1. Define erythropoiesis. Explain the stages of erythropoiesis. Detail about regulation of erythropoiesis. Add a note on Iron deficiency anemia.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the content and images needed to compose a thorough, well-structured answer. Here it is:
Erythropoiesis: Definition, Stages, Regulation, and Iron Deficiency Anemia
1. Definition of Erythropoiesis
Erythropoiesis is the process by which mature red blood cells (erythrocytes) are produced from pluripotent hematopoietic stem cells in the red bone marrow. It is a continuous, tightly regulated process that generates approximately 2 million erythrocytes per second in a healthy adult to maintain the oxygen-carrying capacity of blood. The entire process - from stem cell to circulating red cell - takes about 7 days. Erythrocytes have a lifespan of approximately 120 days in the circulation.
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology
- Basic Medical Biochemistry - A Clinical Approach, 6e
2. Stages of Erythropoiesis
Erythropoiesis proceeds through a well-defined sequence of morphologically recognizable stages. The lineage originates from the Hematopoietic Stem Cell (HSC), then passes through committed progenitors before yielding the first microscopically visible precursor.
Progenitor (Non-morphological) Stages
| Stage | Features |
|---|---|
| HSC | Self-renewing pluripotent stem cell |
| Common Myeloid Progenitor (CMP / CFU-GEMM) | Colony-forming unit for granulocyte, erythroid, monocyte, megakaryocyte |
| Megakaryocyte-Erythroid Progenitor (MEP / BFU-EMeg) | Bipotent; commits to either erythroid or megakaryocyte lineage |
| Burst-Forming Unit - Erythroid (BFU-E) | Large colonies; relatively insensitive to EPO; responsive to IL-3, IL-4, SCF |
