How dilutional hyponatremia occurs?
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive explanation of how dilutional hyponatremia occurs, drawn from authoritative nephrology and surgical textbooks.
Dilutional Hyponatremia — Mechanism
Definition and Core Concept
Dilutional hyponatremia is a form of hypo-osmotic hyponatremia where the serum sodium falls below 135 mmol/L not because sodium is lost, but because water is retained in excess, diluting the existing sodium content of the extracellular fluid (ECF). In contrast to depletional hyponatremia (where Na⁺ is actually lost), total body sodium in dilutional hyponatremia may be normal or even elevated — it is the water that is disproportionately increased.
"Changes in serum sodium concentration are inversely proportional to total body water (TBW). A low serum sodium level occurs when there is an excess of extracellular water relative to sodium." — Schwartz's Principles of Surgery
Pathophysiologic Mechanisms
1. Hypervolemic Dilutional Hyponatremia (most classic form)
This occurs in states of decreased effective circulating volume (ECV) despite a high total ECF volume — a paradox seen in:
- Congestive heart failure (CHF)
- Hepatic cirrhosis
- Nephrotic syndrome
- Advanced renal failure
The vicious cycle:
- Despite a high total ECF volume, the effective (circulating) blood volume is reduced — detected by baroreceptors in the aortic arch and carotid sinuses.
- Baroreceptors trigger the renin-angiotensin-aldosterone system (RAAS) → ↑ aldosterone → renal Na⁺ and water retention.
- Simultaneously, the low effective volume is a non-osmotic stimulus for ADH (vasopressin) release from the hypothalamus, even though osmolality is already low — this is the key pathologic step.
- Vasopressin acts on V2 receptors in the collecting duct, inserting aquaporin-2 (AQP2) channels → free water reabsorption.
- More water is retained → ECF expands further → Na⁺ is diluted further.
- This worsens hyponatremia while simultaneously failing to restore effective circulating volume, perpetuating the cycle.
In advanced renal failure, the mechanism is simpler: the kidneys cannot excrete water normally due to markedly reduced GFR, leading directly to water accumulation.
"When ECF is increased but the circulating blood volume is decreased, as occurs in hepatic cirrhosis, heart failure, and nephrotic syndrome, a vicious cycle is established. The decreased blood volume is sensed by baroreceptors and results in increased aldosterone and vasopressin, even though ECF volume is excessive." — Tietz Textbook of Laboratory Medicine, 7th Edition
2. Euvolemic Dilutional Hyponatremia
Here, the ECF volume appears clinically normal (no oedema), but water has been retained:
- SIADH (Syndrome of Inappropriate ADH Secretion): ADH is secreted "inappropriately" — independent of osmotic or volume stimuli — due to malignancies (e.g., small cell lung cancer), CNS disorders, pulmonary disease, or drugs (cyclophosphamide, vincristine). Vasopressin drives persistent water reabsorption → dilution of Na⁺.
- Primary polydipsia: Massive water intake overwhelms the kidney's capacity to excrete free water (normally up to ~28 L/day), diluting plasma Na⁺. Seen in psychiatric illness or hypothalamic disorders (sarcoidosis).
- Hypothyroidism: Impairs free water excretion.
- Adrenal insufficiency: ↑ CRH → stimulates vasopressin release.
3. Iatrogenic / Postoperative Dilutional Hyponatremia
- Postoperative state: Surgical stress causes a surge in ADH secretion, increasing collecting duct water reabsorption; if hypotonic IV fluids are given simultaneously, free water accumulates rapidly.
- Excessive hypotonic IV fluids: Directly increases TBW, diluting Na⁺.
- Drugs: Antipsychotics, tricyclic antidepressants, ACE inhibitors, and thiazide diuretics (thiazides specifically impair urinary dilution in the distal tubule, unlike loop diuretics which impair both dilution and concentration).
4. TURP Syndrome (specific surgical context)
During transurethral resection of the prostate (TURP), large volumes of hypotonic glycine irrigation fluid can be absorbed intravascularly → direct dilution of plasma Na⁺ → acute dilutional hyponatremia.
Why Symptoms Occur
CNS symptoms (confusion, seizures, coma) arise because hypo-osmolality causes water to shift into cells by osmosis, causing cerebral cell swelling. Symptoms correlate with the rate and severity of the fall in Na⁺ — acute hyponatremia is more dangerous than chronic, as the brain hasn't had time to compensate by extruding osmolytes.
