facial nerve
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive information to provide a complete overview of the facial nerve. Let me compile this into a well-organized reference.
The Facial Nerve (Cranial Nerve VII)
Overview and Fiber Types
The facial nerve is the nerve of the second branchial arch and carries four functional fiber types:
| Fiber Type | Function | Target |
|---|---|---|
| Special visceral efferent (SVE) | Motor to muscles of facial expression | Mimetic muscles, stapedius, stylohyoid, posterior digastric |
| General visceral efferent (GVE) | Parasympathetic secretomotor | Lacrimal gland, submandibular + sublingual glands, nasal seromucinous glands |
| Special visceral afferent (SVA) | Taste | Anterior 2/3 of tongue (via chorda tympani), palate + tonsillar fossa (via GSPN) |
| General somatic afferent (GSA) | Cutaneous sensation + proprioception | External auditory canal, conchal skin, facial muscles |
The brainstem nuclei of origin are: motor nucleus (SVE), superior salivatory nucleus (GVE), and nucleus of the solitary tract (SVA/visceral afferent).
(Cummings Otolaryngology, p. 2451)
Course and Segments
The nerve travels through a bony canal - the fallopian canal - from the fundus of the internal auditory canal (IAC) to the stylomastoid foramen. It has five named segments:
1. Intracranial / Cisternal Segment
Exits the brainstem at the pontomedullary junction, travels with CN VIII to enter the internal auditory canal. Within the IAC the nerve lacks a fibrous sheath or endoneurium and is surrounded only by a thin arachnoid layer.
2. Labyrinthine Segment
- First, shortest, and narrowest segment of the fallopian canal
- Travels superior to the cochlea
- Opens into the geniculate fossa - site of the geniculate ganglion (cell bodies of sensory neurons)
- The overlying bone is dehiscent in ~25% of ears
- Most vulnerable to injury because: (a) narrowest lumen, (b) lacks epineurium, (c) is a watershed zone between the vertebrobasilar (labyrinthine a.) and external carotid (petrosal branch of middle meningeal a.) systems
- Surgical landmark: Bill's bar (vertical crest)
3. Tympanic (Horizontal) Segment
- Begins at the first genu where the nerve turns acutely posterior and slightly inferior at the geniculate ganglion
- Runs along the medial wall of the anterior attic, over the cochleariform process, and forms the superior wall of the oval window niche
- Most common site of congenital bony dehiscence, especially above the oval window
- Surgical landmarks: cochleariform process (transmastoid), supratubal recess
4. Mastoid (Vertical) Segment
- Begins at the second genu at the pyramidal eminence (anteroinferior to the lateral SCC)
- Gives off the chorda tympani (taste, anterior 2/3 tongue; parasympathetics to submandibular/sublingual glands) and stapedial branch at variable points
- The space between the mastoid segment and chorda tympani forms the facial recess (posterior tympanotomy)
- Surgical landmarks: pyramidal eminence, short process of incus, lateral SCC cortex, chorda tympani nerve
5. Extratemporal Segment
- Exits via the stylomastoid foramen (receives blood from the aponeurosis of the posterior digastric - this vascular relationship should be preserved during nerve rerouting)
- Enters the parotid gland, divides into upper and lower trunks
- Further branches and anastomoses within the parotid
(Cummings Otolaryngology, pp. 2450-2452)
Five Terminal Branches (TZBMC)
After exiting the parotid gland:
| Branch | Muscles Supplied |
|---|---|
| Temporal | Frontalis, orbicularis oculi (upper), corrugator |
| Zygomatic | Orbicularis oculi (lower), zygomaticus |
| Buccal | Buccinator, orbicularis oris, muscles of upper lip |
| Marginal Mandibular | Depressors of lower lip and chin |
| Cervical | Platysma |
The buccal branch closely accompanies the parotid duct (surface marking: tragus to midpoint between upper lip and alar base). Injuries lateral to a vertical line through the lateral canthus are surgically repairable.
