CARCINOMA OF CERVIX , ca endometrium ,ovarian tumor answer in detail covering imp points as welll in exaam point of view 2mbbs pathology refer robbin harsh moham add diagrams as well cover required points for muhs exam Add histo pathology diagram and gross as well for exam easy to draw diagram cover all points of important topic frequently ask and make easy to draw diagrams for muhs
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Here are your complete, detailed MUHS 2nd MBBS Pathology exam notes on all three topics, with real textbook histopathology images and easy-to-draw diagram descriptions. (Sources: Robbins & Kumar Basic Pathology, Robbins Cotran & Kumar Pathologic Basis of Disease)
🔴 CARCINOMA OF THE CERVIX
(MUHS Favourite - Frequently Asked)
1. DEFINITION & INCIDENCE
- Most common gynecological malignancy in India (2nd worldwide after breast cancer)
- Peak age: 45-55 years (squamous); adenocarcinoma slightly older
- Precedes by 10-15 years of precancerous SIL (squamous intraepithelial lesion)
2. ETIOLOGY & RISK FACTORS
| Risk Factor | Details |
|---|---|
| HPV infection | Most important; HPV 16 & 18 account for ~70% of cases |
| Early age at first coitus | Before 18 years |
| Multiple sexual partners | Patient or partner |
| High parity | Repeated cervical trauma |
| Smoking | Cocarcinogen |
| Immunosuppression | HIV, transplant patients |
| OCP use | Slight risk |
MUHS Key Point: HPV 16 = SCC; HPV 18 = Adenocarcinoma (remember "18 = 8 letters = Adeno")
3. PATHOGENESIS
Step 1: HPV Infection
- HPV is a DNA virus that infects immature squamous cells at the transformation zone (junction of squamous and columnar epithelium at ectocervix/endocervix)
Step 2: Oncogenic Mechanism - Two key proteins
┌─────────────────────────────────────────────┐
│ HPV Oncoproteins │
├──────────────┬──────────────────────────────┤
│ E6 protein │ Binds & destroys p53 │
│ │ → blocks apoptosis │
│ │ → activates telomerase │
├──────────────┼──────────────────────────────┤
│ E7 protein │ Binds RB protein │
│ │ → releases E2F │
│ │ → uncontrolled cell cycle │
└──────────────┴──────────────────────────────┘
Step 3: Progression
- Low-risk HPV (6, 11): remain episomal - cause condylomas only
- High-risk HPV (16, 18): integrate into host genome - disrupts E2 gene (which normally suppresses E6/E7) → overexpression of E6/E7 → malignant transformation
4. PRECANCEROUS LESIONS - SIL / CIN
Two-tier system (clinical management):
- LSIL = Low-grade SIL = CIN I
- HSIL = High-grade SIL = CIN II + CIN III
Natural History (must memorize for MUHS):
| Lesion | Regress | Persist | Progress |
|---|---|---|---|
| LSIL (CIN I) | 60% | 30% | 10% → HSIL |
| HSIL (CIN II/III) | 30% | 60% | 10% → Carcinoma |
5. HISTOPATHOLOGY OF SIL - (Easy to Draw Diagram)
Robbins Textbook Image - SIL Spectrum:
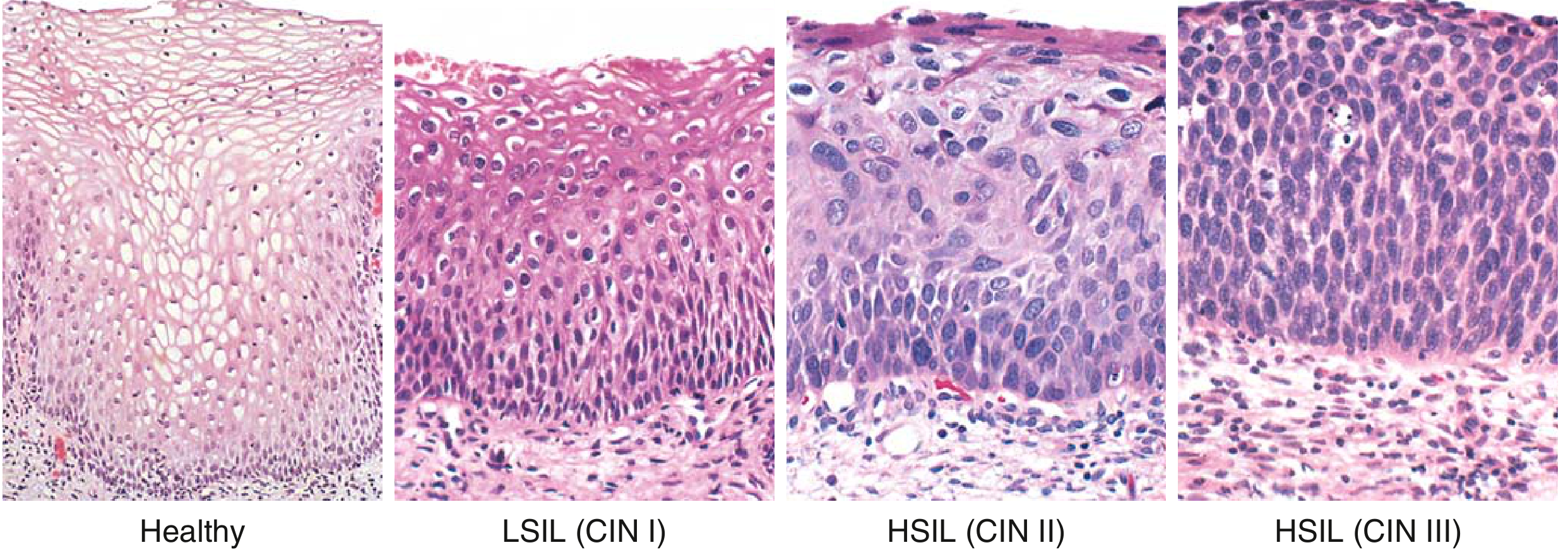
Easy-to-Draw Diagram for Exam:
NORMAL | CIN I (LSIL) | CIN II (HSIL) | CIN III (HSIL)
| | |
SURFACE | Koilocytes | Koilocytes + | No maturation
| (perinuclear | atypia lower | Atypia full
MIDDLE | halos) | 2/3 | thickness
| Atypia lower | |
BASAL | 1/3 only | Atypia lower | Atypia all
| | 2/3 | layers
BASEMENT |~~~~~~~~~~~~~~~~|~~~~~~~~~~~~~~~|~~~~~~~~~~~~~~~
MEMBRANE | INTACT | INTACT | INTACT
(No invasion in SIL - draw BM intact!)
