Rapid sequence induction, modified rapid sequence induction, rapid sequence intubation, rapid sequence induction and intubation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Rapid Sequence Induction / Intubation (RSI / RSII)
Definition and Purpose
RSI is the cornerstone of emergency airway management. It is defined as the nearly simultaneous administration of a potent sedative (induction) agent and a neuromuscular blocking agent (NMBA), after a period of preoxygenation and cardiopulmonary optimization, for tracheal intubation. The technique was initially developed to safely intubate patients while minimizing the risk of pulmonary aspiration of gastric contents, and it avoids bag-mask ventilation (BMV) between induction and intubation to reduce the risk of gastric insufflation and regurgitation.
RSI accounts for ~85% of all ED intubations in recent large registry data. - Rosen's Emergency Medicine, 9e
The terms are used with subtle distinctions:
- Rapid sequence induction (RSI) - primarily the anesthesia literature's term, focusing on the induction phase.
- Rapid sequence intubation (RSI) - the emergency medicine term, emphasizing the full sequence through secured airway.
- Rapid sequence induction and intubation (RSII) - the combined, most precise term used in surgery and trauma.
- Modified RSI - a variant allowing gentle BMV with cricoid pressure (see below).
The 7 Ps of RSI
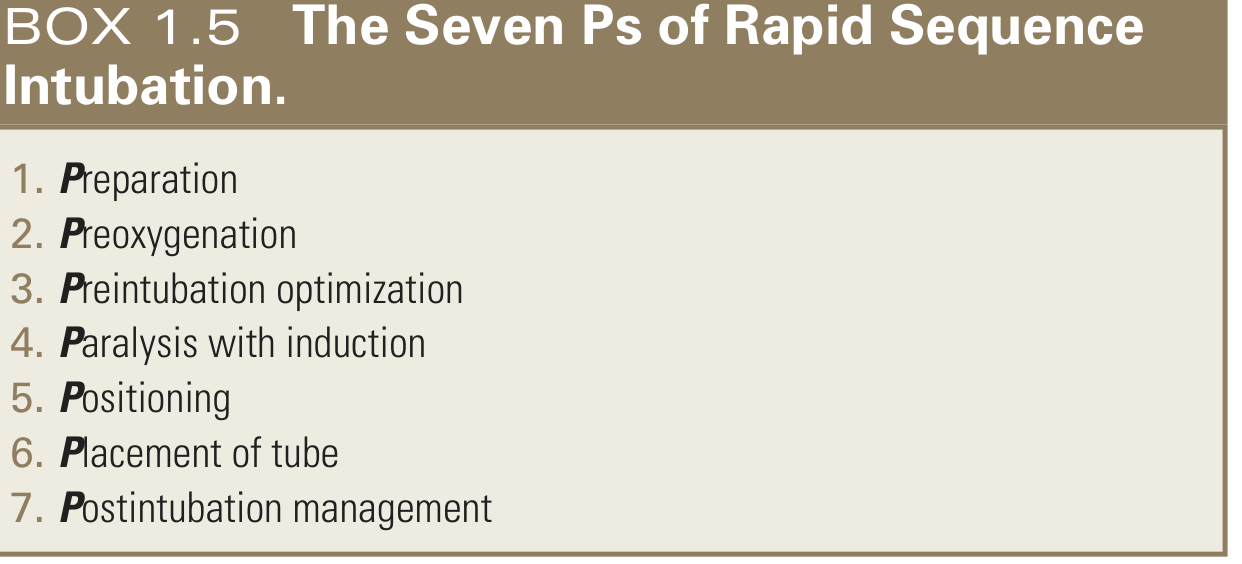
(Rosen's Emergency Medicine, 9e - Box 1.5)
1. Preparation
Assess the patient for intubation difficulty and abnormal physiology. Draw up and label all drugs. Assemble all equipment (laryngoscope, video laryngoscope, tube sizes, stylet, suction). Establish at least two IV lines. Formulate a rescue plan for failed airway and communicate it to the team. Continuous cardiac monitoring and pulse oximetry required.
2. Preoxygenation
Goal: denitrogenation of alveoli to form an oxygen-rich reservoir within the lung's functional residual capacity (FRC, ~30 mL/kg in adults).
- Traditional method: 3 minutes of tidal breathing via non-rebreather mask at 15 L/min - but this only achieves FiO₂ ~65%.
- Preferred: flush-rate oxygen (40-70 L/min) significantly increases FiO₂ and end-tidal O₂ by outcompeting room air entrainment. Achieved by fully opening the wall oxygen valve.
- Alternatively: 8 vital capacity breaths of 100% O₂ over 60 seconds is acceptable if time is limited.
- Effective preoxygenation allows 6-8 minutes of safe apnea before SpO₂ falls below 90% in a healthy adult.