| Colony-Forming Unit - Erythroid (CFU-E) | Highly sensitive to erythropoietin (EPO); final committed progenitor; small colonies |
Under the influence of the transcription factor GATA-1, MEP cells transform into erythropoietin-sensitive erythrocyte-committed progenitors (ErPs), which give rise to the first recognizable cell - the proerythroblast.
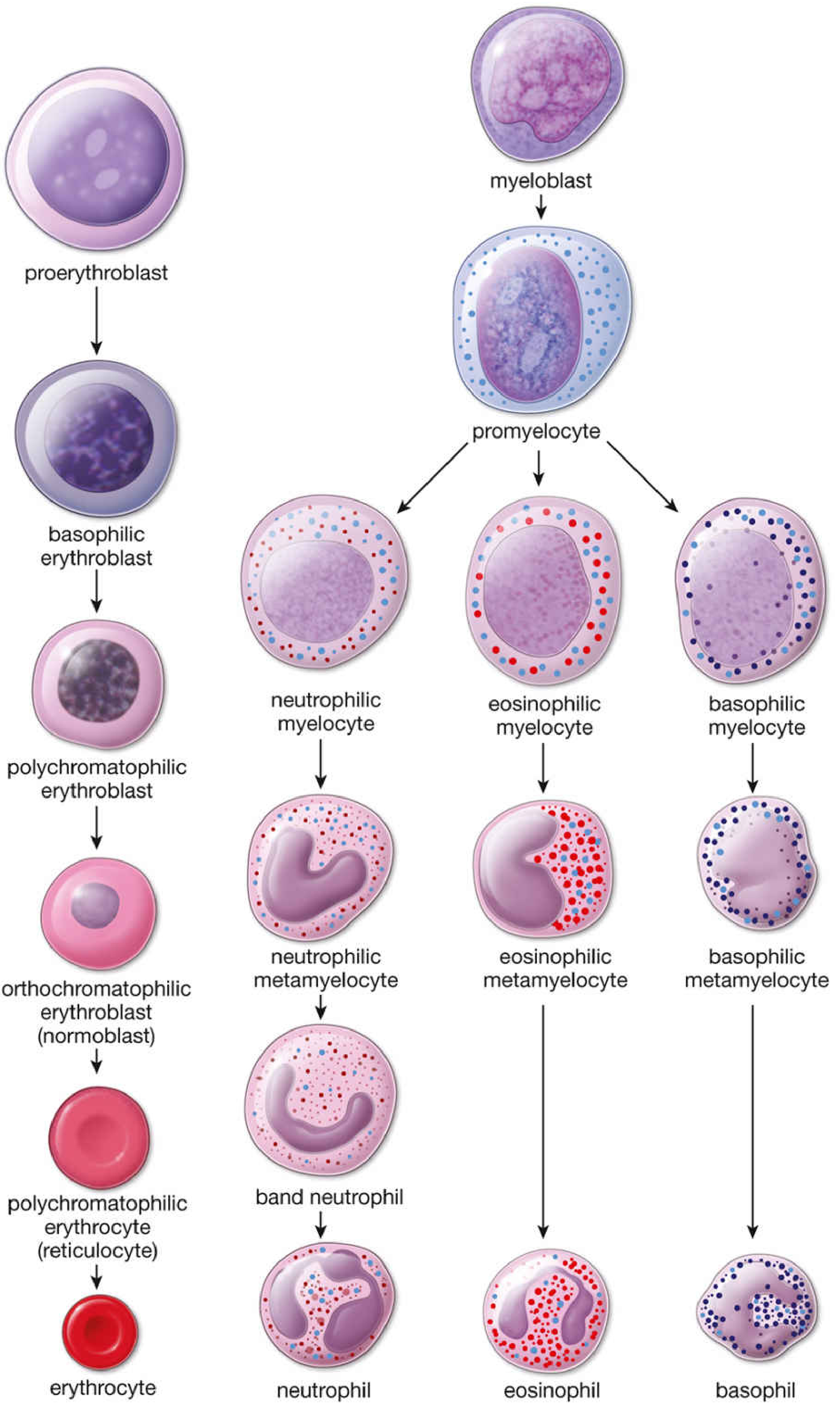
Stages of erythrocytic differentiation - Histology: A Text and Atlas
Morphological (Recognizable) Stages
The following diagram shows how RNA decreases and hemoglobin increases across maturation:
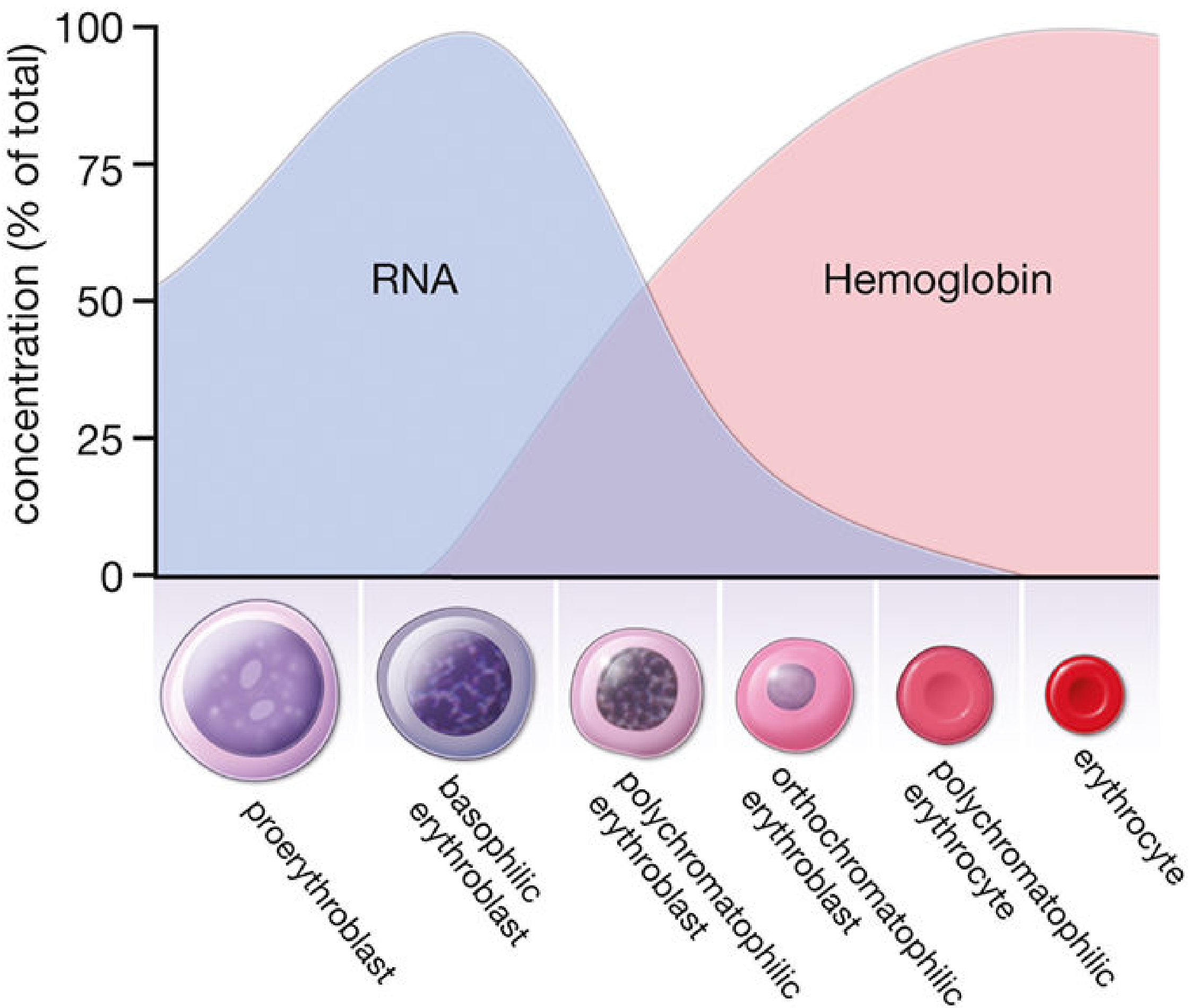
RNA vs. Hemoglobin concentration across erythropoiesis stages - Histology: A Text and Atlas
Stage 1 - Proerythroblast (Pronormoblast)
- Size: 12-20 µm (largest precursor)
- Nucleus: Large, round, with 1-2 prominent nucleoli; fine euchromatin
- Cytoplasm: Mildly basophilic (free ribosomes beginning to accumulate)
- Activity: Components for hemoglobin (Hgb) synthesis begin to accumulate
- Duration: ~24 hours
- Mitosis: Present (capable of division)
Stage 2 - Basophilic Erythroblast (Early Normoblast)
- Size: Smaller than proerythroblast; 10-16 µm
- Nucleus: Smaller, progressively more heterochromatic; nucleoli becoming less visible
- Cytoplasm: Strongly basophilic due to abundant free polyribosomes actively synthesizing Hgb
- Duration: ~24 hours
- Mitosis: Present
Stage 3 - Polychromatophilic Erythroblast (Intermediate Normoblast)
- Size: Continues to decrease
- Nucleus: Smaller still; coarse heterochromatin in a "checkerboard" pattern
- Cytoplasm: Both basophilic AND acidophilic (gray-lilac color): basophilia from RNA/ribosomes + eosinophilia from accumulating Hgb; the cytoplasm may show distinct pink and purple regions
- Duration: ~30 hours
- Mitosis: This is the LAST stage capable of mitotic division