Key histology features:
- Koilocytes = Hallmark of HPV infection = squamous cells with perinuclear halo + wrinkled/raisin-like nucleus
- As grade increases: ↑ nuclear:cytoplasmic ratio, ↑ mitoses (including atypical), ↓ maturation
- CIN III = carcinoma in situ = full thickness atypia, intact basement membrane
6. INVASIVE CARCINOMA OF CERVIX
Types:
- Squamous cell carcinoma (SCC) - 80% (most common)
- Adenocarcinoma + adenosquamous carcinoma - 15%
- Small cell neuroendocrine carcinoma - <5% (worst prognosis)
Gross Pathology (Easy to Draw):
Gross - Invasive Cervical Carcinoma:

Gross appearances:
┌──────────────────────────────────┐
│ GROSS TYPES OF CA CERVIX │
│ │
│ 1. EXOPHYTIC (most common) │
│ Cauliflower/fungating mass │
│ Protrudes out of cervical os │
│ │
│ 2. ENDOPHYTIC/ULCERATIVE │
│ Crater-like ulcer │
│ Necrotic base │
│ │
│ 3. BARREL CERVIX │
│ Circumferential growth │
│ Encircles entire cervix │
│ Hard, barrel-shaped cervix │
└──────────────────────────────────┘
Microscopy - SCC:
- Tongues and nests of squamous cells invading stroma
- Desmoplastic stromal response (fibrous stroma)
- Keratin pearls (well-differentiated tumors) = concentric layers of squamous cells with central keratin
- Atypical mitoses
- Stromal and vascular invasion
Easy Sketch for Exam - SCC Histology:
SURFACE EPITHELIUM
___________________
↓ Invasion
[Nest] [Keratin Pearl] [Nest]
↓ ↓ ↓
|||| Stroma (fibrous/desmoplastic) ||||
[Nest] [Nest]
Blood vessel with tumor
Microscopy - Adenocarcinoma:
- Mucin-secreting glandular cells
- Endocervical gland-like structures
- More common with HPV 18
7. STAGING OF CA CERVIX (FIGO)
| Stage | Description |
|---|---|
| I | Confined to cervix |
| II | Beyond cervix but not to pelvic wall |
| III | To pelvic wall or lower 1/3 vagina |
| IV | Bladder/rectum OR distant metastasis |
MUHS tip: Stage I → Surgery; Stage II/III → Radiation + Chemotherapy
8. SPREAD & METASTASIS
DIRECT EXTENSION:
Cervix → Vagina → Parametrium → Pelvic wall
→ Bladder (anterior) → Rectum (posterior)
LYMPHATIC (most important):
→ Internal iliac → External iliac → Para-aortic nodes
BLOOD-BORNE (late):
→ Lungs, Liver, Bones
- Risk of lymph node metastasis: <1% if invasion <3mm; >10% if invasion >3mm
9. CLINICAL FEATURES
- Most common symptom: Post-coital bleeding (contact bleeding)
- Irregular vaginal bleeding / metrorrhagia
- Foul-smelling vaginal discharge (leukorrhea)
- Dyspareunia (painful intercourse)
- Dysuria (bladder involvement)
- Back pain (pelvic wall involvement)
10. DIAGNOSIS
- Pap smear (Papanicolaou test) = gold standard screening
- Colposcopy (acetic acid → white lesions = acetowhite)
- Biopsy + Cone biopsy
- Schiller's test (iodine staining - normal = brown, abnormal = unstained)
11. TREATMENT & PROGNOSIS
