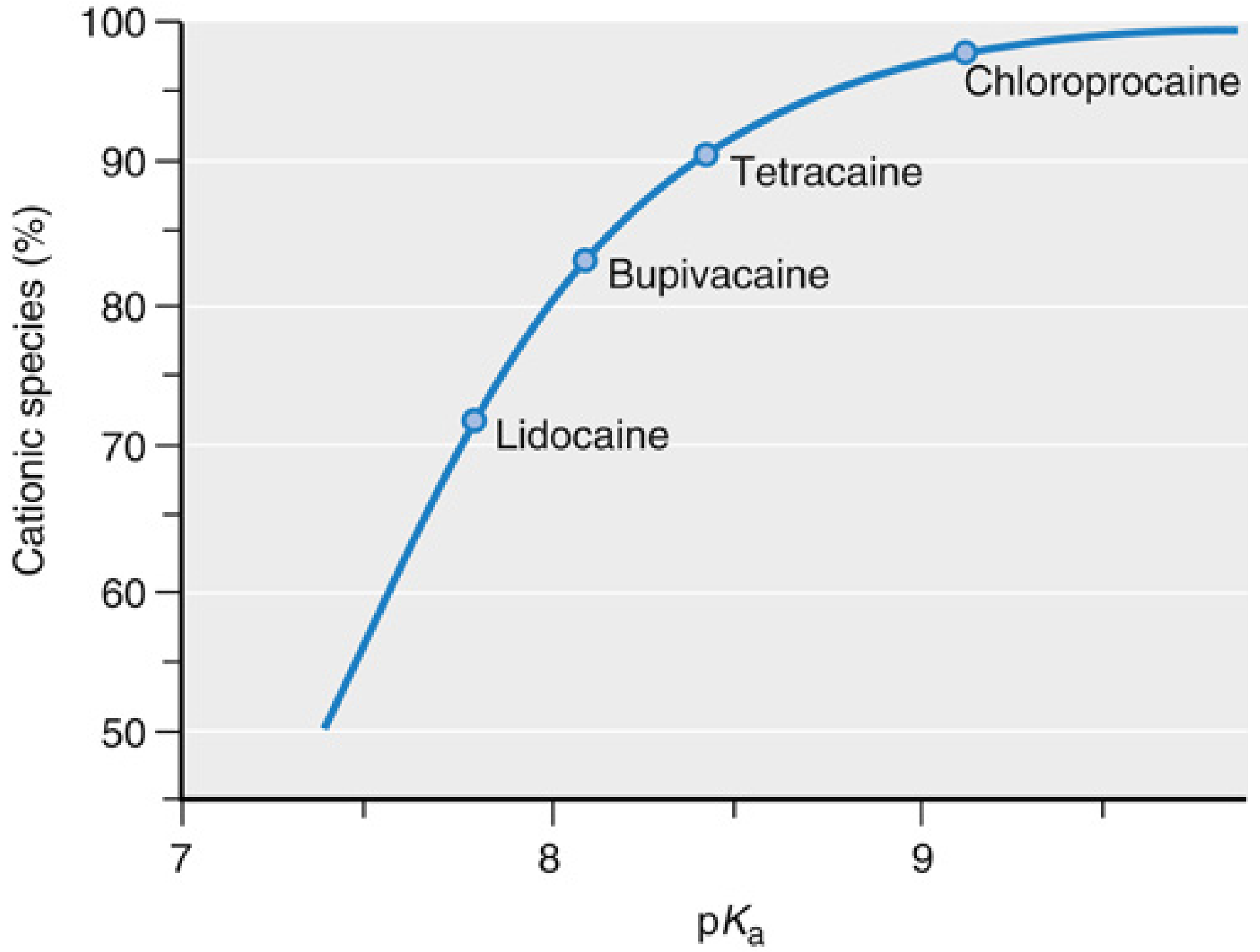
Fig: Fraction of LA in protonated (cationic) form at pH 7.4 as a function of pKa. Lidocaine (lowest pKa) has the largest fraction in neutral form, explaining its faster onset.
