Osteomyelitis
Reading File
Finding Sources
Searching PubMed
osteomyelitis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Loading Image
Reading File
Reading File
I now have rich, comprehensive content from multiple authoritative sources. Let me compose the full answer.
Osteomyelitis
Osteomyelitis is inflammation of bone and bone marrow, virtually always due to infection. It ranges from an acute febrile illness in a child to a chronic, debilitating condition with sinus tracts and sequestrum in adults.
1. Routes of Infection
Three pathways allow organisms to reach bone:
- Hematogenous spread - the most common route in children; bacteremia from trivial mucosal injury or skin infection seeds the metaphysis
- Contiguous spread - from adjacent soft tissue infection (e.g., diabetic foot ulcer, pressure sore)
- Direct inoculation - open fracture, orthopedic surgery, or penetrating trauma
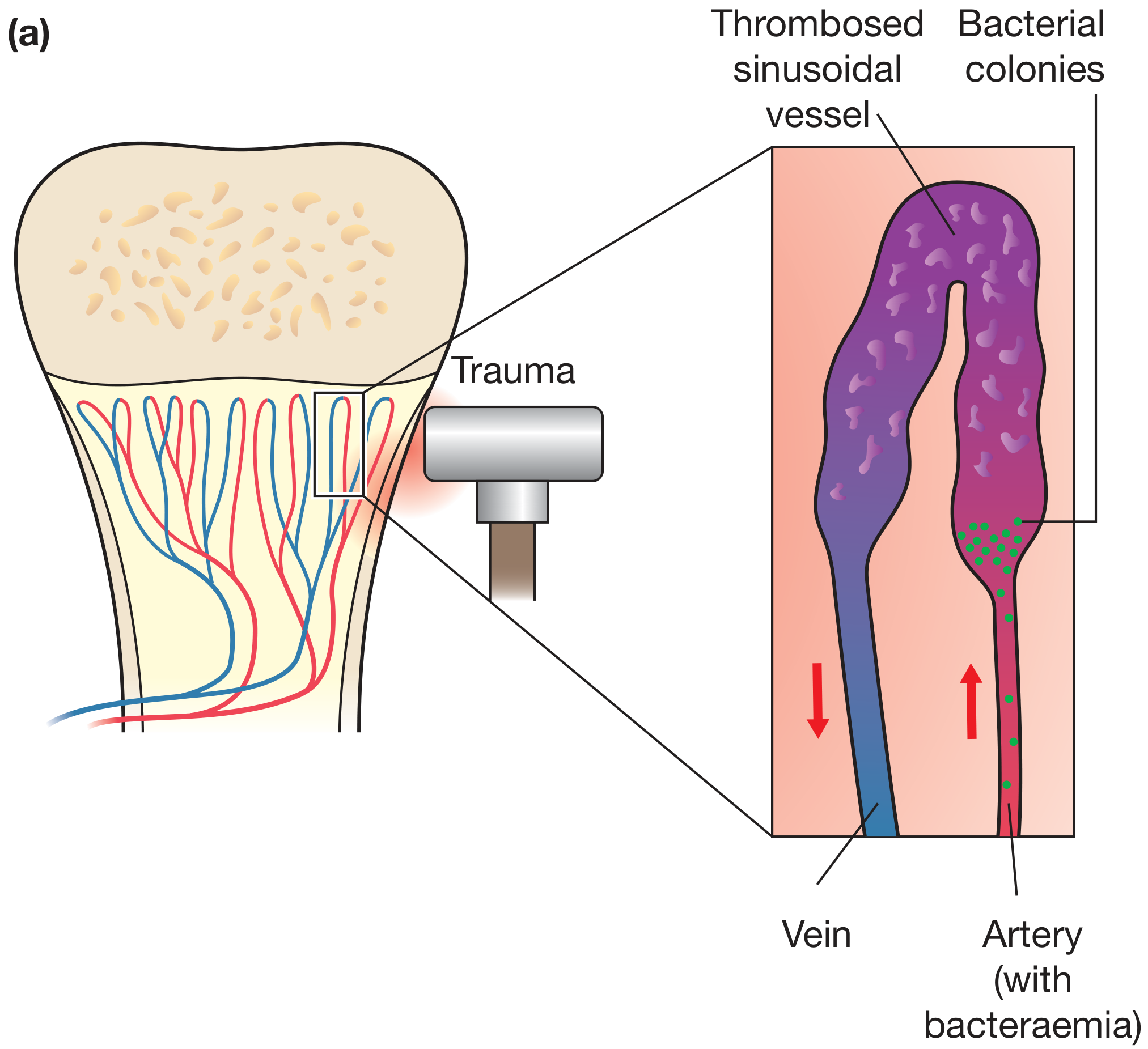
2. Why the Metaphysis?
The metaphysis is the preferential site in children because its vasculature consists of looped sinusoidal vessels with slow, turbulent flow. Microtrauma causes micro-tears that allow bacteremic organisms to seed these vessels, which thrombose and form bacterial colonies.
Age-related variation in site:
- Neonates: metaphyseal vessels penetrate the growth plate, so epiphyses and joints are frequently co-infected