- Children, obese patients, late-term pregnant women, and critically ill patients desaturate considerably faster.
- Apneic oxygenation: applying nasal cannula at 10-15 L/min (or high-flow humidified O₂ up to 60 L/min) during intubation attempts further extends safe apnea time.
3. Preintubation Optimization (formerly "Premedication")
Correct reversible physiologic derangements before induction:
- Hypoxemia: maximize preoxygenation as above.
- Hypotension: administer a fluid bolus or vasopressor (phenylephrine, norepinephrine) before induction to prevent peri-induction cardiovascular collapse.
- Severe acidosis: consider sodium bicarbonate.
- Optional adjunct medications include fentanyl (1-3 mcg/kg) to blunt sympathetic response in hypertensive emergencies (e.g., intracranial hemorrhage), lidocaine (1.5 mg/kg IV), or atropine (0.01 mg/kg in children to prevent vagal bradycardia from laryngoscopy). Defasciculating agents (vecuronium or rocuronium at 1/10 induction dose) have been used but are controversial.
4. Paralysis with Induction
The induction agent and NMBA are administered in rapid succession (nearly simultaneously). The NMBA is not withheld until the patient loses consciousness - it is pushed immediately after the induction agent.
5. Positioning
- Place patient supine with head elevated ~20-30 degrees (ramped position for obese patients).
- Apply cricoid pressure (Sellick maneuver) if used: 10 N of force while awake, increased to 30 N after loss of consciousness (LOC). This is the most controversial step in RSI (see below).
- Wait ~45-60 seconds after NMBA administration.
6. Placement of Tube
At 45-60 seconds, confirm adequate relaxation (test jaw mobility). Perform laryngoscopy under direct or video visualization and place the ETT. Confirm with end-tidal CO₂ capnography immediately.
7. Postintubation Management
- Chest X-ray to exclude mainstem intubation.
- Initiate continuous capnography.
- Administer adequate sedation and analgesia: midazolam 0.1-0.2 mg/kg + fentanyl 0.5-1 mcg/kg or morphine 0.2-0.3 mg/kg.
- Propofol infusion (0.05-0.1 mg/kg/min) is useful for neurologic emergencies (short duration allows frequent neuro checks).
- Avoid long-acting NMBAs post-intubation unless necessary.
Sample RSI Protocol (Etomidate + Succinylcholine)
| Time | Step |
|---|---|
| T-10 min | Preparation |
| T-5 min | Preoxygenation - 100% O₂ for 3 min or 8 vital capacity breaths |
| T-3 min | Preintubation optimization as indicated |
| T-0 | Paralysis with induction: Etomidate 0.3 mg/kg + Succinylcholine 1.5 mg/kg |
| T+30 s | Positioning; optional Sellick maneuver |
| T+45 s | Placement: laryngoscopy, intubation, EtCO₂ confirmation |
| T+2 min | Postintubation management: sedation/analgesia, mechanical ventilation |
(Rosen's Emergency Medicine, 9e - Table 1.1)
Induction Agents
| Agent | Dose | Onset | Duration | Benefits | Caveats |
|---|---|---|---|---|---|
| Etomidate | 0.3-0.5 mg/kg IV | <1 min | 10-20 min | Hemodynamically neutral, ↓ICP, ↓IOP, antiemetic | Myoclonus, cortisol suppression (single dose clinical significance debated), no analgesia |
| Ketamine | 1-2 mg/kg IV | ~1 min | 10-20 min | Bronchodilator, dissociative amnesia, analgesia, maintains BP | ↑Secretions, ↑BP, emergence phenomenon |
| Propofol | 0.5-1.5 mg/kg IV | 20-40 s | 8-15 min | Smooth induction, ↓ICP | ↓BP (significant), apnea |
| Thiopental | 3-5 mg/kg IV | <1 min | 5-10 min | Historical standard, ↓ICP | Severe hypotension, not widely available |
| Midazolam | 0.1-0.3 mg/kg IV | 1-2 min | 15-30 min | Amnestic, available | Slow onset, hypotension |
(Tintinalli's Emergency Medicine - Table 29A-8)
Etomidate + succinylcholine is the most common ED combination; ketamine is preferred in bronchospasm or hemodynamic instability.