Why LAs work poorly in infected tissue: Infected tissues are acidic (low pH). At low pH, more LA is converted to the charged cation, reducing the lipid-soluble uncharged form available to cross membranes. Onset is slower and block may be incomplete.
4. Physicochemical Properties and Clinical Correlations
| Property | Effect on Clinical Use |
|---|---|
| Lipid solubility | Higher = greater potency, longer duration, more protein binding, slower absorption |
| pKa | Lower pKa = more uncharged drug at pH 7.4 = faster onset (lidocaine pKa 7.9 vs chloroprocaine 9.1) |
| Protein binding | Higher binding (bupivacaine 95%) = longer duration; lower binding (procaine 6%) = shorter duration |
| Vasodilator activity | Most LAs cause vasodilation at clinical concentrations (shortening duration); cocaine is the exception - it causes vasoconstriction |
Nerve Fiber Susceptibility
Smaller and unmyelinated fibers are generally more susceptible to LA blockade. The order of block is approximately:
- B fibers (preganglionic autonomic) - most sensitive
- C fibers (unmyelinated pain, temperature)
- Aδ fibers (sharp pain, temperature)
- Aβ fibers (touch, pressure)
- Aα fibers (motor) - least sensitive (largest, most myelinated)
This underlies differential sensory/motor block - dilute solutions preferentially block pain before motor function, which is exploited in epidural analgesia for labour.
5. Pharmacokinetics
Absorption
The rate of systemic absorption depends on:
- Site of injection - highest blood levels: intercostal > caudal > epidural > brachial plexus > sciatic/femoral > subcutaneous
- Dose and concentration used
- Addition of vasoconstrictors (epinephrine reduces peak concentration in blood)
- Drug's intrinsic vasodilator properties
- Lipid solubility of the drug (more lipid-soluble = more tissue-bound = slower absorption)
Distribution
Following absorption, highly perfused organs (brain, lung, liver, kidney, heart) rapidly remove LAs from the blood (initial rapid phase). The lung is particularly important as a "first-pass" extractor - patients with right-to-left cardiac shunts are more vulnerable to IV lidocaine toxicity because this lung extraction is bypassed.
Muscle provides the largest reservoir due to its mass.
Metabolism
- Esters: Hydrolyzed by pseudocholinesterase (plasma). Very rapid. Cocaine is the exception - metabolized in the liver. Patients with pseudocholinesterase deficiency have theoretically slower ester metabolism.
- Amides: Hepatic P-450 enzymes (N-dealkylation, hydroxylation). Rate: prilocaine > lidocaine > mepivacaine > ropivacaine > bupivacaine. Liver disease reduces metabolism significantly.
Very little unmetabolized LA is excreted by the kidney.
6. Additives and Adjuncts
Vasoconstrictors (Epinephrine)
- Causes local vasoconstriction at injection site
- Reduces peak plasma concentration, facilitates neuronal uptake, prolongs block duration (by up to 50% for lidocaine), reduces toxicity
- Effect more pronounced for shorter-acting agents; limited effect on bupivacaine peripheral nerve block duration
- Typical concentration: 1:200,000 (5 mcg/mL)
Sodium Bicarbonate (Alkalinisation)
- LA solutions are acidic (pH 3.3-6.8) for stability and bacteriostasis
- Adding sodium bicarbonate (1 mEq/10 mL) raises pH, increases the uncharged fraction, and accelerates onset
- Not used with bupivacaine (precipitates above pH 6.8)
Opioids
- Added to epidural/intrathecal LAs for synergistic analgesia
- Act on spinal opioid receptors, allowing dose reduction of LA and reduced motor block
Dexamethasone / Steroids
- Prolongs peripheral nerve blocks by up to 50%
Clonidine / Alpha-2 agonists
- Augment analgesia via activation of α2-adrenergic receptors
7. Clinical Applications
Topical Anaesthesia
- EMLA cream (lidocaine 2.5% + prilocaine 2.5%) - intact skin, requires 60 min under occlusive dressing
- Tetracaine gel (Ametop) - 30 min for intact skin
- Cocaine - ENT surgery; unique as it combines anaesthesia with vasoconstriction
- Benzocaine sprays - topical mucosal anaesthesia (caution: methemoglobinemia)
Infiltration Anaesthesia
- Direct injection into tissue; onset immediate for all agents
- Any LA can be used; duration varies by agent and whether epinephrine is added
- Large areas: use dilute solutions in high volumes
Peripheral Nerve Blocks
- Injection near major nerve trunks or plexuses (brachial, femoral, sciatic, etc.)