- Stage I: Radical hysterectomy + pelvic lymph node dissection
- Stage II-III: Radiotherapy + Cisplatin chemotherapy
- Small cell: Very poor prognosis
- 5-year survival: Stage I ~90%; Stage IV ~15%
🟠 CARCINOMA OF ENDOMETRIUM
(Very Frequently Asked in MUHS - Type I vs Type II is a must!)
1. EPIDEMIOLOGY
- Most common gynecological cancer in developed countries
- Peak age: 55-65 years (postmenopausal)
- Usually presents early with postmenopausal bleeding
2. CLASSIFICATION - TYPE I vs TYPE II
This is the single most important concept for MUHS exams:
| Feature | TYPE I (Endometrioid) | TYPE II (Serous) |
|---|---|---|
| Frequency | 80-85% | 15% |
| Precursor | Atypical hyperplasia | Endometrial atrophy |
| Estrogen | Estrogen-dependent | NOT estrogen-dependent |
| Key mutation | PTEN, KRAS, PIK3CA, ARID1A | TP53 (>90%) |
| Grade | Low grade (well diff.) | High grade |
| Prognosis | Better | Poor |
| Age | Peri-menopausal | Post-menopausal (older) |
| Associated | Obesity, DM, HTN | Endometrial atrophy |
Mnemonic: "Type I = POKE me gently (PTEN, OKE = obesity/K-RAS/estrogen) = good prognosis" "Type II = TP53 = Terrible Prognosis = bad"
3. RISK FACTORS FOR TYPE I
┌──────────────────────────────────────────────┐
│ RISK FACTORS - CA ENDOMETRIUM │
│ │
│ ↑ ESTROGEN (unopposed = no progesterone) │
│ │
│ • Obesity - adipose tissue converts │
│ androgens to estrogens (aromatase) │
│ • Nulliparity │
│ • Late menopause │
│ • Estrogen-secreting ovarian tumors │
│ (granulosa cell tumor) │
│ • Exogenous estrogens │
│ • Tamoxifen use (weak estrogen effect) │
│ • Polycystic ovarian syndrome (PCOS) │
│ • Lynch syndrome (hereditary) │
│ - MLH1, MSH2 mutations │
│ • Cowden syndrome - PTEN germline mutation │
└──────────────────────────────────────────────┘
4. PATHOGENESIS
Type I (Endometrioid):
Unopposed Estrogen
↓
Endometrial Hyperplasia (without atypia)
↓
Atypical Hyperplasia (PTEN mutation = earliest event)
↓
Well-differentiated Endometrioid Carcinoma
↓
Mutations: PTEN (30-80%) → PIK3CA (40%) → KRAS (25%) → ARID1A (30%)
↓
Poorly differentiated with TP53 mutation (late event)
Type II (Serous):
Endometrial Atrophy (thin, atrophic endometrium)
↓
Serous Endometrial Intraepithelial Carcinoma (SEIC)
↓
TP53 mutation (EARLY event, >90%)
↓
High-grade Serous Carcinoma
5. ENDOMETRIAL HYPERPLASIA - Precursor
Robbins Textbook Image:
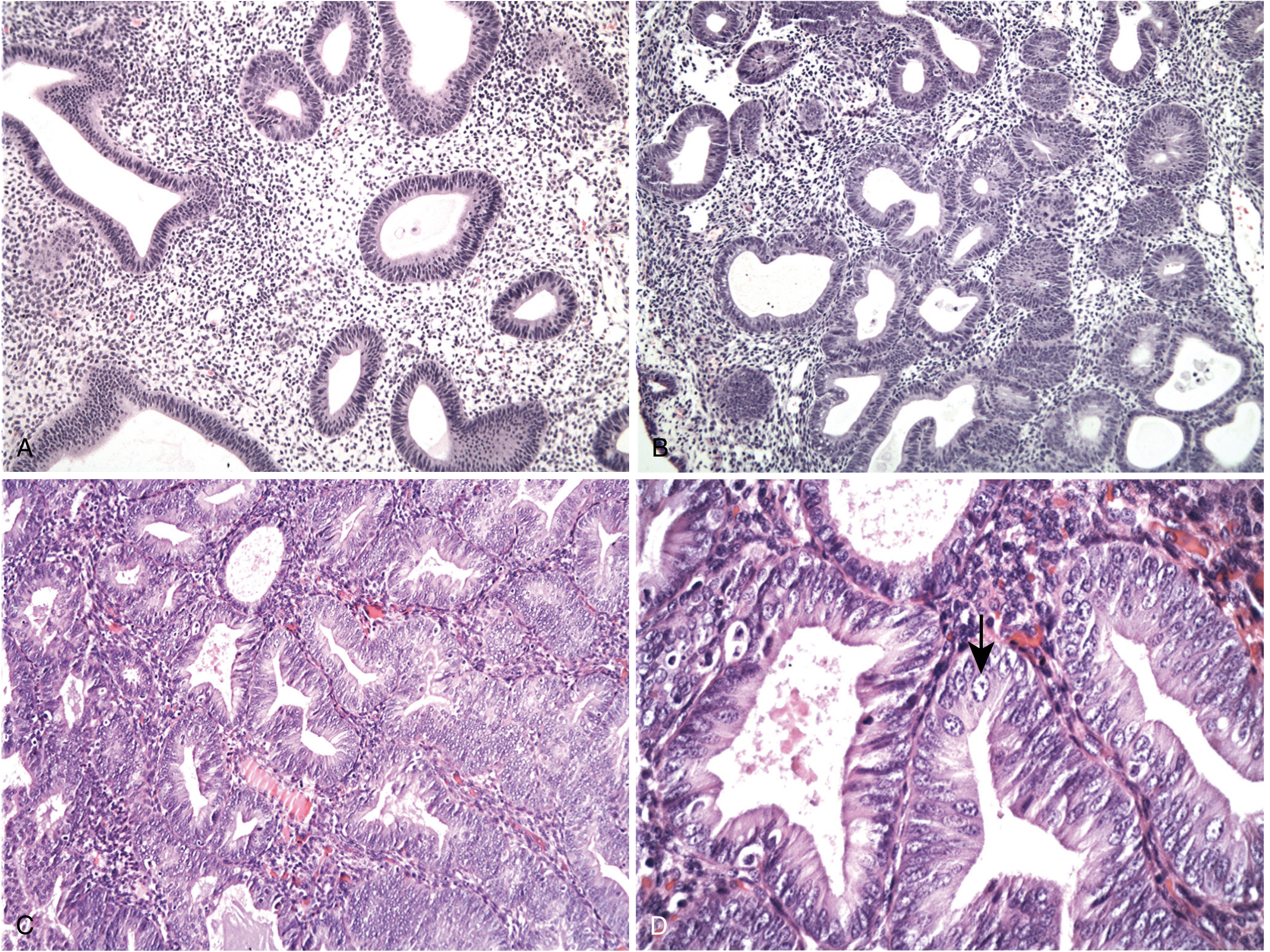
| Type | Risk of Cancer |
|---|---|
| Hyperplasia without atypia | ~1% |
| Atypical hyperplasia | ~30% |
Easy diagram for hyperplasia:
NORMAL ENDOMETRIUM:
[G][ S ][G][ S ][G] G=gland, S=stroma
Equal gland:stroma ratio
HYPERPLASIA WITHOUT ATYPIA:
[G][G][S][G][G][S][G]
↑ Glands, some crowding, NO atypia
ATYPICAL HYPERPLASIA (back-to-back glands):
[G][G][G][G][G][G][G]
Back-to-back glands, minimal stroma