Neuromuscular Blocking Agents (NMBAs)
| Agent | Type | Dose | Onset | Duration | Notes |
|---|---|---|---|---|---|
| Succinylcholine | Depolarizing | 1.5 mg/kg IV (4 mg/kg IM) | 45-60 s | 5-9 min (full recovery 8-12 min) | Gold standard; rapid offset allows spontaneous ventilation to return quickly |
| Rocuronium | Non-depolarizing | 1.0-1.2 mg/kg IV | 60-90 s | 30-60 min | Best succinylcholine alternative; reversed by sugammadex (200 mg if high-dose used) |
| Vecuronium | Non-depolarizing | 0.08-0.28 mg/kg IV | 2-4 min | 25-120 min | Slower onset; prolonged in obesity, elderly, hepatorenal dysfunction |
(Tintinalli's Emergency Medicine - Table 29A-9; Miller's Anesthesia 10e)
Succinylcholine: Complications and Contraindications
| Complications | Absolute/Relative Contraindications |
|---|---|
| Fasciculations | Pre-existing hyperkalemia |
| Transient ↑intragastric, intraocular, and intracranial pressure | Burns >5 days old |
| Bradycardia (especially pediatric) | Denervation injuries >5 days old (e.g., spinal cord injury, stroke) |
| Masseter spasm | Significant crush injuries >5 days old |
| Malignant hyperthermia (in genetically susceptible) | Severe infection >5 days old |
| Prolonged apnea with pseudocholinesterase deficiency | Pre-existing myopathies (Duchenne's, etc.) |
- Mechanism of hyperkalemia: succinylcholine triggers extrajunctional ACh receptor upregulation, causing exaggerated K⁺ efflux. Average rise is ~0.5 mEq/L in normal patients - clinically insignificant unless baseline K⁺ is already elevated or there is denervation/upregulation.
- Cocaine use reduces plasma cholinesterase availability, potentially prolonging blockade.
- Treat suspected malignant hyperthermia with dantrolene 2.5 mg/kg IV + temperature control.
When succinylcholine is contraindicated: use rocuronium 1.0-1.2 mg/kg (high-dose provides comparable intubating conditions within 90 seconds, and sugammadex reverses it rapidly if needed). - Miller's Anesthesia, 10e
Cricoid Pressure (Sellick Maneuver)
The most controversial component of RSI. Applied to the cricoid cartilage to compress the esophagus and prevent passive regurgitation into the pharynx.
Arguments for:
- The cricoid forms a complete cartilaginous ring - pressure on it collapses underlying soft tissue.
- Widely practiced; recommended force: 10 N awake → 30 N after LOC.
- Low risk if properly applied.
Arguments against:
- MRI studies show the esophagus laterally displaces rather than compresses.
- Decreases lower esophageal sphincter tone, potentially increasing regurgitation risk.
- Worsens laryngeal visualization during direct laryngoscopy.
- Can occlude the subglottic airway, impeding mask ventilation and intubation.
- Not validated in prospective RCTs to reduce aspiration.
Practical guidance: Apply cricoid pressure unless it worsens glottic visualization, in which case release or reduce force. Maintain until cuff is inflated and position confirmed. - Miller's Anesthesia, 10e; Morgan & Mikhail, 7e
Modified RSI (mRSI)
No single standardized definition exists. In a US survey, modified RSI most commonly refers to gentle bag-mask ventilation in conjunction with cricoid pressure between induction and intubation. - Miller's Anesthesia, 10e
Rationale: Some patients cannot be safely managed without some ventilation before the tube is placed:
- Obese patients
- Pregnant patients (late second/third trimester)
- Critically ill patients with severe hypoxemia
- Pediatric patients
- Patients in whom adequate preoxygenation was impossible
Technique: Gentle PPV with inspiratory pressure <20 cmH₂O, applied while maintaining cricoid pressure. The aim is to prevent severe desaturation without significantly distending the stomach.
A multicenter ICU RCT showed that BMV during RSI significantly reduced desaturation and improved oxygen nadirs compared to no-BMV, with no difference in witnessed aspiration or subsequent chest X-ray infiltrates. However, the high-risk aspirators were excluded, limiting broad extrapolation to the ED. - Rosen's EM, 9e
As a general rule, modified RSI is appropriate when the risk of desaturation outweighs the risk of aspiration.
Indications for RSI
- Full stomach (NPO guidelines not observed)
- Bowel obstruction
- Active upper GI bleeding / recent vomiting
- Morbid obesity
- Pregnancy (second trimester onward - though some have questioned this in elective cases)
- Poorly controlled GERD
- Nasogastric tube in situ
- Diabetic gastroparesis
- Predicted difficult mask ventilation with reassuring airway (e.g., edentulous bearded patient)
Contraindications / When NOT to Use Standard RSI
- Anticipated difficult airway where intubation success is uncertain - awake intubation or video laryngoscopy is preferred.
- Deeply comatose patients or cardiac arrest - may be intubated without any drugs.
- Succinylcholine contraindications (see above) - use rocuronium instead, or use modified RSI.
- Tracheal RSI is specifically not indicated when the patient can be managed with a supraglottic airway or awake technique.