Stage 4 - Orthochromatophilic Erythroblast (Late Normoblast)
- Size: Only slightly larger than a mature RBC (~7.8 µm)
- Nucleus: Small, compact, densely pyknotic; no visible chromatin pattern; eventually extruded
- Cytoplasm: Predominantly eosinophilic (pink) due to large amounts of Hgb
- Duration: ~48 hours
- Mitosis: No longer capable of division
- Key event: Nuclear extrusion occurs at this stage. Residual nuclear fragments = Howell-Jolly bodies
Stage 5 - Polychromatophilic Erythrocyte (Reticulocyte)
- Nucleus: Absent (extruded)
- Cytoplasm: Slight basophilia from residual polyribosomes + eosinophilia from Hgb (hence "polychromatophilic")
- Activity: Still capable of synthesizing Hgb from retained ribosomes and mRNA
- With supravital stains (brilliant cresyl blue / new methylene blue): residual RNA precipitates as a reticulum (network), hence the name reticulocyte
- Circulation: Released from bone marrow into blood; circulates for 1-2 days; matures in the spleen where ribosomes and mRNA are lost
- Normal count: 0.5-1.5% of circulating RBCs
Stage 6 - Mature Erythrocyte (Normocyte)
- Size: 7.2-7.8 µm; biconcave disc
- Nucleus: Absent
- Cytoplasm: Uniformly eosinophilic; central pallor = 1/3 of cell diameter
- Lifespan: ~120 days
- Fate: Senescent RBCs phagocytosed by macrophages in spleen, liver, and bone marrow; heme recycled; iron stored as ferritin/hemosiderin for reuse
Memory summary: Proerythroblast → Basophilic erythroblast → Polychromatophilic erythroblast → Orthochromatophilic erythroblast → Reticulocyte → Erythrocyte
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology
3. Regulation of Erythropoiesis
Erythropoiesis is regulated at multiple levels - primarily by oxygen tension (through erythropoietin), by specific growth factors and cytokines, and by the transcription factor GATA-1.