- Older children: metaphysis is the primary site; epiphyseal vessels are blocked by the growth plate
- Adults: after growth plate closure, anastomoses reform between metaphyseal and epiphyseal vessels, so epiphyses and subchondral regions are more commonly involved
3. Causative Organisms
| Setting | Likely Organisms |
|---|---|
| All ages (most common) | S. aureus (80-90% of culture-positive cases) |
| Neonates | Group B Streptococcus, E. coli |
| Children | S. aureus, Streptococcus pyogenes, H. influenzae (less common since vaccination) |
| Sickle cell disease | Salmonella spp., gram-negatives (functional asplenia + areas of osteonecrosis as nidi) |
| Diabetics / foot infection | Mixed flora, gram-negatives |
| Open fracture / surgery | Polymicrobial, Pseudomonas, Acinetobacter |
| IV drug users | Pseudomonas, Candida |
| Immunocompromised | Mycobacteria, fungi (Coccidioides, Blastomyces, Cryptococcus) |
S. aureus binds bone matrix collagen via cell wall proteins, explaining its predilection for bone.
Note: Cultures identify a causative organism in only ~50% of cases; PCR assays targeting microbial DNA are improving this figure.
4. Pathology by Stage
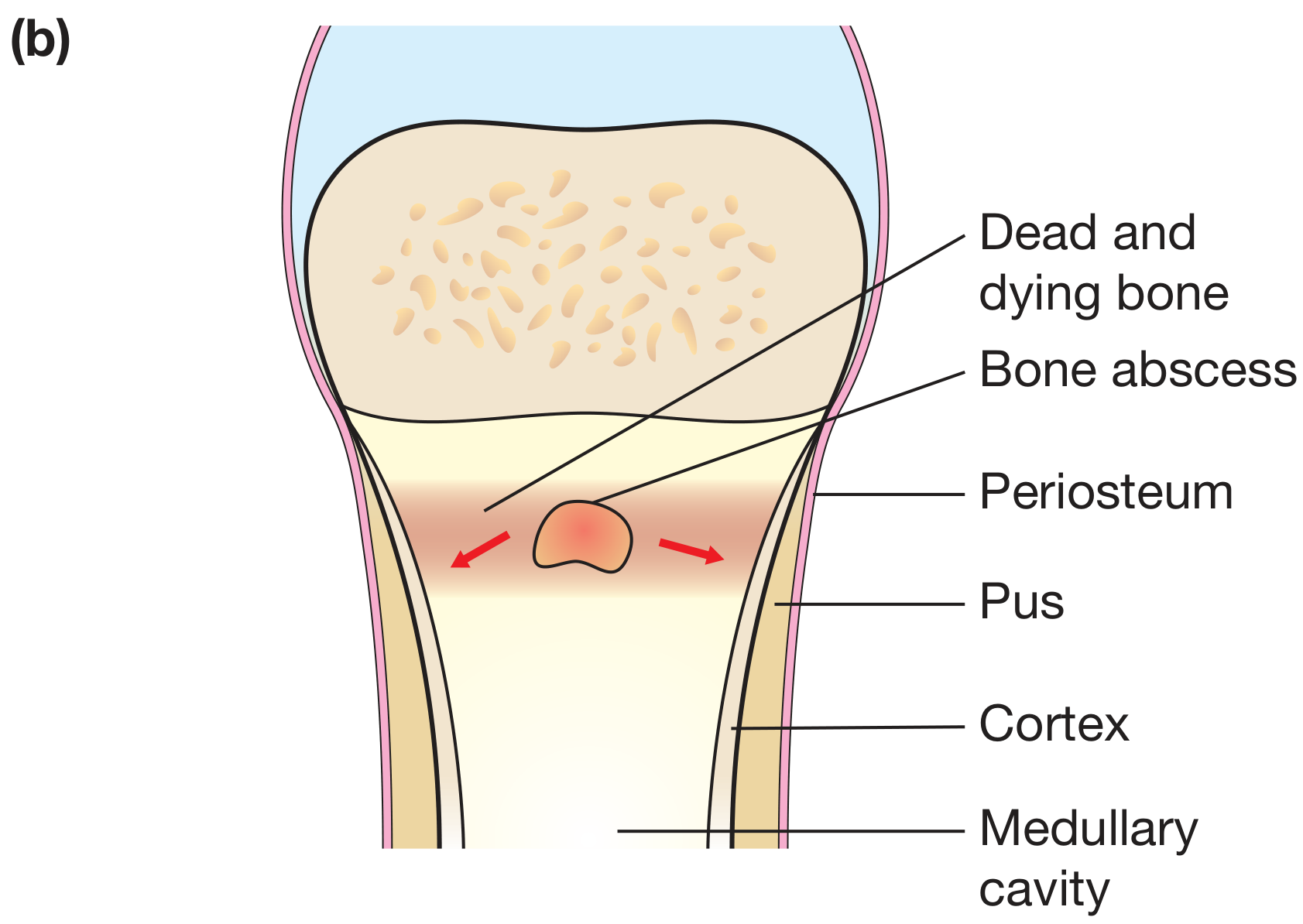
Acute (first 48 hours)
- Bacteria proliferate and induce a neutrophilic infiltrate
- Necrosis of osteocytes and marrow develops within 48 hours
- Bacteria spread through Haversian canals to the periosteum