Delayed Sequence Intubation (DSI)
A related technique for patients who are too agitated or delirious to cooperate with preoxygenation. Dissociative-dose ketamine (1-2 mg/kg IV) is given first as procedural sedation to allow adequate preoxygenation, followed by completion of RSI with an NMBA. DSI separates the "preparation" from the "paralysis" step to optimize oxygen reserve before apnea is induced. - Rosen's Emergency Medicine, 9e
Special Populations
| Population | Consideration |
|---|---|
| Trauma / full stomach | RSII with at least 4 providers; in-line cervical stabilization; suction ready |
| TBI / intracranial hypertension | RSI with agents that ↓ICP (etomidate, propofol); avoid ketamine if ICP elevated (debated) |
| Hemodynamic instability | Ketamine preferred; avoid propofol; vasopressors before induction |
| Severe asthma / bronchospasm | Ketamine preferred (bronchodilation); consider ketamine + rocuronium |
| Hyperkalemia | Succinylcholine contraindicated; use rocuronium 1.2 mg/kg |
| Burns / denervation >5 days | Succinylcholine contraindicated; rocuronium + sugammadex plan |
| ESRD (renal failure) | Modified RSI with rocuronium may substitute for succinylcholine if hyperkalemia present |
| Pregnancy | Modified RSI preferred; rocuronium increasingly used; head-up position |
| Pediatric | Atropine premedication (0.01-0.02 mg/kg) to blunt vagal response; succinylcholine 2 mg/kg <10 kg |
| Obese | Ramped positioning; apneic oxygenation; shortened safe apnea window |
Key Drugs and Doses Summary
| Drug | Role | Dose |
|---|---|---|
| Etomidate | Induction | 0.3 mg/kg IV |
| Ketamine | Induction | 1-2 mg/kg IV |
| Propofol | Induction | 0.5-1.5 mg/kg IV |
| Succinylcholine | Paralysis (depolarizing) | 1.5 mg/kg IV |
| Rocuronium | Paralysis (non-depolarizing) | 1.0-1.2 mg/kg IV |
| Sugammadex | Rocuronium reversal | 16 mg/kg (immediate), 4 mg/kg (routine) |
| Fentanyl | Premedication (blunt sympathetics) | 1-3 mcg/kg IV |
| Midazolam | Post-intubation sedation | 0.1-0.2 mg/kg IV |
| Atropine | Pediatric premedication | 0.01-0.02 mg/kg IV |
Sources: Rosen's Emergency Medicine 9e; Tintinalli's Emergency Medicine; Miller's Anesthesia 10e; Current Surgical Therapy 14e; Morgan & Mikhail's Clinical Anesthesiology 7e; Barash's Clinical Anesthesia 9e
Difficult airway guidelines
Finding Sources
Searching PubMed
"difficult airway" AND "guidelines" AND "management"
Reading File
Reading File
Reading File
Reading Article
PMID: 41203471
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive material. Let me compile the full structured answer.
Difficult Airway Guidelines
Definition of a Difficult Airway
A difficult airway exists when a conventionally trained clinician experiences difficulty with any or all of the following:
- Facemask ventilation (BMV)
- Supraglottic airway (SGA/EGD) placement
- Laryngoscopy
- Tracheal intubation
- Surgical airway access
The ASA (American Society of Anesthesiologists) and the Difficult Airway Society (DAS) are the two most influential bodies issuing guidelines. The DAS updated its guidelines for unanticipated difficult tracheal intubation in adults in 2025 (published January 2026, PMID 41203471).
