Complete details on vasculitis
Reading File
Finding Sources
Searching PubMed
vasculitis classification management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive answer. Let me compile it.
Vasculitis - Complete Clinical Review
Definition
Vasculitis is a general term for vessel wall inflammation. The two most common pathogenic mechanisms are immune-mediated inflammation and direct vascular invasion by infectious pathogens. Physical/chemical injury (radiation, toxins, trauma) also causes vasculitis. Some 20 primary forms are recognized, classified by vessel size, immune mechanism, autoantibody profile, granuloma formation, organ specificity, and demographics.
- Robbins & Kumar Basic Pathology, p. 328
Classification by Vessel Size
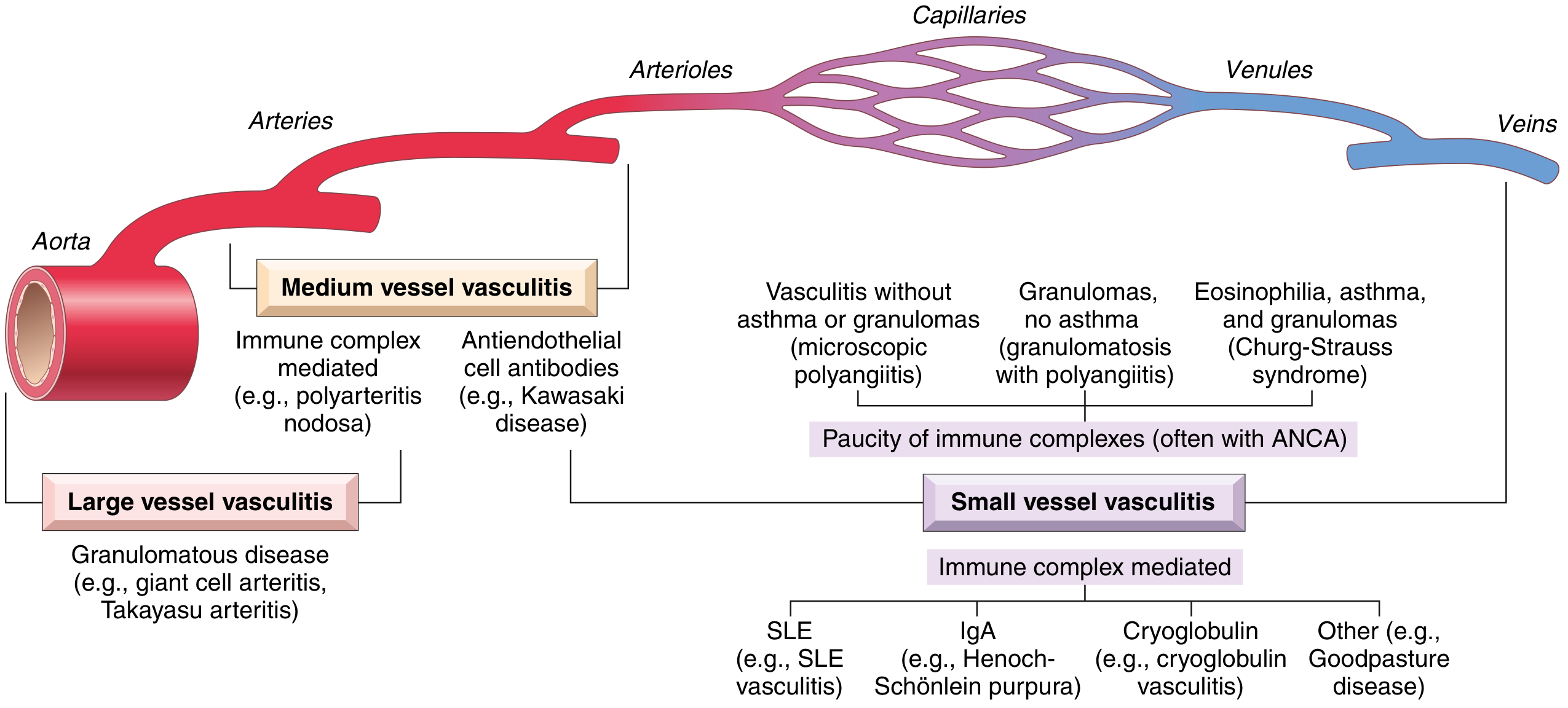
Large-Vessel Vasculitis
Predominantly affects the aorta and its major branches.