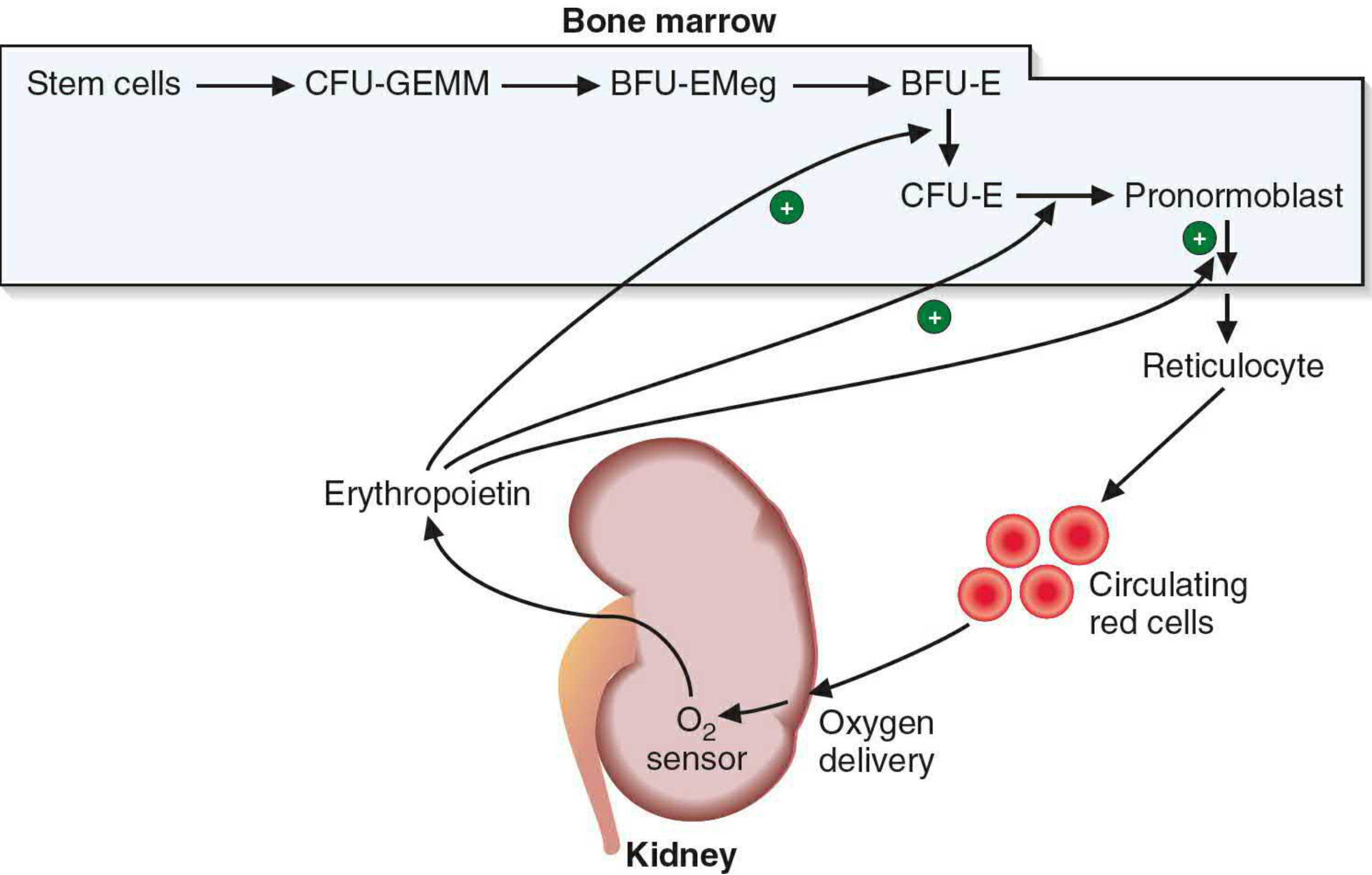
Erythropoietin feedback loop - Basic Medical Biochemistry, 6e
A. Erythropoietin (EPO) - The Master Regulator
- Source: 90% produced by peritubular interstitial cells (fibroblast-like cells) of the renal cortex; 10% by hepatocytes
- Stimulus: Decreased tissue oxygen delivery (hypoxia, anemia, high altitude, cardiopulmonary disease)
- Molecular weight: 34 kDa glycoprotein hormone
- Mechanism:
- Hypoxia activates Hypoxia-Inducible Factor-1 (HIF-1), which transcriptionally upregulates the EPO gene
- EPO binds to specific receptors on CFU-E and early erythroblasts
- Receptor activation triggers JAK2/STAT5 signaling, promoting:
- Proliferation of erythroid progenitors
- Survival (anti-apoptotic signaling)
- Differentiation and maturation
- Feedback: Increased RBC mass restores oxygen delivery → EPO production falls
- Clinical relevance: Recombinant EPO (epoetin alfa) is used in anemia of chronic kidney disease, cancer chemotherapy-induced anemia