Step 1: Pre-Airway Assessment - Identifying the Difficult Airway
Fewer than 50% of difficult intubations can be predicted, and most standard tests (Mallampati, thyromental distance) are not applicable in emergency settings (2/3 of ED patients cannot cooperate with these assessments). Only obvious anatomic/pathologic abnormalities and a prior history of difficult intubation are reliable predictors. - Roberts & Hedges' Clinical Procedures in Emergency Medicine
Four systematic mnemonics (from Walls' Manual / Rosen's Emergency Medicine) evaluate each component of the airway:
LEMON - Difficult Direct Laryngoscopy
| Letter | Assessment |
|---|---|
| L - Look externally | Obvious gestalt: trauma, blood, obesity, large tongue, beard, collar |
| E - Evaluate 3-3-2 rule | 3 fingers: inter-incisor gap; 3 fingers: floor of mandible (mentum to hyoid); 2 fingers: thyromental (laryngeal prominence to chin). Any reduction predicts difficulty |
| M - Mallampati | Class I (full view) = easy; Class III/IV = difficulty; requires awake, cooperative patient |
| O - Obstruction / Obesity | Supraglottic obstruction (abscess, hematoma, angioedema, tumor), obesity, OSA |
| N - Neck mobility | Reduced extension (arthritis, collar, ankylosing spondylitis, prior fusion) |
Cormack-Lehane grading of laryngoscopic view:
- Grade 1: full glottis visible (~100% success)
- Grade 2a: arytenoids + partial cords (success drops minimally)
- Grade 2b: arytenoids only (~65% success)
- Grade 3: epiglottis only (highly difficult)
- Grade 4: no epiglottis visible (<1% of elective cases; extremely difficult)
ROMAN - Difficult Bag-Mask Ventilation
| Letter | Factor |
|---|---|
| R - Radiation/Resistance | Head/neck radiation, intrinsic lung disease (asthma, COPD, ARDS) requiring high pressures |
| O - Obstruction/Obesity/OSA | Supraglottic obstruction, obesity, obstructive sleep apnea |
| M - Mallampati/Mask seal/Male | High Mallampati, beard/facial trauma (poor seal), male sex |
| A - Age | >55 years (physiologic appearance is more useful than chronologic age) |
| N - No teeth | Edentulous patients - loss of strut for mask seal. "Teeth out to intubate, teeth in to ventilate" |
RODS - Difficult Extraglottic Device (SGA/LMA) Placement
| Letter | Factor |
|---|---|
| R - Restricted mouth opening / Resistance | <2 fingers mouth opening; high airway resistance |
| O - Obstruction/Obesity/OSA | Mass effect, large tongue, redundant tissue |