- In children, the periosteum is loosely attached - subperiosteal abscesses form and dissect along the bone
- Periosteal lifting further impairs cortical blood supply
Subacute / Chronic
- Chronic inflammatory cells (lymphocytes, plasma cells) replace neutrophils
- Cytokines drive bone resorption, fibrous tissue ingrowth, and reactive bone at the periphery
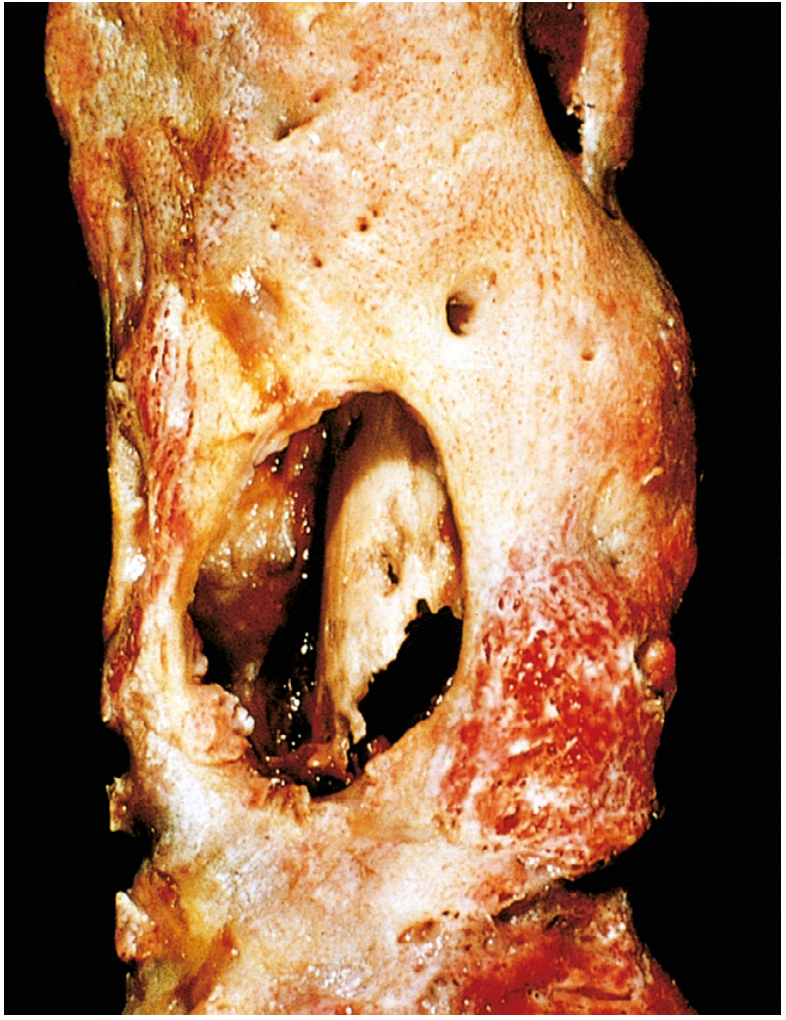
- Sequestrum: avascular dead bone fragment, a nidus for persistent infection
- Involucrum: shell of reactive periosteal new bone that encases the sequestrum - creates the classic "bone within a bone" radiographic appearance
- Pus may track through gaps in the involucrum, penetrate the skin, and form sinus tracts (cloacae)
- Brodie abscess: well-defined lytic lesion with a sclerotic rim - a characteristic of subacute osteomyelitis
5. Clinical Features
Acute hematogenous osteomyelitis (children):
- Fever, chills, malaise, vomiting
- Refusal to bear weight (lower extremity) or use the limb
- Point tenderness over the affected metaphysis - the most reliable physical sign
- Localized warmth, swelling, erythema (variable)
- Sympathetic joint effusion may develop even without joint infection
- Male:female ratio approximately 2-3:1
- Long bones in ~80% of cases (distal femur, proximal tibia, proximal humerus most common)
Adults:
- Presentation is often more subtle