(Gray's Anatomy for Students, p. 1052; Bailey & Love, p. 430)
Named Branches Within the Temporal Bone
- Greater superficial petrosal nerve (GSPN) - from geniculate ganglion; preganglionic parasympathetics to pterygopalatine ganglion → lacrimal gland + nasal glands; also carries taste from palate
- Nerve to stapedius - from mastoid segment; dysfunction causes hyperacusis
- Chorda tympani - from mastoid segment; taste anterior 2/3 tongue + preganglionic parasympathetics to submandibular ganglion → submandibular and sublingual glands
Surgical Landmarks by Segment
| Segment | Landmark |
|---|---|
| Labyrinthine | Vertical crest (Bill's bar) |
| Geniculate ganglion | Retrograde dissection of GSPN (middle fossa approach) |
| Tympanic | Cochleariform process; supratubal recess |
| Second genu | Oval window |
| Mastoid | Pyramidal eminence; bisects lateral SCC; short process of incus; chorda tympani |
| Stylomastoid foramen | Cephalic edge + aponeurosis of posterior digastric |
(Cummings Otolaryngology, Table 126.1)
Clinical Disorders
Bell Palsy (Idiopathic Facial Paralysis)
- Incidence: 23-37 per 100,000/year; peaks >65 years (59/100,000); bilateral in only 0.3%
- Diagnosis requires: (1) paresis of all muscle groups on one side, (2) sudden onset, (3) no CNS signs, (4) no ear/CPA disease
- Etiology: Reactivation of latent HSV-1 in the geniculate ganglion (best current evidence); HSV-1 DNA found in both trigeminal and geniculate ganglia at autopsy
- Pathology: Diffuse demyelination throughout intratemporal course; most severe at the labyrinthine segment and meatal foramen (Wallerian degeneration)
- Treatment: Corticosteroids (mainstay) ± antivirals
- Progressive facial paralysis is NOT Bell palsy - always image to exclude neoplasm
Ramsay Hunt Syndrome (Herpes Zoster Oticus)
- Caused by varicella zoster virus (VZV) reactivation
- Presents with facial palsy + vesicles in the ear canal/auricle (+ sometimes sensorineural hearing loss, vertigo)
- Treat with steroids + acyclovir
Differential Diagnosis of Facial Paralysis
Acute onset: Bell palsy, herpes zoster, Guillain-Barré, Lyme disease, otitis media (suppurative or cholesteatoma), trauma