| Disease | Key Feature |
|---|---|
| Giant Cell Arteritis | Granulomatous; age >50; temporal/ophthalmic arteries |
| Takayasu Arteritis | Granulomatous; age <50; aortic arch and branches |
Medium-Vessel Vasculitis
Predominantly affects main visceral arteries and their branches; aneurysms and stenoses are common.
| Disease | Key Feature |
|---|---|
| Polyarteritis Nodosa (PAN) | Necrotizing; no ANCA; no pulmonary involvement |
| Kawasaki Disease | Anti-endothelial cell antibodies; coronary arteries; children |
Small-Vessel Vasculitis
Predominantly affects arterioles, capillaries, and venules.
ANCA-associated (pauci-immune):
| Disease | ANCA | Hallmark |
|---|---|---|
| Microscopic Polyangiitis (MPA) | MPO-ANCA | Necrotizing GN + pulmonary capillaritis; no granulomas |
| Granulomatosis with Polyangiitis (GPA / Wegener) | PR3-ANCA (95%) | Upper + lower airway granulomas + GN |
| Eosinophilic GPA (EGPA / Churg-Strauss) | MPO-ANCA (>50%) | Asthma + eosinophilia + granulomatous inflammation |
Immune complex-mediated:
| Disease | Immune Complex |
|---|---|
| IgA Vasculitis (HSP) | IgA deposits |
| Cryoglobulinemic Vasculitis | Cryoglobulin complexes |
| SLE Vasculitis | Nuclear antigen complexes |
| Anti-GBM Disease (Goodpasture) | Anti-GBM antibody |
Pathogenesis
1. Immune Complex Deposition
Immune complexes deposit in vessel walls, activate complement, and recruit neutrophils. Seen in drug hypersensitivity vasculitis (e.g., penicillin), SLE, and HBsAg-associated PAN (up to 30% of PAN cases).
2. ANCA-Associated Mechanisms
ANCAs are autoantibodies directed against neutrophil cytoplasmic antigens. Two main types:
- PR3-ANCA (c-ANCA): Neutrophil azurophilic granule constituent; shares homology with microbial peptides
- MPO-ANCA (p-ANCA): Myeloperoxidase
Pathogenic sequence:
- Drugs or cross-reactive microbial antigens induce ANCA formation
- Inflammatory stimuli (e.g., TNF) upregulate surface expression of PR3/MPO on neutrophils
- ANCAs bind these cytokine-activated cells, causing further neutrophil activation
- ANCA-activated neutrophils release granule contents and reactive oxygen species, injuring endothelial cells
- Lesions are "pauci-immune" - no circulating immune complexes, no antibody/complement in vessel walls
ANCA titers generally mirror clinical severity; a rise after quiescence predicts relapse.
3. Anti-Endothelial Cell Antibodies
Underlie Kawasaki disease.
4. Autoreactive T Cells
Cause granulomatous vasculitis (GCA, Takayasu). Both Th1 (IFN-γ) and Th17 (IL-17) pathways are involved in GCA.
- Robbins & Kumar Basic Pathology, pp. 328-332
Individual Vasculitis Entities
Giant Cell (Temporal) Arteritis
The most common vasculitis in the United States.
Vessels affected: Temporal arteries, ophthalmic arteries, vertebral arteries, aorta.
Risk factors: Age >50, North European descent; strong MHC class II HLA association.