Cells: rounded vesicular nuclei, prominent nucleoli
6. GROSS PATHOLOGY
┌──────────────────────────────────────┐
│ GROSS - CA ENDOMETRIUM │
│ │
│ Uterus enlarged │
│ │
│ Two patterns: │
│ 1. POLYPOID/EXOPHYTIC mass │
│ → Soft, tan-gray mass │
│ → Projects into uterine cavity │
│ → Like cauliflower │
│ │
│ 2. DIFFUSE - entire endometrium │
│ involved │
│ │
│ Cut section: │
│ → Gray-white tumor │
│ → May invade myometrium │
│ → Necrosis and hemorrhage │
└──────────────────────────────────────┘
7. HISTOPATHOLOGY
Robbins Textbook Image - Endometrioid Carcinoma (Serous type histology on right):
Endometrioid Carcinoma Histology:
- Tubular glands resembling proliferative endometrium
- Back-to-back glands with minimal intervening stroma
- Cells: columnar, stratified nuclei, moderate atypia
- Grading (FIGO 1-3):
Grade 1: >95% glandular pattern (well differentiated)
Grade 2: 6-50% solid areas
Grade 3: >50% solid areas (poorly differentiated)
Serous Carcinoma Histology:
- Papillary tufts and small clusters of highly atypical cells
- Marked cytologic atypia: high N:C ratio, atypical mitoses, hyperchromasia, prominent nucleoli
- IHC: Diffuse strong p53 positivity (mutant p53 accumulates)
Easy Sketch - Endometrioid Carcinoma:
╔══╗ ╔══╗ ╔══╗
║ ║ ║ ║ ║ ║ ← Back-to-back tubular glands
╚══╝ ╚══╝ ╚══╝ resembling endometrium
↑ ↑ ↑
Minimal stroma between
↓ Myometrial invasion
████████████████████████ ← myometrium (smooth muscle)
8. SPREAD & STAGING
Spread:
- Direct: Myometrial invasion → cervix → vagina
- Lymphatic: Pelvic → para-aortic nodes
- Blood-borne: Lungs, liver (late)
- Note: Serous carcinoma spreads transtubal → peritoneal implants (like ovarian Ca)
| FIGO Stage | Description |
|---|---|
| I | Confined to uterus |
| II | Involves cervical stroma |
| III | Beyond uterus but within pelvis/nodes |
| IV | Bladder/rectum or distant mets |
9. CLINICAL FEATURES
- Postmenopausal vaginal bleeding (cardinal symptom - early sign)
- Uterine enlargement
- Watery vaginal discharge
- Pelvic/back pain (advanced)
MUHS tip: "Any postmenopausal bleeding = carcinoma endometrium until proven otherwise"
10. DIAGNOSIS & TREATMENT
- Endometrial biopsy / D&C = definitive diagnosis
- TVUS: endometrial thickness >4mm (postmenopausal) = suspicious
- Treatment: Total abdominal hysterectomy + bilateral salpingo-oophorectomy (TAH + BSO)
- Radiotherapy if myometrial invasion >50%
- Prognosis: Overall 5-year survival ~75%; Stage I serous has worse prognosis than Stage I endometrioid
🟡 OVARIAN TUMORS
(Most Complex Topic - Asked Every Year in MUHS)
1. CLASSIFICATION (WHO / MUHS Standard)
┌─────────────────────────────────────────────────────┐
│ OVARIAN TUMORS │
├───────────────────────┬─────────────────────────────┤
│ I. SURFACE EPITHELIAL│ Most common (65-70%) │