B. Growth Factors and Cytokines
| Factor | Action | Stage targeted |
|---|---|---|
| Stem Cell Factor (SCF / c-Kit ligand) | Early erythroid commitment | HSC, CMP |
| IL-3 | Proliferation of early progenitors | BFU-E |
| IL-4 | Supports erythroid differentiation | MEP → ErP |
| GM-CSF | Supports CMP differentiation | CMP |
| EPO | Terminal differentiation, survival | CFU-E, erythroblasts |
C. GATA-1 Transcription Factor
- GATA-1 is a zinc-finger transcription factor that is essential for terminal erythroid differentiation
- It drives expression of erythroid-specific genes (globin chains, heme synthesis enzymes, transferrin receptor)
- Loss of GATA-1 causes developmental arrest at the MEP stage with apoptosis of erythroid precursors
D. Kinetics and Negative Regulation
- Mitoses occur in proerythroblasts, basophilic erythroblasts, and polychromatophilic erythroblasts (3 stages)
- Each erythroblast undergoes approximately 4 cell cycles, amplifying one proerythroblast into ~16 orthochromatophilic erythroblasts
- Bone marrow is NOT a storage site for erythrocytes - cells are released as soon as formed
- Negative regulators: Activin, TGF-β, and high EPO feedback inhibit excess production
E. Iron and Substrate Availability
-
Adequate iron supply is mandatory for Hgb synthesis; iron deficiency shifts erythropoiesis toward ineffective production
-
Vitamin B12 and folate are required for DNA synthesis in dividing erythroblasts; their deficiency causes megaloblastic anemia
-
Basic Medical Biochemistry, 6e; Histology: A Text and Atlas
4. Iron Deficiency Anemia (IDA)
Iron Metabolism - Background
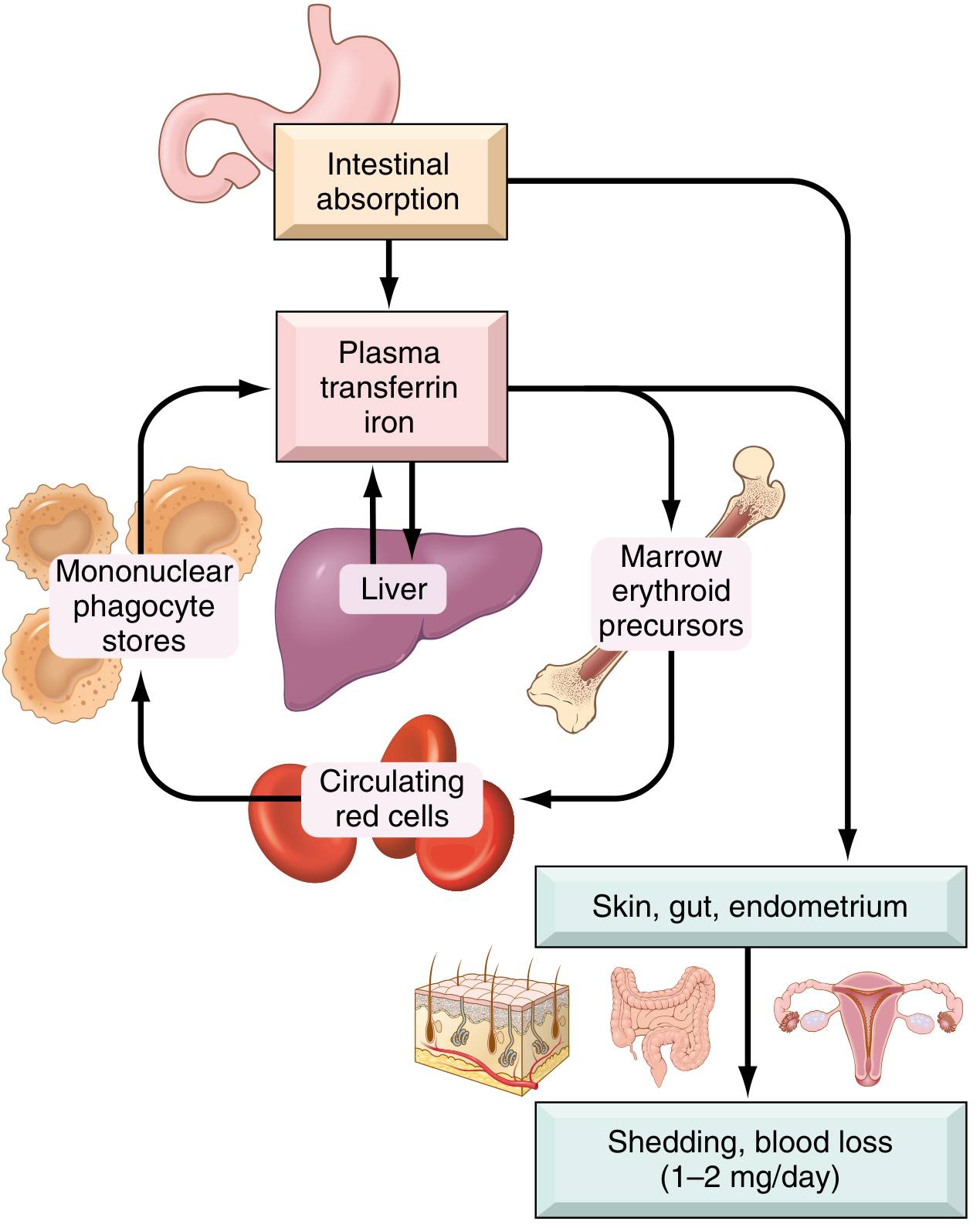
Normal iron metabolism - Robbins, Cotran & Kumar Pathologic Basis of Disease
Total body iron: ~3,450 mg (males), ~2,450 mg (females). The majority is in the functional compartment as hemoglobin iron; the remainder is stored as ferritin and hemosiderin, primarily in hepatocytes and macrophages of the spleen and bone marrow.