Diagnostic Algorithm
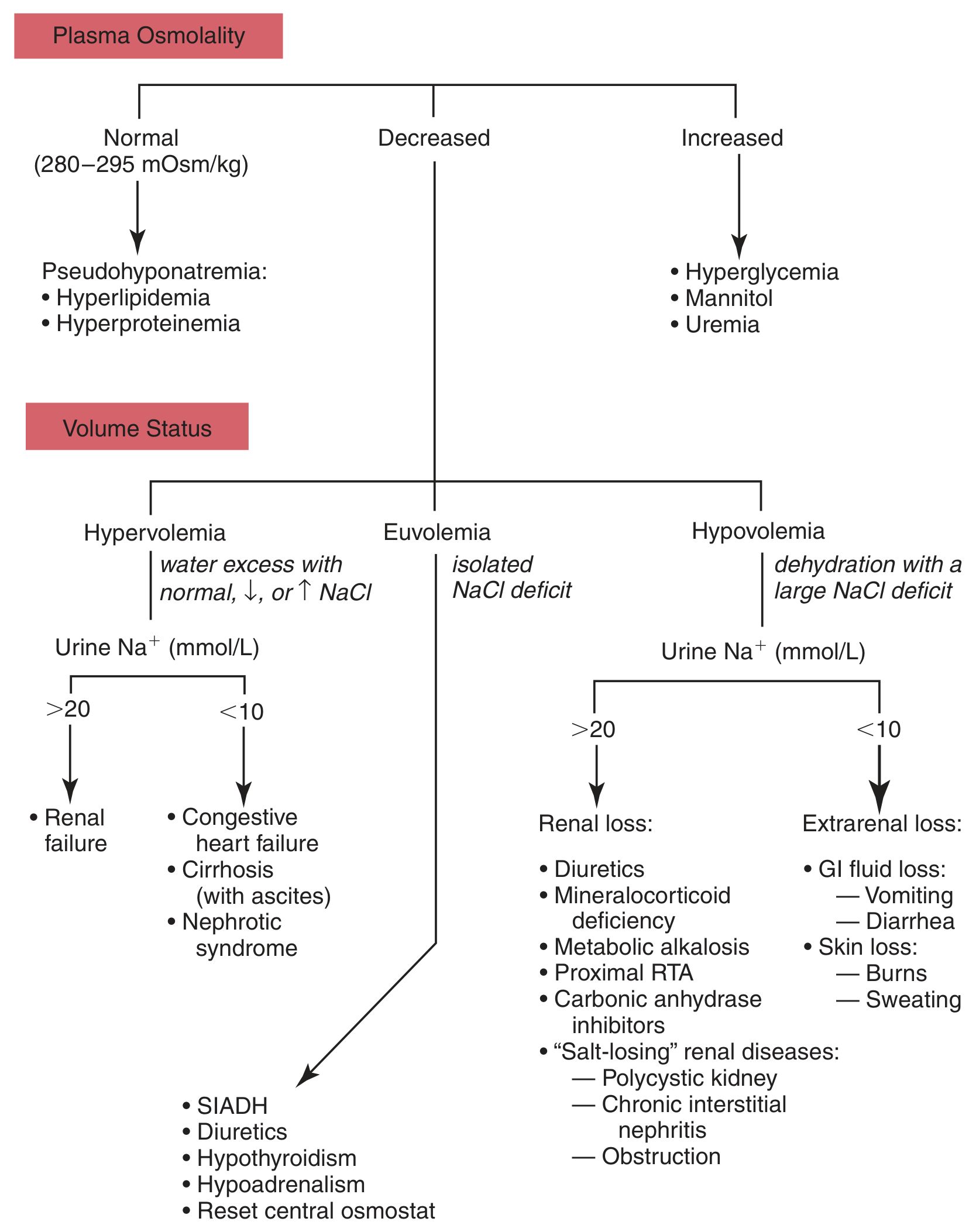
As the diagram shows, dilutional hyponatremia falls under decreased plasma osmolality + hypervolemia (urine Na⁺ <10 mmol/L in CHF/cirrhosis/nephrotic syndrome; >20 mmol/L in renal failure) or euvolemia (SIADH, diuretics, hypothyroidism, hypoadrenalism).
Summary Table
| Mechanism | Volume Status | Key Examples |
|---|---|---|
| ↓ Effective circulating volume → ↑ ADH + aldosterone | Hypervolemic | CHF, cirrhosis, nephrotic syndrome |
| ↓ GFR → impaired water excretion | Hypervolemic | Renal failure |
| Inappropriate ADH secretion | Euvolemic | SIADH, postoperative state |
| Excess water ingestion | Euvolemic | Primary polydipsia |
| Drug-induced water retention | Euvolemic | Thiazides, antipsychotics, TCAs |
| Direct fluid absorption | Acute | TURP syndrome |
Sources:
- Tietz Textbook of Laboratory Medicine, 7th Ed., pp. 1938–1939
- Schwartz's Principles of Surgery, 11th Ed., p. 114
- Brenner and Rector's The Kidney, 2-Volume Set, pp. 2280–2281
This is a shared conversation. Sign in to Orris to start your own chat.