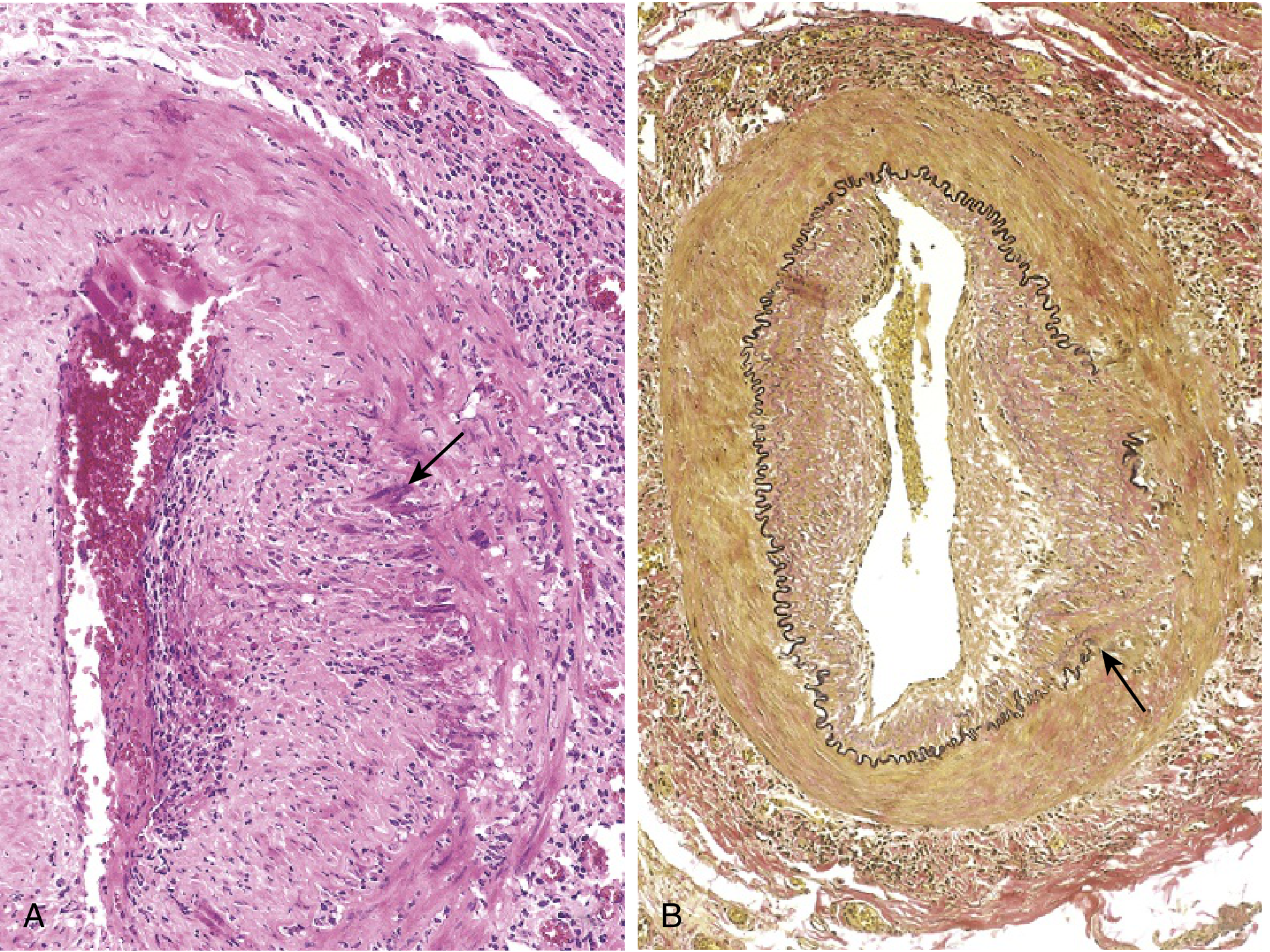
Morphology:
- Patchy granulomatous inflammation of the inner media
- T lymphocytes and macrophages with multinucleate giant cells
- Fragmentation of the internal elastic lamina
- Nodular intimal thickening reducing lumen diameter
- In 25% of cases: non-specific panarteritis without giant cells
Clinical features:
- Fever, fatigue, weight loss
- Facial pain/headache along the temporal artery; tender to palpation
- Ocular symptoms in ~50% (ophthalmic artery involvement) - diplopia to complete vision loss (an ophthalmologic emergency)
- ESR markedly elevated
- Often associated with polymyalgia rheumatica
Diagnosis: Temporal artery biopsy (negative biopsy does not exclude - inflammation is patchy)
Treatment: Corticosteroids (mainstay). Anti-IL-6 receptor therapy (tocilizumab) for steroid-resistant cases; recent evidence supports tocilizumab for glucocorticoid-sparing.
Takayasu Arteritis ("Pulseless Disease")
Vessels: Aorta, aortic arch branches (carotid, subclavian, renal arteries), pulmonary artery.
Demographics: Age <50; young Asian women predominantly.
Morphology: Granulomatous inflammation of the aorta and its main branches; irregular thickening of the aortic wall, intimal wrinkling; "tree-bark" aorta. Lesions histologically resemble GCA.