│ TUMORS │ │
│ │ a. Serous (most common) │
│ │ b. Mucinous │
│ │ c. Endometrioid │
│ │ d. Clear cell │
│ │ e. Brenner tumor │
│ │ │
│ │ Each can be: │
│ │ Benign/Borderline/Malignant │
├───────────────────────┼─────────────────────────────┤
│ II. GERM CELL TUMORS │ 15-20% │
│ │ a. Teratoma (most common) │
│ │ - Mature (dermoid cyst) │
│ │ - Immature (malignant) │
│ │ b. Dysgerminoma │
│ │ c. Yolk sac tumor │
│ │ d. Choriocarcinoma │
├───────────────────────┼─────────────────────────────┤
│ III. SEX CORD-STROMAL│ 5-10% │
│ TUMORS │ a. Granulosa cell tumor │
│ │ b. Thecoma-fibroma │
│ │ c. Sertoli-Leydig cell │
│ │ (Arrhenoblastoma) │
├───────────────────────┼─────────────────────────────┤
│ IV. METASTATIC │ From GIT, breast, etc. │
│ TUMORS │ Krukenberg tumor (stomach) │
└───────────────────────┴─────────────────────────────┘
2. TYPE I vs TYPE II OVARIAN CARCINOMA
Robbins Diagram - Type I and Type II Carcinoma:
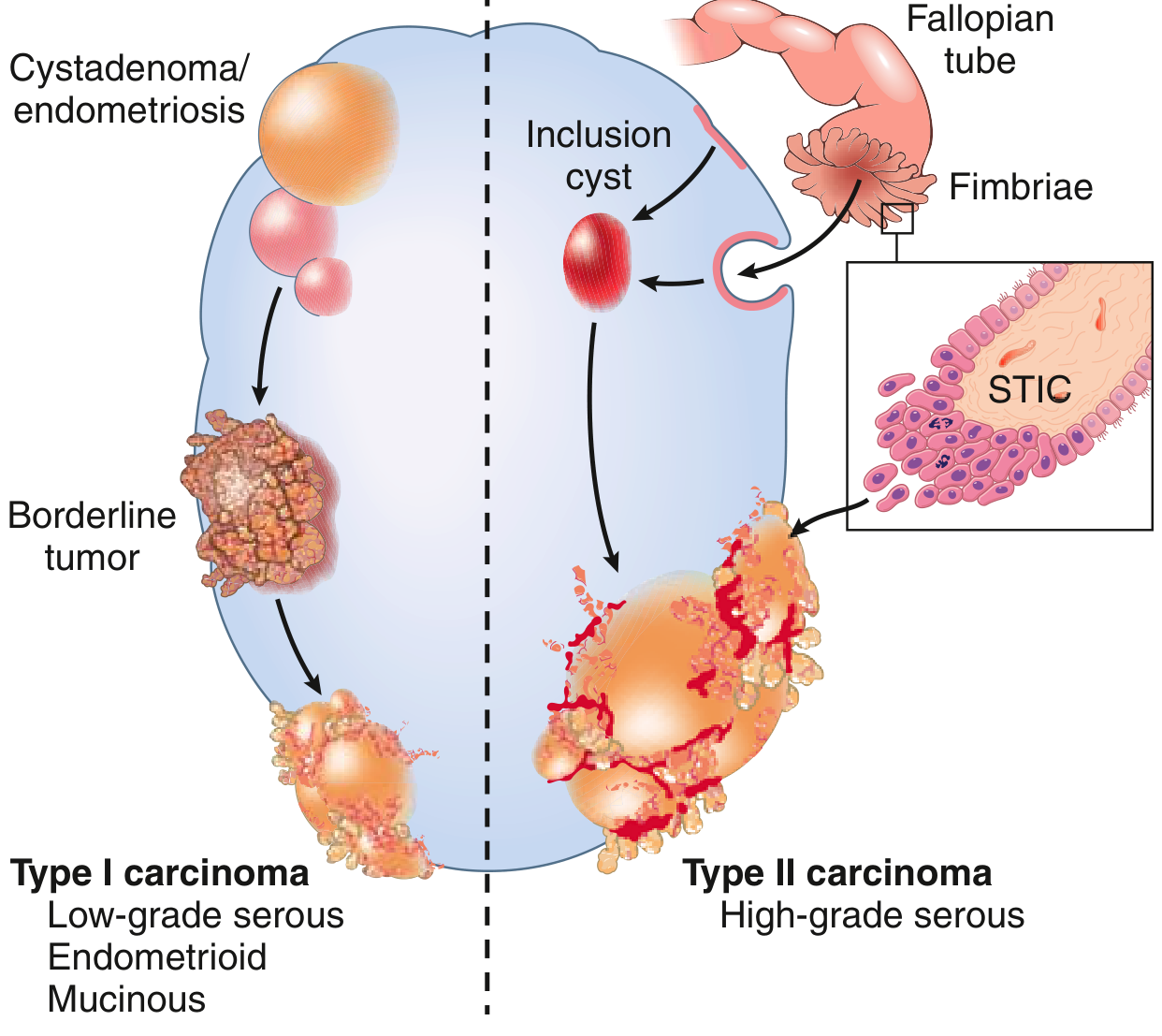
| Feature | Type I | Type II |
|---|---|---|
| Grade | Low grade | High grade |
| Histology | Low-grade serous, mucinous, endometrioid, clear cell | High-grade serous (most common) |
| Origin | Borderline tumors / endometriosis | Serous tubal intraepithelial carcinoma (STIC) in fallopian tube fimbriae |
| Mutations | KRAS, BRAF, ERBB2 (low-grade serous); KRAS (mucinous); PTEN, PIK3CA (endometrioid) | TP53 (>95%), BRCA1/BRCA2 |
| Progression | Slow, stepwise | Rapid |
| TP53 | Wild type | Mutated |
High-yield: BRCA1/BRCA2 mutations → almost ALL are high-grade serous (Type II) with TP53 mutations. Lifetime risk 20-60% with BRCA1/2 mutation.
3. SURFACE EPITHELIAL TUMORS
A. SEROUS TUMORS (Most Common)
Risk factors:
- Nulliparity, early menarche, late menopause
- Family history, BRCA1/2 mutations
- OCP use is protective (suppresses ovulation)
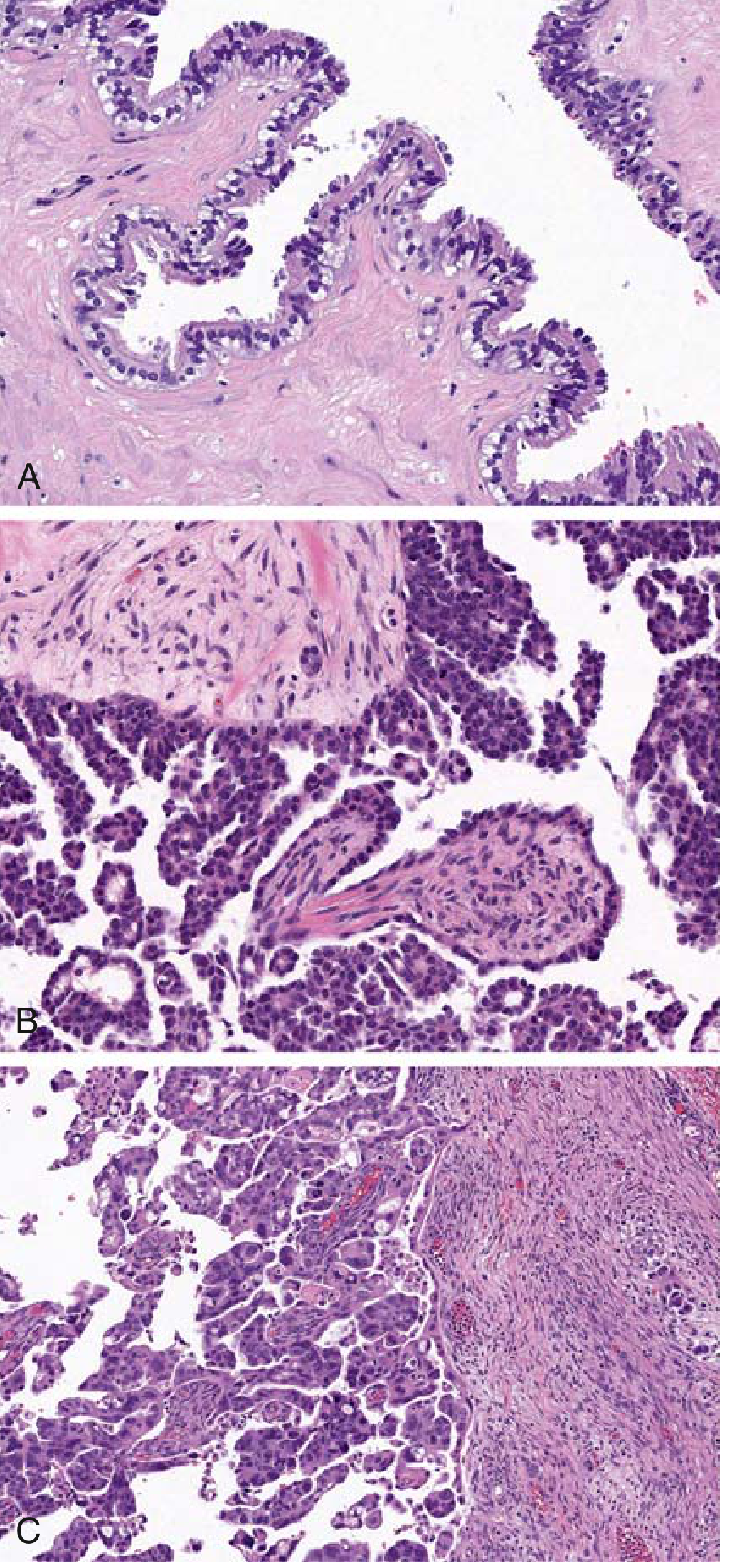
Gross - Serous Tumors:
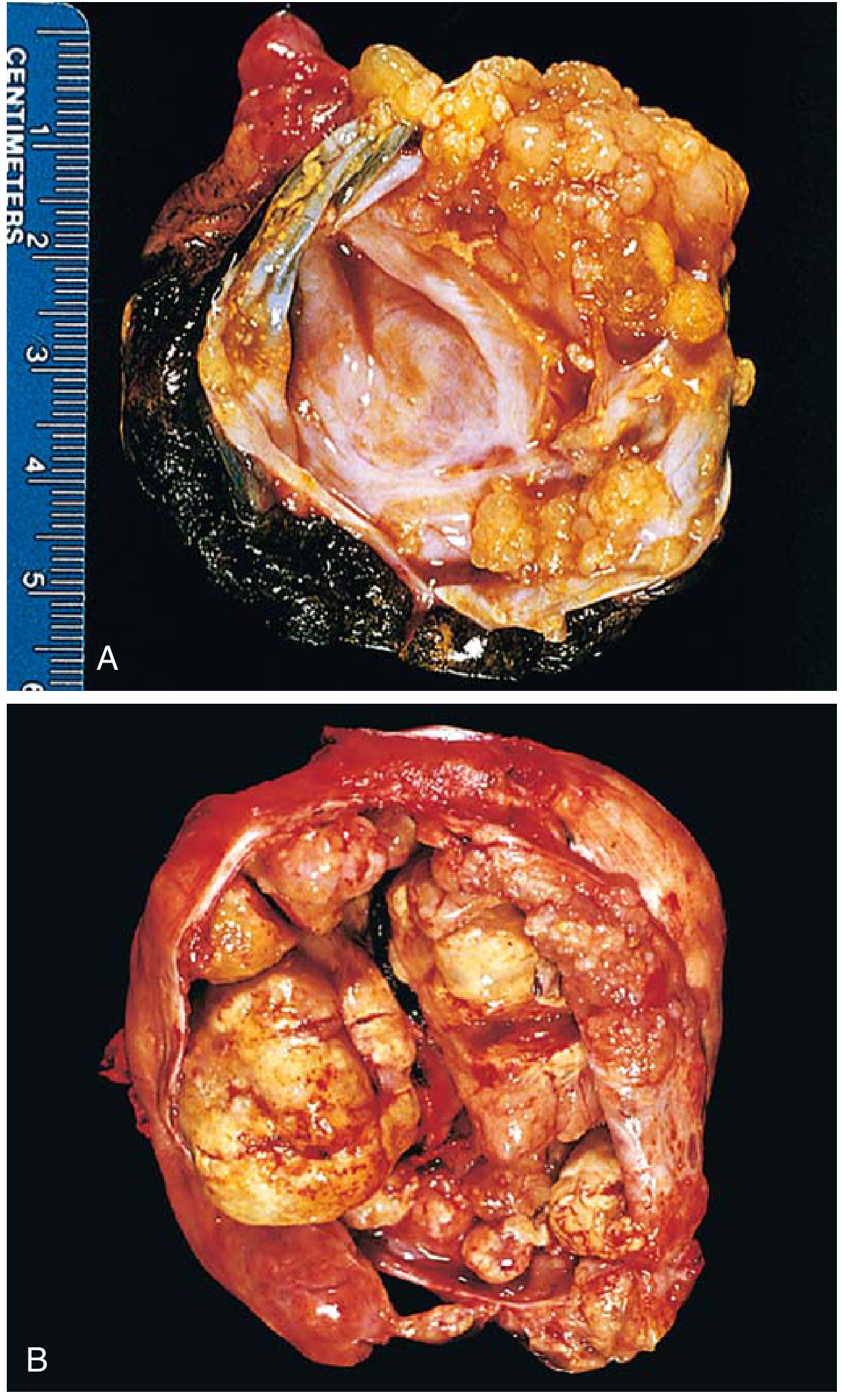 FIG. 17.16 - Robbins: Ovarian serous tumors - borderline serous tumor (A) and cystadenocarcinoma (B)
FIG. 17.16 - Robbins: Ovarian serous tumors - borderline serous tumor (A) and cystadenocarcinoma (B)
Gross Easy-Draw:
┌──────────────────────────────────────────────┐
│ SEROUS CYSTADENOMA (Benign) │
│ │
│ ╭──────────────────────╮ │
│ │ Thin-walled cyst │ │
│ │ Smooth inner lining │ │
│ │ Clear serous fluid │ │
│ │ Few small papillae │ │
│ ╰──────────────────────╯ │
│ Size: up to 30-40 cm │
│ 25% bilateral │
│ │
│ SEROUS CYSTADENOCARCINOMA (Malignant) │
│ │
│ ╭──────────────────────╮ │
│ │ Complex papillary │ ← Irregular, │
│ │ projections │ prominent │
│ │ Solid areas │ papillae │
│ │ Necrosis present │ │
│ │ Nodular outer │ │
│ │ surface (invasion) │ │
│ ╰──────────────────────╯ │
└──────────────────────────────────────────────┘