- Ultrasound guidance has reduced onset times and made LA mixing less critical
- Bupivacaine, ropivacaine, levobupivacaine common for long procedures
Intravenous Regional Anaesthesia (Bier Block)
- Lidocaine 0.5% injected IV into exsanguinated, tourniquet-isolated limb
- Only lidocaine used (bupivacaine too cardiotoxic if tourniquet fails)
- Duration limited to tourniquet time
Epidural Anaesthesia/Analgesia
- Widely used for labour, surgery, post-op pain
- Bupivacaine, ropivacaine, lidocaine most common
- Onset slower than spinal; more variable anatomy
- Alkalinisation accelerates onset
- Sacral sparing can occur due to large L5-S2 nerve roots
Spinal (Intrathecal) Anaesthesia
- Direct injection into CSF; reliable, rapid onset
- Tetracaine, bupivacaine, lidocaine used
- Dose requirements lower (no dural barrier to cross)
Pregnancy considerations
- Spread and depth of neuraxial block greater in pregnancy (dilated epidural veins reduce space volume + progesterone increases nerve susceptibility)
- Dosage should be reduced in all stages of pregnancy
8. Systemic Toxicity (LAST - Local Anaesthetic Systemic Toxicity)
LAST results from accumulation of LA in the systemic circulation - either from inadvertent intravascular injection or unanticipated rapid absorption. Both the CNS and cardiovascular systems are particularly vulnerable.
CNS Toxicity (appears first, at lower plasma levels)
Dose-dependent progression with lidocaine as the example:
| Plasma concentration (mcg/mL) | Effect |
|---|---|
| 1-5 | Analgesia |
| 5-10 | Lightheadedness, tinnitus, numbness of tongue, metallic taste (perioral paraesthesia) |
| 10-15 | Seizures, unconsciousness |
| 15-25 | Coma, respiratory arrest |
| >25 | Cardiovascular depression |
CNS toxicity correlates directly with LA potency (lipid solubility). Factors that worsen CNS toxicity: acidosis, hypercapnia, decreased protein binding, reduced clearance.
Cardiovascular Toxicity (occurs at higher concentrations)
All LAs can cause hypotension, dysrhythmias, and myocardial depression. More potent, lipid-soluble agents (bupivacaine especially) can cause:
- Bradycardia and hypotension
- Wide complex dysrhythmias
- Complete heart block
- Cardiovascular collapse
Bupivacaine is particularly dangerous because it accumulates in cardiac Na+ channels during systole (fast on, slow off) and the block accumulates with successive heartbeats - the "fast-in, slow-out" kinetics. Ropivacaine and levobupivacaine are 30-40% less cardiotoxic than bupivacaine.
Importantly, 10-20% of LAST cases present with cardiovascular signs alone, without preceding neurologic symptoms - requiring high clinical vigilance.