Clinical features:
- Ocular disturbances (visual field defects, retinal hemorrhage)
- Absent/asymmetric pulses in upper extremities - "pulseless disease"
- Neurologic deficits (syncope, strokes)
- Hypertension (renovascular involvement)
- Pulmonary hypertension
- Systemic inflammation (fever, arthritis, myalgia)
- Pooled prevalence of stroke: 8.9% per meta-analysis
Treatment: Corticosteroids; methotrexate, azathioprine, or biologics as steroid-sparing agents. Vascular surgery/stenting for critical stenoses.
Polyarteritis Nodosa (PAN)
Vessels: Medium and small arteries - spares pulmonary circulation, glomeruli, arterioles, capillaries, and venules (key distinguishing feature from MPA).
Associations: Hepatitis B (HBsAg immune complexes in ~30% of cases). No ANCA.
Morphology:
- Segmental transmural necrotizing inflammation
- Lesions at different stages of development in same patient (unlike MPA)
- Inflammatory aneurysms; thrombosis; infarction of supplied organs
- Healing with fibrous scarring
Clinical features:
- Multisystem disease: kidney (hypertension, hematuria), heart, liver, peripheral nervous system (mononeuritis multiplex)
- GI tract involvement - mesenteric arteritis causing pain/bleeding
- Skin: livedo reticularis, nodules, ulcers, digital infarcts
Treatment: Corticosteroids + cyclophosphamide for severe cases; antiviral therapy (interferon + antivirals) for HBV-associated PAN.
Kawasaki Disease
Demographics: Infants and young children; Asian descent; most common under 5 years.
Pathogenesis: Anti-endothelial cell antibodies. Likely triggered by an uncharacterized infectious agent.
Morphology: Necrotizing arteritis affecting coronary arteries in 80% of symptomatic cases; coronary artery aneurysms (risk of thrombosis and rupture).
Clinical features (mucocutaneous lymph node syndrome):
- Fever >5 days (required)
- Bilateral conjunctival injection (non-purulent)
- Oral changes: strawberry tongue, red cracked lips, pharyngeal erythema
- Rash (polymorphous)
- Extremity changes: erythema/edema of hands/feet, periungual desquamation
- Cervical lymphadenopathy
- Coronary aneurysms in untreated cases - most important complication
Treatment: IV immunoglobulin (IVIG) + aspirin (dramatically reduces coronary aneurysm risk). Infliximab for refractory cases.
Granulomatosis with Polyangiitis (GPA / Wegener)
Vessels: Small to medium vessels; upper and lower respiratory tract + kidneys.
Antibody: PR3-ANCA present in ~95% of cases.
Classic triad:
- Necrotizing granulomas of the upper respiratory tract (sinusitis, nasal septal perforation, "saddle-nose" deformity)
- Necrotizing vasculitis of pulmonary vessels
- Focal necrotizing glomerulonephritis (crescentic GN)

Clinical features:
- Chronic sinusitis, epistaxis, nasal/oral ulcers
- Hemoptysis, dyspnea
- Hematuria, proteinuria (renal failure if untreated)
- Constitutional symptoms
- c-ANCA/PR3-ANCA is the key diagnostic marker
Treatment: Rituximab or cyclophosphamide + glucocorticoids for remission induction. Rituximab or azathioprine/methotrexate for maintenance. Close monitoring mandatory.
Microscopic Polyangiitis (MPA)
Vessels: Capillaries, arterioles, venules (and small arteries) - the smallest vessels.
Antibody: MPO-ANCA (most cases). Pauci-immune (no immune complexes).
Distinguishes from PAN: Affects capillaries/venules; all lesions are the same age; involves pulmonary capillaries and glomeruli (PAN does not).
Morphology: Segmental fibrinoid necrosis; focal transmural necrotizing lesions; leukocytoclastic vasculitis (neutrophil karyorrhexis in postcapillary venules); no granulomas.
Clinical features:
- Palpable purpura (skin, most common)
- Necrotizing GN (90% of patients) - hematuria, proteinuria
- Pulmonary capillaritis - hemoptysis, diffuse alveolar hemorrhage
- Abdominal pain/bleeding; muscle pain; weakness
Treatment: Corticosteroids + cyclophosphamide or rituximab. Remission maintenance with azathioprine/rituximab.
Eosinophilic Granulomatosis with Polyangiitis (EGPA / Churg-Strauss)
Vessels: Small to medium vessels; respiratory tract.