Hepcidin is the master regulator of iron absorption and distribution:
- A peptide hormone synthesized by hepatocytes
- Binds ferroportin on enterocytes and macrophages → causes its endocytosis and degradation
- When iron stores are high or inflammation is present: hepcidin rises → iron is trapped in enterocytes and macrophages → reduced iron delivery to erythroid precursors
- When iron stores are low: hepcidin falls → ferroportin expression increases → more iron absorbed from gut and released from macrophage stores
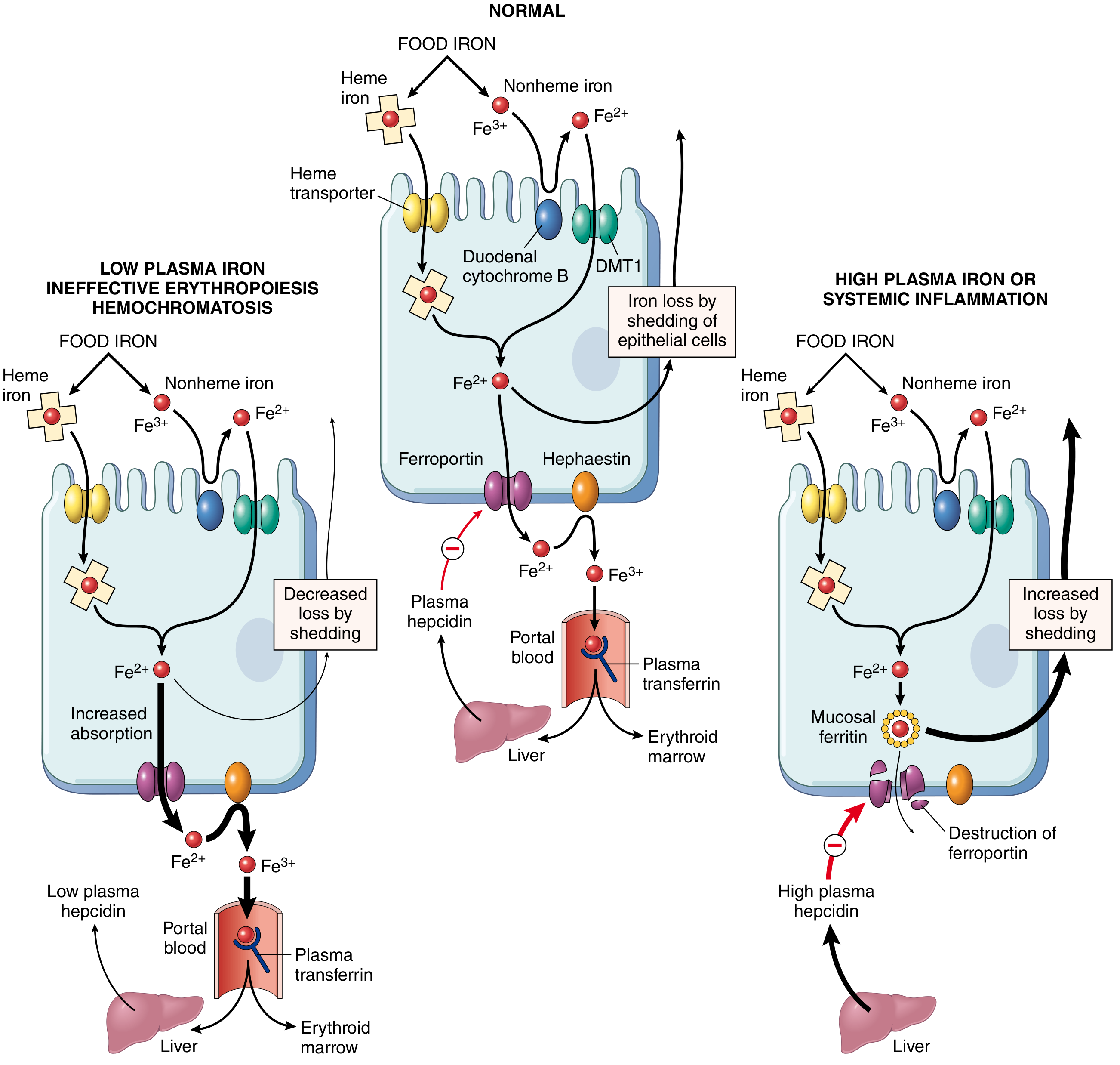
Hepcidin-ferroportin axis regulating iron absorption - Robbins, Cotran & Kumar Pathologic Basis of Disease
Definition
Iron deficiency anemia is a hypochromic microcytic anemia resulting from inadequate iron supply for hemoglobin synthesis, leading to reduced mean corpuscular volume (MCV) and mean corpuscular hemoglobin (MCH). It is the most common nutritional disorder in the world.