| D - Distorted/Disrupted airway | Trauma, tumor, prior surgery distorting anatomy |
| S - Short thyromental distance | Receded mandible - tongue sits posteriorly, obstructs EGD seal |
SMART - Difficult Cricothyrotomy
| Letter | Factor |
|---|---|
| S - Surgery | Prior surgery creating scarring/anatomic distortion |
| M - Mass | Abscess, hematoma over the anterior neck |
| A - Access/Anatomy | Obesity, edema, subcutaneous emphysema |
| R - Radiation | Radiation fibrosis |
| T - Tumor | Laryngeal or neck tumor |
Point-of-care ultrasound can identify and mark the cricothyroid membrane (CTM) preemptively in high-risk cases. - Rosen's Emergency Medicine, 9e
Step 2: Preoperative (or Pre-Intubation) Decision Framework
The ASA guidelines mandate consideration of four key questions:
- Assess likelihood and clinical impact of: difficult mask ventilation, difficult SGA placement, difficult laryngoscopy/intubation, difficult surgical airway
- Deliver supplemental oxygen continuously throughout all attempts
- Weigh relative merits of:
- Awake intubation vs. intubation after induction
- Noninvasive vs. invasive techniques
- Video laryngoscopy as the primary approach
- Preservation vs. ablation of spontaneous ventilation
- Develop primary AND rescue strategies before starting
Emergency Difficult Airway Algorithm (Rosen's/Walls)
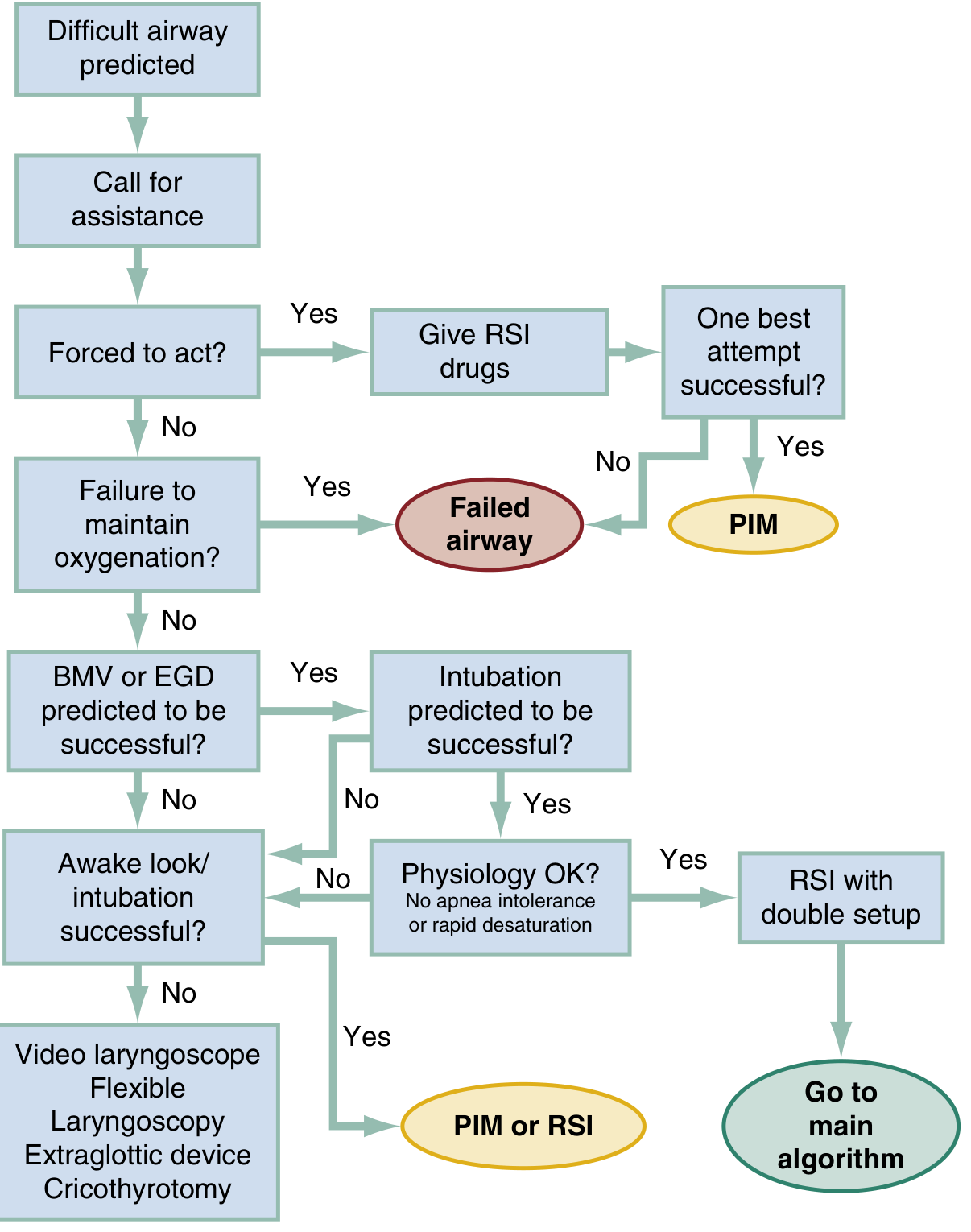
(Rosen's Emergency Medicine, 9e - Modified from Walls' Manual of Emergency Airway Management, 5e)
Key decision points:
1. Forced to act?
When impending arrest/obstruction means there is no time for an alternative approach (e.g., rapidly advancing angioedema, status asthmaticus about to arrest, premature extubation in a critically ill patient with a difficult airway): give RSI drugs and make the one best attempt with video laryngoscopy + optimal positioning. If successful → postintubation management (PIM). If not → declare failed airway.
2. Failure to maintain oxygenation?
If SpO₂ cannot be maintained → declare failed airway (see below).
3. BMV or EGD predicted to succeed?
If yes, and intubation predicted to succeed, and physiology OK (no apnea intolerance/rapid desaturation) → RSI with double setup (surgical airway immediately available). If physiology not OK → awake approach.
If BMV/EGD not predicted to succeed → awake look/intubation.
4. Awake intubation approach (when anatomy or physiology dictates against RSI):
- Video laryngoscopy awake
- Flexible laryngoscopy (fiberoptic bronchoscope)
- Extraglottic device