Histology - Serous Tumors (Robbins Image):
Histology Key Points:
- Benign (Cystadenoma): Single layer of tall ciliated columnar epithelium lining cyst
- Borderline: Epithelial stratification (2-3 layers), mild atypia, NO stromal invasion
- Malignant (Carcinoma): Complex papillary formations, marked atypia, STROMAL INVASION
- Psammoma bodies = concentric calcifications = characteristic of serous tumors
Easy Sketch - Serous Tumor Histology:
BENIGN: BORDERLINE: MALIGNANT:
┌──────┐ ┌──────┐ ┌──────┐
│ │ │ │ ||| │ │█████│
│Cilia │ │Strat.│ No │Papil│
│Single│ │ 2-3 │ invasion │Atyp │
│layer │ │layers│ │Invas│
└──────┘ └──────┘ └──────┘
Psammoma Body (Easy Draw):
[Concentric rings of calcification]
like a target/bull's-eye
○○○ ← outer ring
○○ ← middle
○ ← central
Clinical Features & Prognosis:
- 5-year survival: borderline confined to ovary = 100%; malignant confined = 70%; malignant + peritoneal spread = 25%
- Often associated with ascites
- Spreads to peritoneal surfaces and omentum
B. MUCINOUS TUMORS
| Feature | Details |
|---|---|
| Bilaterality | Rare (cf. serous which is 25% bilateral) |
| Contents | Thick, gelatinous mucin |
| Size | Often very large, multicystic |
| Key mutation | KRAS |
| Malignant % | Only 10% |
Gross - Mucinous Cystadenoma:
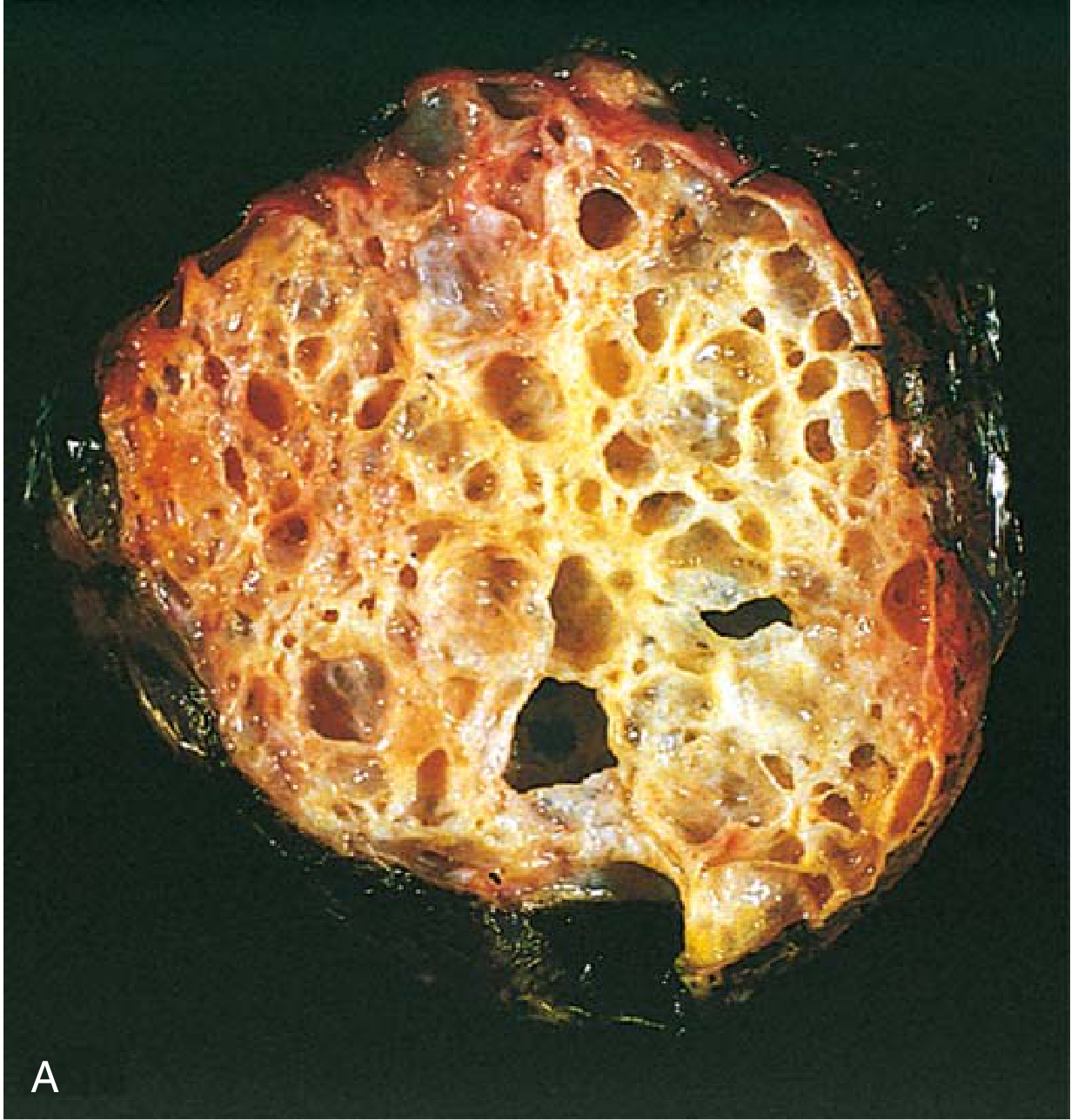
Histology: Mucin-secreting tall columnar cells (like intestinal epithelium), NO cilia, mucin-filled glands
Pseudomyxoma Peritonei:
- Rupture of mucinous tumor → mucin seeds peritoneum
- When caused by ovarian tumor: usually resolves
- Most cases of pseudomyxoma peritonei are actually from appendiceal mucinous tumors
Krukenberg Tumor:
- Metastatic mucin-secreting adenocarcinoma to both ovaries (bilateral)
- Most common primary site = stomach
- Histology: Signet ring cells (mucin pushes nucleus to periphery) in fibrous stroma
C. ENDOMETRIOID TUMORS
- Resemble endometrial glands histologically (tubular glands)
- 20% bilateral
- 15-20% are associated with simultaneous endometrial carcinoma
- Associated with endometriosis
- Mutations: PTEN, PIK3CA (same as endometrial carcinoma)
D. CLEAR CELL CARCINOMA
- Large cells with abundant clear cytoplasm (glycogen-rich)
- Resembles hypersecretory gestational endometrium
- Associated with endometriosis or endometrioid carcinoma
- Treated like other ovarian carcinomas
4. GERM CELL TUMORS
TERATOMAS (15-20% of ovarian tumors; >90% are benign)
A. Mature (Benign) Teratoma = Dermoid Cyst
GROSS FEATURES (Easy Draw):
┌────────────────────────────────────────┐
│ DERMOID CYST / MATURE TERATOMA │
│ │
│ ╭──────────────────────────╮ │
│ │ Outer: smooth capsule │ │
│ │ Inner: skin-like lining │ │
│ │ Contents: │ │
│ │ - Sebaceous material │ │
│ │ - Hair / matted hair │ │
│ │ - Teeth (25%) │ │
│ │ - Bone/cartilage │ │
│ │ - Thyroid tissue │ │