- Fever may be low-grade or absent
- Localized bone pain and tenderness
- In chronic disease: sinus tracts, palpable involucrum/sequestrum, intermittent flares after years of dormancy
Special: Spinal osteomyelitis (vertebral osteomyelitis/discitis)
- Most common in adults >50 years
- Back pain + fever, often indolent onset
- Neurologic compromise possible if epidural abscess forms
6. Investigations
Blood tests:
- Elevated WBC, ESR, CRP (ESR and CRP more sensitive than WBC)
- Blood cultures positive in ~40% of acute hematogenous cases in children
Imaging:
| Modality | Findings | Notes |
|---|---|---|
| Plain X-ray | Soft tissue swelling, lytic destruction, periosteal reaction | Lags 10-21 days behind infection; first sign is soft tissue swelling |
| Ultrasound | Subperiosteal fluid/abscess | Useful in children; guides aspiration |
| Bone scan (Tc-99m) | Hot spot within hours | Sensitive but not specific; useful for multifocal disease in neonates |
| CT | Cortical destruction, sequestra, sinus tracts | Better than X-ray for bone detail |
| MRI | Marrow edema, abscess, soft tissue extension | Highest sensitivity and specificity; modality of choice; shows penumbra sign in subacute infection (high-signal granulation tissue around low-signal abscess core) |
Radiographic changes may not be apparent for up to 2 weeks after onset, so MRI should not be withheld pending plain film changes.