Etiology and Pathogenesis
Iron deficiency arises from one or more of four mechanisms:
1. Dietary lack
- Most common in low-resource countries (plant-based diet with inorganic/non-heme iron)
- High-risk groups in wealthy nations: infants (breast milk ~0.3 mg/L), vegans, elderly with poor dentition/income
2. Impaired absorption
- Celiac disease, sprue, atrophic gastritis
- Gastrectomy (reduces acidity needed for Fe³⁺ → Fe²⁺ reduction; accelerates gastric transit)
- Dietary inhibitors: tannins (tea), carbonates, oxalates, phosphates
3. Increased requirement
- Rapidly growing infants and adolescents
- Pregnancy (fetal demands + blood volume expansion)
- Premenopausal females
4. Chronic blood loss (most common cause in developed countries)
- Gastrointestinal: peptic ulcer, colorectal cancer, hookworm infestation, NSAID-induced gastropathy
- Gynecologic: menorrhagia
- Key clinical point: Iron deficiency in an adult male or postmenopausal female in a high-income country must be attributed to GI blood loss until proven otherwise - failing to do so risks missing an occult gastrointestinal malignancy
Stages of Iron Depletion
Iron deficiency progresses through three stages before overt anemia appears:
| Stage | Iron Stores | Serum Iron / TIBC | Hemoglobin |
|---|---|---|---|
| Stage 1 - Storage depletion | Ferritin ↓, bone marrow iron absent | Normal | Normal |
| Stage 2 - Transport depletion | Absent stores | Serum Fe ↓, TIBC ↑ | Normal (early) |
| Stage 3 - Functional deficiency | Absent | Serum Fe ↓↓, TIBC ↑↑, Transferrin sat. <15% | Hgb ↓ (overt anemia) |
Morphology
Bone marrow:
- Mild to moderate increase in erythroid progenitors (reactive erythroid hyperplasia)
- Diagnostically significant: Absent stainable iron in macrophages on Prussian blue stain (the most specific bone marrow finding)
Peripheral blood smear:

IDA blood smear: hypochromic microcytic cells with widened central pallor and pencil cells - Robbins, Cotran & Kumar Pathologic Basis of Disease
- Microcytosis: MCV < 80 fL
- Hypochromia: Enlarged zone of central pallor (>1/3 diameter); Hgb visible only as a narrow peripheral rim
- Poikilocytosis: "Pencil cells" (elongated, narrow red cells) are characteristic
- Anisocytosis (variable cell size)
Clinical Features
Symptoms of anemia:
- Fatigue, weakness, pallor, dyspnea on exertion, palpitations, headache
Features specific to iron deficiency (from tissue enzyme depletion - cytochromes, catalase):
- Koilonychia (spoon-shaped nails)
- Alopecia
- Atrophic glossitis (smooth, sore tongue)
- Atrophic gastritis with reduced gastric acid
- Pica: craving for non-food items (clay, soil) or unusual food (ice = pagophagia, flour)
- Plummer-Vinson syndrome: triad of microcytic hypochromic anemia + dysphagia from esophageal webs + atrophic glossitis (rare)
- In children: neurological effects from iron depletion in CNS (irritability, poor concentration)
Laboratory Diagnosis
| Test | Result in IDA |
|---|---|
| Hemoglobin / Hematocrit | Decreased |
| MCV | < 80 fL (microcytic) |
| MCH | Decreased (hypochromic) |
| Serum iron | Low (< 60 µg/dL) |
| TIBC (transferrin) | Elevated |
| Transferrin saturation | < 15% |
| Serum ferritin | Low (< 12 µg/L) - best single test for IDA |
| Serum hepcidin | Low (iron deficiency suppresses hepcidin) |
| Reticulocyte count | Low or normal (inadequate response) |
| Peripheral smear | Microcytic, hypochromic, pencil cells |
| Bone marrow iron (Prussian blue) | Absent (gold standard) |
Treatment
- Identify and treat the underlying cause (e.g., GI bleed)
- Oral iron: Ferrous sulfate 325 mg (65 mg elemental iron) three times daily
- Reticulocyte response within 5-7 days
- Hemoglobin normalizes in 6-8 weeks
- Continue for 3-6 months to replenish stores
- IV iron: For malabsorption, intolerance to oral iron, or rapid repletion needed (e.g., pre-surgery, severe anemia in pregnancy)
- Dietary advice: Increase heme iron (meat), supplement with vitamin C (enhances non-heme iron absorption), avoid tea with meals
Sources cited:
- Robbins, Cotran & Kumar Pathologic Basis of Disease (9780443264528)
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology (9781975181512)
- Basic Medical Biochemistry - A Clinical Approach, 6e (9781975150143)
This is a shared conversation. Sign in to Orris to start your own chat.