│ │ "Rokitansky protuberance"│ │
│ │ = mural nodule with │ │
│ │ teeth projecting │ │
│ ╰──────────────────────────╯ │
│ Size: Usually <10 cm │
│ 90% UNILATERAL │
│ Right side more common │
└────────────────────────────────────────┘
Histology:
- Tissues from ALL THREE germ cell layers:
- Ectoderm: skin, hair, sebaceous glands, teeth, neural tissue
- Endoderm: bronchial/intestinal epithelium, thyroid
- Mesoderm: bone, cartilage, muscle
B. Immature Teratoma (Malignant)
- Immature/embryonic neural tissue (neuroepithelium)
- Graded 1-3 by amount of immature neural tissue
- More common in young women
- AFP may be raised
C. Monodermal Teratomas:
- Struma ovarii = all thyroid tissue → can cause hyperthyroidism
- Carcinoid tumor of ovary
5. SEX CORD-STROMAL TUMORS
GRANULOSA CELL TUMOR (Most Important)
KEY FACTS:
• Produces ESTROGEN (feminizing tumor)
• Causes: Precocious puberty (child), Postmenopausal bleeding,
Endometrial hyperplasia → endometrial carcinoma
• Histology: Call-Exner bodies (coffee bean nuclei)
• Marker: Inhibin positive
• Low malignant potential (late recurrence >20 years)
Call-Exner Bodies (Easy Draw):
Granulosa cells arranged around
central accumulation of eosinophilic material
[◦◦◦◦◦◦◦] ← granulosa cells
[◦ ♦ ◦] ← Call-Exner body (eosinophilic center)
[◦◦◦◦◦◦◦]
"Coffee bean" nuclei = nuclear groove
THECOMA-FIBROMA
| Thecoma | Fibroma |
|---|---|
| Estrogenic | Non-functional |
| Yellow on cut section | Firm, white, whorled |
| Endometrial hyperplasia | Associated with Meigs syndrome |
| Meigs = fibroma + ascites + pleural effusion |
SERTOLI-LEYDIG CELL TUMOR (Arrhenoblastoma)
- Produces androgens (virilizing tumor)
- Causes: hirsutism, amenorrhea, clitoromegaly, deepening of voice
- Rare, young women
6. MARKERS FOR OVARIAN TUMORS
| Tumor | Tumor Marker |
|---|---|
| Epithelial (serous/mucinous) | CA-125 (most important) |
| Yolk sac tumor | AFP (alpha-fetoprotein) |
| Dysgerminoma | LDH |
| Choriocarcinoma | β-hCG |
| Granulosa cell tumor | Inhibin |
| Immature teratoma | AFP |
| Krukenberg / mucinous | CEA |
7. RISK FACTORS FOR EPITHELIAL OVARIAN CANCER
INCREASE RISK: DECREASE RISK:
• Age >45 • OCP use (protective)
• Nulliparity • Multiparity
• Early menarche • Breastfeeding
• Late menopause • Tubal ligation
• Family history • Oophorectomy
• BRCA1/BRCA2
• Lynch syndrome
• Endometriosis
8. CLINICAL FEATURES OF OVARIAN CANCER
- Silent killer - often presents late (Stage III/IV)
- Abdominal distension/pain
- Ascites (very common)
- Pelvic mass
- Weight loss
- Early satiety (omental involvement)
- Pleural effusion (advanced)
9. FIGO STAGING - OVARIAN CANCER
| Stage | Description |
|---|---|
| I | Confined to ovaries |
| II | Pelvic extension |
| III | Peritoneal implants outside pelvis / retroperitoneal nodes |