Classic triad: Asthma + eosinophilia + granulomatous vasculitis.
Antibody: MPO-ANCA in >50% (ANCA more frequent when glomerulonephritis is present).
Clinical features:
- Long history of adult-onset asthma
- Peripheral eosinophilia (>10% on differential)
- Mononeuritis multiplex
- Skin lesions; cardiac involvement (eosinophilic myocarditis - major cause of death)
- GN (less common than GPA or MPA)
Treatment: High-dose glucocorticoids; cyclophosphamide for severe/refractory disease. Mepolizumab (anti-IL-5) approved for steroid-sparing in EGPA.
IgA Vasculitis (Henoch-Schönlein Purpura / HSP)
Vessels: Small vessels (IgA immune complex deposits in vessel walls).
Most common systemic vasculitis in children. Often follows a respiratory infection.
Classic tetrad:
- Palpable purpura (lower extremities/buttocks) - non-thrombocytopenic
- Arthralgia/arthritis
- Colicky abdominal pain (GI vasculitis)
- Renal involvement (IgA nephropathy pattern - hematuria/proteinuria)
Pathology: IgA and C3 deposits in small vessel walls on immunofluorescence (identical pattern to IgA nephropathy in the kidney).
Treatment: Mostly self-limiting in children. Supportive care. Corticosteroids for severe GI/renal involvement.
Behçet Disease
Vessels: Any size - veins as well as arteries (one of few vasculitides to prominently involve veins).
Pathogenesis: Strongly associated with HLA-B51. T-cell-mediated with neutrophil hyperactivation.
Clinical features (classic triad):
- Recurrent oral aphthous ulcers (virtually universal)
- Genital ulcers
- Uveitis (may lead to blindness)
Additional features: skin lesions (erythema nodosum, pseudofolliculitis), venous thrombosis, CNS involvement, arthritis.
Pathergy test: Nonspecific skin hyperreactivity to needle prick.
Treatment: Colchicine, azathioprine, cyclosporine, anti-TNF agents for refractory disease.
Shared Clinical Manifestations
Regardless of specific type, vasculitis commonly presents with:
- Constitutional: Fever, malaise, myalgia, arthralgia, weight loss
- Skin: Palpable purpura, livedo reticularis, ulcers, digital infarcts
- Renal: Hematuria, proteinuria, progressive renal failure (glomerulonephritis)
- Neurologic: Mononeuritis multiplex, headache, stroke
- Pulmonary: Hemoptysis, diffuse alveolar hemorrhage, nodules
- GI: Abdominal pain, GI bleeding, bowel infarction
Diagnosis
Laboratory
| Test | Utility |
|---|---|
| ANCA (PR3/MPO) | GPA (PR3), MPA/EGPA (MPO) |
| ESR / CRP | Disease activity marker (markedly elevated in GCA) |
| CBC | Eosinophilia (EGPA), anemia of inflammation |
| Urinalysis | RBC casts, proteinuria (renal vasculitis) |
| Serum creatinine | Renal function |
| HBsAg / HCV antibody | PAN, cryoglobulinemic vasculitis |
| ANA, anti-dsDNA | SLE-associated vasculitis |
| Complement (C3, C4, CH50) | Low in immune-complex vasculitis |
| Cryoglobulins | Cryoglobulinemic vasculitis |
| IgA levels | IgA vasculitis |
Imaging
- Angiography (DSA): Gold standard for medium/large vessel vasculitis; shows stenoses, occlusions, aneurysms. Angiography can be negative in small vessel CNS vasculitis.
- MRA/CTA: Useful for large vessel disease; inferior to DSA for small peripheral vessels
- High-resolution MRI vessel wall imaging: Circumferential vessel wall enhancement in CNS vasculitis
- PET-CT: Inflammatory activity in large vessel vasculitis (GCA, Takayasu)
- CXR/CT chest: Nodules, cavities, diffuse alveolar hemorrhage (GPA, MPA, EGPA)
Biopsy
- Temporal artery biopsy: GCA (skip lesions mean negative biopsy does not exclude)
- Renal biopsy: Necrotizing GN with pauci-immune pattern (ANCA vasculitis)
- Skin biopsy: Leukocytoclastic vasculitis; IgA staining (HSP)
- Brain/meningeal biopsy: Often necessary for primary CNS vasculitis (angiography frequently negative)
- Nasal/sinus biopsy: GPA
Treatment Overview
General Principles
Treatment is guided by disease type, severity, and organ involvement:
- Severe: CNS, cardiac, renal, peripheral nerve - aggressive immunosuppression
- Not severe: Skin/musculoskeletal - may use glucocorticoids alone or watchful waiting
- Always exclude infectious vasculitis before starting immunosuppression
- "Watchful waiting" is appropriate when diagnosis is uncertain, etiology is reversible (drug/toxin), or disease is self-limited
A common error is treating patients too long with high-dose immunosuppressive agents.