Microbiological:
- Bone biopsy with culture remains the gold standard for pathogen identification
- Surface wound swabs are unreliable and should not substitute for deep cultures
7. Classification
Waldvogel Classification (classic):
- Hematogenous
- Contiguous focus without vascular insufficiency
- Contiguous focus with vascular insufficiency (e.g., diabetic foot)
Cierny-Mader Classification (anatomic + host):
- Stage I: Medullary (endosteal disease only)
- Stage II: Superficial (cortical surface only)
- Stage III: Localized (full thickness cortex, stable bone)
- Stage IV: Diffuse (unstable bone requiring reconstruction)
- Combined with host class A (normal), B (compromised), or C (treatment worse than disease)
8. Complications
- Bacteremia and sepsis
- Septic arthritis (especially in neonates and when metaphysis is intracapsular)
- Chronic osteomyelitis (5-25% of acute cases)
- Pathologic fracture
- Growth disturbance / limb length discrepancy (if epiphyseal plate is damaged in children)
- Squamous cell carcinoma arising in a chronic draining sinus tract (Marjolin's ulcer)
- Secondary (reactive) amyloidosis
- Endocarditis
9. Treatment
General Principles
- Drain pus (surgical drainage where indicated)
- Rest and splint the affected limb
- Analgesia
- Targeted antibiotic therapy
Antibiotics
Empirical therapy should cover S. aureus as a priority:
- Methicillin-sensitive S. aureus (MSSA): penicillinase-resistant penicillin (oxacillin, nafcillin) or first-generation cephalosporin
- MRSA suspected or confirmed: vancomycin (note: retrospective data show higher relapse rates with vancomycin vs. beta-lactam for MSSA, so use vancomycin only when MRSA is strongly suspected or confirmed, or in true penicillin allergy)
- Gram-negatives (open fracture, IV drug use, Pseudomonas): 3rd-generation cephalosporins, aminoglycosides, imipenem-cilastatin
Duration:
- Standard: IV antibiotics for 4-6 weeks, then transition to oral
- Shortened IV-then-oral regimens are used for uncomplicated cases in patients improving both clinically and haematologically
- Recent meta-analysis (Lima et al., 2025, PMID 40280255) comparing oral vs. IV antibiotics for bone/joint infections supports early oral switch when appropriate
Surgical Management
Acute: Surgical drainage is indicated when:
- There is no clinical improvement within 24-48 hours of antibiotics
- There is a subperiosteal or soft tissue abscess
- Pus is present on aspiration
Chronic osteomyelitis - the surgical problem:
- Debridement of all necrotic bone (sequestrectomy) and soft tissue
- Obliteration of dead space: options include local muscle flaps, antibiotic-impregnated calcium sulfate or PMMA beads (gentamicin, tobramycin), or antibiotic-loaded biodegradable implants
- Bone reconstruction if segmental defect (Ilizarov technique, vascularized bone grafts)
- Hyperbaric oxygen as an adjunct in refractory cases
10. Special Forms
Tuberculous Osteomyelitis (Pott's Disease)
- More destructive and harder to control than pyogenic osteomyelitis
- ~1-3% of pulmonary/extrapulmonary TB patients develop bone infection
- Predilection for the spine (thoracolumbar junction), then hip and knee
- Typical presentation: localized pain, low-grade fever, weight loss; months to years before diagnosis
- Radiograph: anterior vertebral body destruction, disc space loss, paraspinal "cold abscess" (no rim enhancement on CT, unlike pyogenic)
- Tuberculous dactylitis (spina ventosa): cystic cavities with diaphyseal expansion, hands > feet
Diabetic Foot Osteomyelitis
- Contiguous spread from neuropathic/ischemic ulcers
- Often polymicrobial
- Probe-to-bone test: positive predictive value >89% for osteomyelitis
- MRI is the most accurate imaging modality
Neonatal Osteomyelitis
- Often subtle - irritability, pseudoparalysis of a limb, swelling
- Metaphyseal vessels cross the growth plate, so joint and epiphyseal involvement is common
- Multifocal in ~40% of neonates; whole-body MRI or skeletal scintigraphy may be needed
- S. aureus, Group B Strep, E. coli
Recent Evidence (2024-2026)
- Risk factors (Yang et al., 2025 - PMID 40607967): Systematic review/meta-analysis confirming diabetes, peripheral vascular disease, immunosuppression, and prior surgery as major modifiable risk factors.
- Oral vs. IV antibiotics (Lima et al., 2025 - PMID 40280255): Meta-analysis of RCTs supports that oral antibiotics are non-inferior to IV for bone and joint infections when bioavailability is high, supporting early oral step-down.
- Calcaneal osteomyelitis (Jiang et al., 2024 - PMID 38869983): Systematic review of 1,118 cases highlights the need for aggressive surgical debridement in calcaneal disease given high recurrence rates.
Sources: Robbins & Cotran Pathologic Basis of Disease; Bailey and Love's Short Practice of Surgery, 28e; Rosen's Emergency Medicine; Grainger & Allison's Diagnostic Radiology; Campbell's Operative Orthopaedics, 15e (2026)
This is a shared conversation. Sign in to Orris to start your own chat.