Chronic/progressive: Facial neuroma (schwannoma), parotid malignancy with perineural invasion, cholesteatoma, meningioma
Bilateral facial paralysis suggests metabolic, autoimmune, or infectious disease (including Lyme disease).
Management Algorithm for Facial Paralysis
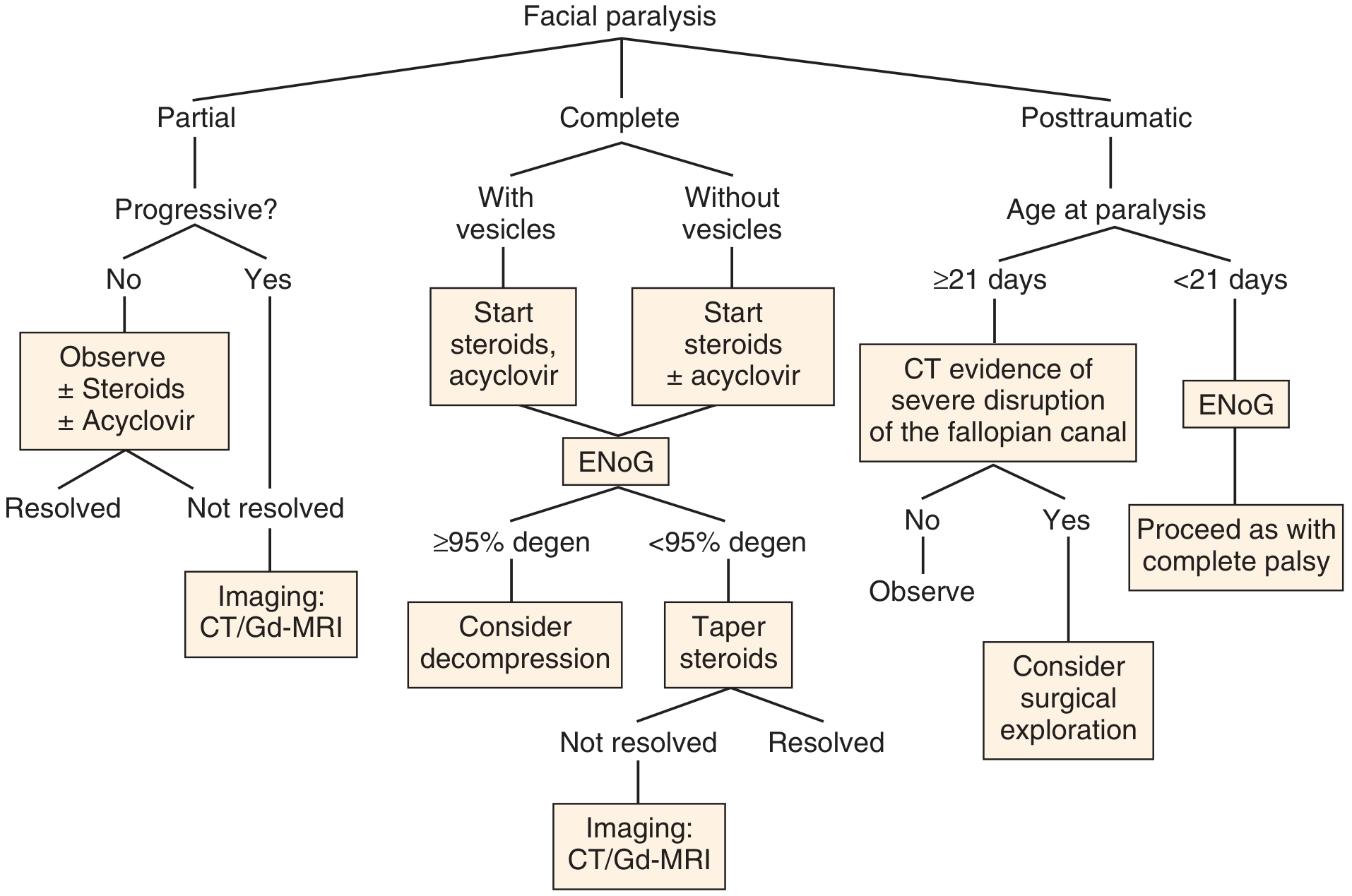
Fig. 172.1 - Management algorithm. Partial palsy: observe ± steroids; if progressive, image. Complete palsy: start steroids (+ acyclovir if vesicles present), then ENoG - if ≥95% degeneration, consider surgical decompression. Posttraumatic: ENoG within 21 days; CT if severe fallopian canal disruption, consider surgical exploration. (Cummings Otolaryngology)
Electrodiagnostic Testing
- Electroneuronography (ENoG): Compares compound action potential amplitudes side-to-side; ≥95% degeneration within 14 days of onset → threshold for considering decompression surgery
- Topodiagnostic tests: Schirmer test (lacrimal = GSPN), stapedial reflex (nerve to stapedius), taste testing / submandibular flow (chorda tympani) - useful for localizing level of lesion but accuracy is limited
Grading of Facial Palsy
The House-Brackmann scale (Grades I-VI) is the standard clinical grading system. Key parameters include absolute movement, eye closure, resting asymmetry, and degree of synkinesis. Progressive or recurrent palsy should prompt CT/gadolinium-MRI of the entire facial nerve from brainstem to parotid.
Key Vulnerabilities Summary
- Labyrinthine segment: Narrowest, no epineurium, watershed blood supply - most susceptible to inflammatory compression (Bell palsy, trauma)
- Geniculate ganglion: Thin/dehiscent bone, tethered by GSPN, in path of temporal bone fractures
- Tympanic segment: Most common site of congenital dehiscence; exposed by cholesteatoma
- Mastoid segment: Variable course especially with congenital anomalies; at risk in postauricular approaches
- Stylomastoid foramen: Superficially placed in neonates (underdeveloped mastoid tip) - vulnerable to forceps injury
(Sources: Cummings Otolaryngology Head and Neck Surgery; Gray's Anatomy for Students; Bailey and Love's Short Practice of Surgery, 28th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.