- Cricothyrotomy as last resort
DAS 2015 Algorithm (still widely used; 2025 update maintains this framework)
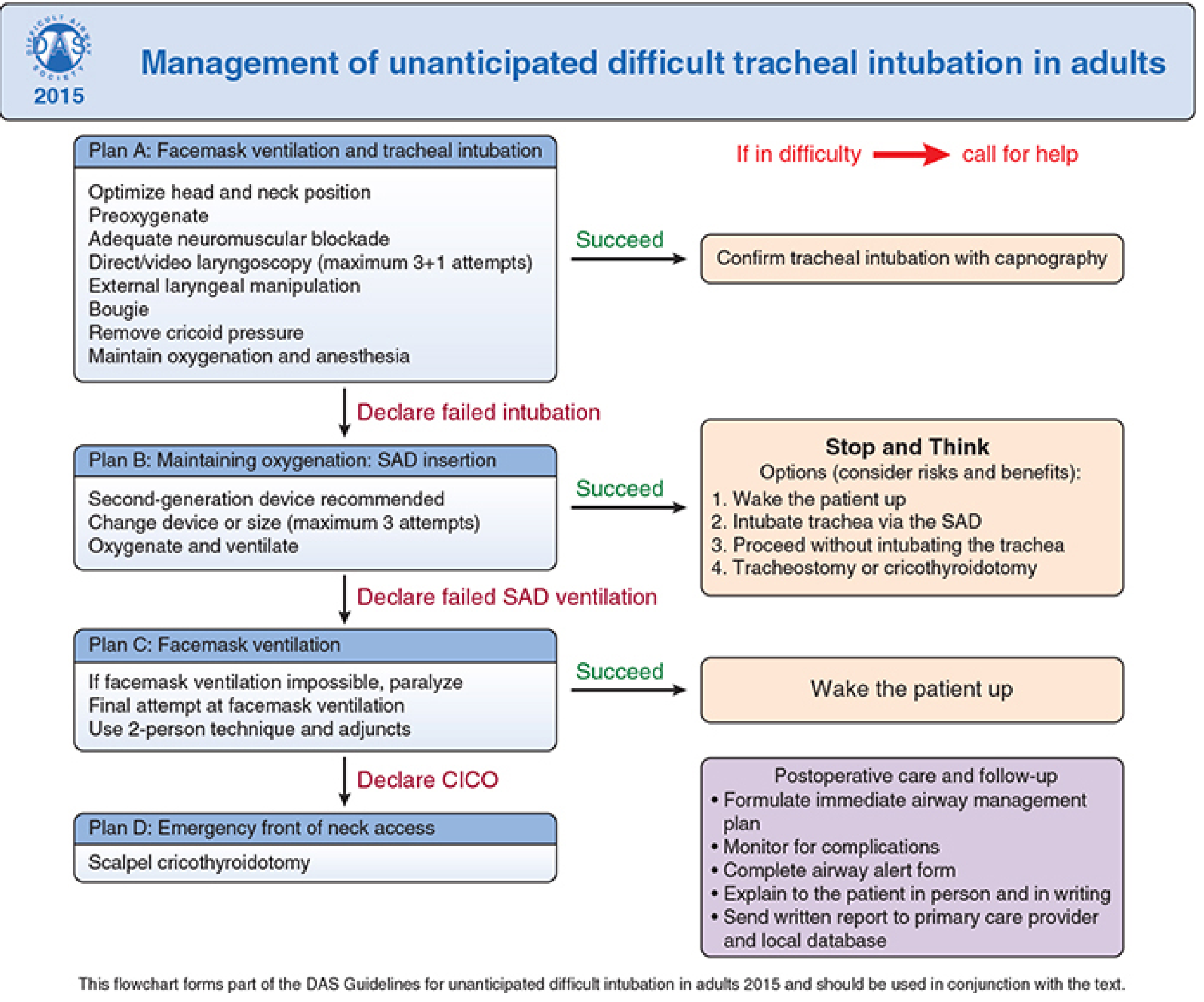
(DAS 2015 Guidelines - Frerk et al., Br J Anaesth 2015; framework retained in DAS 2025)
Plan A - Facemask Ventilation + Tracheal Intubation
- Optimize head/neck position; adequate NMB
- Direct or video laryngoscopy: maximum 3+1 attempts (3 by first operator, 1 by a more experienced colleague)
- Adjuncts: external laryngeal manipulation (BURP), bougie, remove cricoid pressure if impairing view
- Confirm tracheal intubation with waveform capnography
Declare failed intubation if Plan A unsuccessful → move to Plan B immediately
Plan B - Maintaining Oxygenation: SGA Insertion
- Insert a second-generation SGA (e.g., LMA Supreme, i-gel, ProSeal) - these have a gastric drainage channel
- Maximum 3 attempts; change device or size
- Oxygenate and ventilate
If successful: Stop and Think
- Wake the patient up
- Intubate via the SGA (with fiberscope)
- Proceed without intubating (if procedure can be done under SGA)
- Surgical airway (tracheostomy or cricothyrotomy)
Declare failed SAD ventilation if Plan B fails → Plan C
Plan C - Facemask Ventilation
- Final attempt at BMV (two-person technique, adjuncts: oral airway, nasal airway, jaw thrust)
- If face mask ventilation impossible: fully paralyze if not already done → final attempt
- If successful: wake the patient up
Declare CICO (Can't Intubate, Can't Oxygenate) if Plan C fails → Plan D
Plan D - Emergency Front-of-Neck Airway (FONA)
Scalpel cricothyrotomy is the preferred technique in a CICO emergency:
- Identify CTM by laryngeal handshake (feel: thyroid cartilage → gap → cricoid ring)
- Palpable CTM: Transverse stab incision through CTM → turn blade 90° (sharp edge caudally) → slide bougie along blade into trachea → railroad lubricated 6-mm cuffed tube → ventilate → confirm with capnography
- Impalpable CTM (obese, radiation, distorted): Vertical 8-10 cm skin incision (caudad to cephalad) → blunt dissection → identify/stabilize larynx → proceed as above
Post-FONA care: postpone elective surgery, urgent surgical review of cricothyrotomy site, document, complete airway alert form, explain to patient, send written report to GP.
DAS 2025 Guidelines - Key Updates (PMID 41203471)
Published January 2026 in the British Journal of Anaesthesia. 65 recommendations from a 3-year, 65-meeting process with systematic review of 1241 papers.