Remission Induction
| Drug | Use |
|---|---|
| High-dose glucocorticoids | All severe vasculitis (first-line) |
| Cyclophosphamide | GPA, MPA, EGPA, PAN (severe) |
| Rituximab | GPA, MPA (non-inferior to cyclophosphamide; preferred when fertility preservation matters) |
| IVIG + aspirin | Kawasaki disease |
Remission Maintenance
| Drug | Use |
|---|---|
| Azathioprine | GPA, MPA, EGPA |
| Methotrexate | GPA (mild-moderate) |
| Mycophenolate mofetil (MMF) | Alternative to azathioprine |
| Rituximab | GPA, MPA maintenance |
| Low-dose prednisone | GCA, Takayasu |
Biologic Agents
| Agent | Use |
|---|---|
| Tocilizumab (IL-6R inhibitor) | GCA (glucocorticoid-sparing), Takayasu |
| Mepolizumab (anti-IL-5) | EGPA (eosinophil-targeted) |
| Infliximab (anti-TNF) | Refractory Kawasaki, Behçet |
Monitoring
Vasculitis has high relapse rates. Regular clinical, laboratory, and radiographic monitoring is mandatory - not just at disease onset, but for years after diagnosis. ANCA titers correlate with disease activity; a rising titer predicts relapse.
Infection Prophylaxis
Pneumocystis jiroveci pneumonia (PJP) prophylaxis is required for patients on cyclophosphamide + glucocorticoid regimens.
Cardiovascular Risk
Vasculitis carries significantly increased cardiovascular risk:
-
ANCA-associated vasculitis: 3-fold increased CVD risk; 8-fold increased cerebrovascular event risk
-
GCA / Takayasu: Increased stroke and cardiovascular mortality; meta-analysis shows pooled stroke prevalence of 8.9% in Takayasu
-
Platelet inhibitor use should follow general population guidelines (aspirin for secondary, not primary, CVD prevention)
-
Firestein & Kelley's Textbook of Rheumatology; Robbins & Kumar Basic Pathology, pp. 328-336; Fitzpatrick's Dermatology, p. 2586; Murray & Nadel's Respiratory Medicine
Quick Reference Summary Table
| Vasculitis | Vessel Size | Key Ab/Marker | Classic Feature | Treatment |
|---|---|---|---|---|
| Giant Cell Arteritis | Large | ESR↑, IL-6↑ | Age >50, temporal HA, blindness | Steroids ± tocilizumab |
| Takayasu | Large | ESR↑ | Age <50, pulseless, Asian women | Steroids ± methotrexate |
| PAN | Medium | HBsAg (30%) | No lung, no ANCA, renal/gut infarcts | Steroids ± CYC; antivirals if HBV |
| Kawasaki | Medium | Anti-EC Ab | Children, coronary aneurysms | IVIG + aspirin |
| GPA (Wegener) | Small-Med | PR3-ANCA (95%) | Sinusitis + hemoptysis + GN | Steroids + rituximab/CYC |
| MPA | Small | MPO-ANCA | GN (90%) + pulm capillaritis | Steroids + rituximab/CYC |
| EGPA (Churg-Strauss) | Small-Med | MPO-ANCA (>50%) | Asthma + eosinophilia | Steroids ± mepolizumab |
| IgA Vasculitis (HSP) | Small | IgA deposits | Children: purpura + arthritis + GI | Supportive; steroids if severe |
| Behçet | Variable | HLA-B51 | Oral + genital ulcers + uveitis | Colchicine, azathioprine, anti-TNF |
| Cryoglobulinemic | Small | Cryoglobulins, HCV | Purpura + GN + peripheral neuropathy | Treat HCV; steroids; rituximab |
This is a shared conversation. Sign in to Orris to start your own chat.