| IV | Distant metastasis |
70% cases are diagnosed at Stage III-IV (poor prognosis)
COMPARATIVE SUMMARY TABLE (MUHS Exam Quick Review)
| Feature | Ca Cervix | Ca Endometrium | Ovarian Cancer |
|---|---|---|---|
| Most common type | SCC (80%) | Endometrioid (80%) | Serous carcinoma |
| Key etiology | HPV 16/18 | Unopposed estrogen | BRCA1/2; KRAS; TP53 |
| Peak age | 45-55 yrs | 55-65 yrs | 45-65 yrs |
| Precursor | CIN/SIL | Atypical hyperplasia | Borderline tumor / STIC |
| Hallmark symptom | Post-coital bleeding | Postmenopausal bleeding | Silent, ascites (late) |
| Gross | Exophytic/ulcerative | Polypoid endometrial mass | Large cystic/solid mass |
| Key histology | Keratin pearls; desmoplasia | Back-to-back glands | Papillae; psammoma bodies |
| Spread | Direct + lymphatic | Myometrial invasion | Peritoneal dissemination |
| Key mutation | E6→p53; E7→RB | PTEN (Type I); TP53 (Type II) | TP53 (high grade); KRAS (low grade) |
| Screening | Pap smear | None (endometrial biopsy if symptomatic) | CA-125 + TVS (not ideal) |
| Treatment | Surgery/RT/Chemo | TAH + BSO | Surgery + Platinum/Taxol |
FREQUENTLY ASKED MUHS EXAM QUESTIONS & SHORT ANSWERS
Q: What is the transformation zone?
→ Junction between squamous ectocervix and columnar endocervix; site of metaplasia and HPV-induced carcinogenesis; most common site for CIN and invasive carcinoma.
Q: What are koilocytes?
→ Squamous cells with perinuclear halo + wrinkled/raisin nuclei = pathognomonic of HPV infection; seen in CIN I/LSIL.
Q: What is Meigs syndrome?
→ Ovarian fibroma + ascites + right-sided pleural effusion; resolves after tumor removal.
Q: What is Krukenberg tumor?
→ Bilateral metastatic mucin-secreting carcinoma of the ovary; signet ring cells; most commonly from stomach carcinoma.
Q: What is pseudomyxoma peritonei?
→ Diffuse mucinous implants throughout peritoneal cavity; most commonly from appendiceal mucinous tumor (not primary ovarian).
Q: Granulosa cell tumor - hallmark histology?
→ Call-Exner bodies (granulosa cells arranged around central eosinophilic material); coffee-bean nuclei (nuclear grooves); positive for inhibin.
Q: Differentiate psammoma bodies?
→ Concentric calcifications; seen in serous tumors (ovary, thyroid papillary carcinoma, meningioma, mesothelioma) - NOT specific for malignancy alone.
Q: Type I vs Type II endometrial carcinoma - key differences?
→ Type I = endometrioid, estrogen-dependent, PTEN mutation, better prognosis.
Type II = serous, non-estrogen-dependent, TP53 mutation (>90%), poor prognosis, like ovarian serous carcinoma behavior.
References: Robbins & Kumar Basic Pathology (10th Ed.), Robbins Cotran & Kumar Pathologic Basis of Disease (10th Ed.)
This is a shared conversation. Sign in to Orris to start your own chat.