Key themes:
- Maintain the 4-plan linear algorithm (Plan A: intubation; Plan B: SGA; Plan C: face mask; Plan D: FONA)
- Prioritize continuous oxygen delivery throughout all steps
- Maximize first-attempt success rather than focusing on managing failure
- Waveform capnography is mandatory for confirming ventilation at every step
- New sections on: the physiologically difficult airway (RSI in haemodynamically unstable patients), obesity, human factors (communication, team dynamics), and point-of-care ultrasound for CTM identification
- Documentation and education: airway alert documentation, institutional training requirements
Awake Intubation
Indicated whenever there is a known or suspected difficult airway and it is safe to do so (cooperative patient, time available).
Preferred techniques:
- Awake flexible fiberoptic intubation (FOI) - gold standard for known difficult airway, distorted anatomy, unstable cervical spine
- Awake video laryngoscopy - increasingly used as equivalent to awake FOI in many centers
- Awake direct laryngoscopy - in experienced hands for partially difficult airways
Preparation for awake intubation:
- Antisialagogue: glycopyrrolate 0.2 mg IV or IM (reduces secretions, improves topical anesthetic contact)
- Topical anesthesia: 4% lidocaine spray or atomized nebulization of oropharynx, supraglottic structures, and below the vocal cords (transcricoid injection or spray-as-you-go via bronchoscope)
- Sedation (optional): low-dose midazolam, dexmedetomidine, or ketamine (carefully, to preserve spontaneous ventilation)
- Maximum safe lidocaine dose: 4-9 mg/kg topically (systemic absorption significantly less than IV)
Awake FOI is not appropriate when the patient is agitated/uncooperative, time is critically limited, or topical anesthesia cannot be achieved (e.g., allergic to local anesthetics).
Video Laryngoscopy (VL) in the Difficult Airway
VL is now recommended as the primary approach for anticipated difficult intubation in most guidelines. It provides:
- Magnified indirect glottic view that cannot be achieved with direct laryngoscopy
- Shared visualization for supervision and training
- Improved visualization in: obesity, limited mouth opening, limited neck mobility, anterior larynx
Hyperangulated VL blades (e.g., McGrath, GlideScope 60°) are best for visualization but may paradoxically make tube passage more difficult - use an appropriately shaped stylet.
Standard geometry VL blades (e.g., C-MAC, McGrath MAC) allow both indirect and direct viewing and facilitate tube passage.
VL should generally be avoided if the camera will be obscured by vomit or blood - use direct laryngoscopy in those cases.
"Physiologically Difficult Airway"
A concept increasingly recognized in DAS 2025 and ICU guidelines. Patients who are physiologically deranged (severe hypoxemia, haemodynamic instability, severe metabolic acidosis, right heart failure) are at extreme risk of peri-intubation cardiac arrest - even if anatomy is normal.
Key principles:
- Optimize physiology before intubation wherever possible (fluids, vasopressors, prone positioning for oxygenation, BiPAP pre-oxygenation)
- Choose ketamine as induction agent in hypotension
- Avoid propofol in hemodynamic instability
- Use push-dose epinephrine at the bedside before induction if severe hypotension
- Peri-intubation arrest is more preventable than it is treatable
Incidence Summary
| Situation | Incidence |
|---|---|
| Difficult DL (grade 3/4) in elective anesthesia | ~5% |
| Impossible mask ventilation | <0.5% |
| Failed intubation in elective anesthesia | 1:1000-2000 |
| Failed intubation in obstetrics | ~1:250 |
| CICO scenario | ~1:5,000-10,000 |
| Difficult emergency intubation | up to 10% |
Airway Equipment - Minimum Requirements for Difficult Airway Cart
- Video laryngoscope (hyperangulated and standard geometry blades)
- Flexible bronchoscope (fiberoptic)
- Second-generation SGAs (multiple sizes: i-gel, LMA Supreme)
- Intubating LMA (ILMA / Fastrach)
- Bougie (gum elastic bougie)
- Retrograde intubation kit
- Scalpel (#10 blade), bougie, and 6-mm cuffed ETT (for surgical airway)
- Cricothyrotomy kit (commercial or improvised)
- Transtracheal jet ventilation equipment
- Tube exchangers
Sources: Rosen's Emergency Medicine 9e; Morgan & Mikhail's Clinical Anesthesiology 7e; Sabiston Textbook of Surgery; Roberts & Hedges' Clinical Procedures in Emergency Medicine; Fishman's Pulmonary Diseases; DAS 2015 Guidelines (Frerk et al., Br J Anaesth 2015;115:827-848); DAS 2025 Guidelines (Ahmad et al., Br J Anaesth 2026, PMID 41203471)
This is a shared conversation. Sign in to Orris to start your own chat.