Treatment of LAST
- Stop injection immediately
- Airway management - 100% oxygen; intubate if unconscious
- Seizures - benzodiazepines (first line); avoid propofol in cardiovascular compromise
- Intravenous lipid emulsion (20% Intralipid):
- Bolus: 1.5 mL/kg IV over 1 minute
- Infusion: 0.25 mL/kg/min continued for 10 min after haemodynamic stability
- Maximum dose: ~10 mL/kg over first 30 min
- Mechanism: "lipid sink" - sequesters lipid-soluble LA away from target tissues
- CPR if cardiac arrest - prolonged resuscitation may be needed
- Avoid vasopressin, calcium channel blockers, beta-blockers (worsen bupivacaine toxicity)
- ECMO if refractory
9. Specific Side Effects by Drug
Prilocaine and Benzocaine - Methemoglobinemia
- Prilocaine is metabolized to ortho-toluidine, which oxidizes haemoglobin Fe2+ to Fe3+ (methemoglobin)
- Benzocaine sprays also cause methemoglobinemia
- Treatment: IV methylene blue 1-2 mg/kg of 1% solution over 5 min (reduces Fe3+ back to Fe2+)
Cocaine
- The only LA that causes vasoconstriction (blocks norepinephrine reuptake)
- Used only topically in ENT surgery
- Abuse potential; cardiovascular stimulant effects
Chloroprocaine
- Fastest onset among all LAs (low toxicity permits high concentration)
- Very short duration (rapidly hydrolyzed)
- Historical concern about neurotoxicity with intrathecal use (now resolved with newer formulations)
EMLA (Eutectic Mixture)
- Lidocaine 2.5% + prilocaine 2.5%; eutectic mixture has lower melting point than either component alone, allowing cream formulation
- Applied under occlusive dressing to intact skin for 60 minutes
- Causes initial vasoconstriction, then vasodilation after 2+ hours
10. Allergy
True allergy to LAs is rare. Important distinctions:
- Ester LAs (procaine, tetracaine) - metabolized to PABA, which causes the rare true allergic reactions. Cross-reactivity within ester group occurs.
- Amide LAs - NOT metabolized to PABA; true allergic reactions are extremely rare
- Preservatives (methylparaben, metabisulfite) in multi-dose vials can cause reactions and should be considered
- Cross-reactivity between esters and amides does NOT occur
11. Contraindications and Cautions
- Infection at injection site - risk of spreading infection; LA efficacy reduced in acidic infected tissue
- Coagulopathy - contraindication to neuraxial blocks
- Patient refusal
- Known hypersensitivity to specific drug class
- Hepatic failure - reduces metabolism of amide LAs; dose reduction required
- Pseudocholinesterase deficiency - theoretically prolongs ester LA effect
- Cardiac conduction disease - increased risk from cardiotoxic agents
- Myasthenia gravis - caution with aminoesters
Quick Reference Summary
| Feature | Esters | Amides |
|---|---|---|
| Linkage | -CO- | -NHC- |
| Metabolism | Plasma pseudocholinesterase | Hepatic P-450 |
| Allergy | Yes (PABA) | Very rare |
| Stability | Less stable | More stable |
| Examples | Procaine, cocaine, tetracaine, chloroprocaine, benzocaine | Lidocaine, bupivacaine, ropivacaine, mepivacaine, prilocaine, levobupivacaine |
Mnemonic for amides: "I'll PLAY" = I (prilocaine), L (lidocaine), P (prilocaine - already counted), A (articaine), L (levobupivacaine), Y - or more simply, amides have a double 'i' in the generic name (lidocaine, bupivacaine, ropivacaine, mepivacaine, prilocaine - all have "-caine" with a vowel before it).
Simpler mnemonic: Amides have two 'i's in their name (lIdocaIne, bupIvacaIne, ropIvacaIne etc.)
- Miller's Anesthesia, 10e, Ch. 25 | Morgan & Mikhail's Clinical Anesthesiology 7e, Ch. 16 | Barash Clinical Anesthesia 9e, Ch. 22 | Tintinalli's Emergency Medicine, Ch. 36
This is a shared conversation. Sign in to Orris to start your own chat.