In ICU when cardiac patient come and we do ecg and check pulse so in which condition shock is given or not given with reason
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
I now have all the information needed for a thorough, structured answer. Let me compose it.
Here is a complete clinical guide on when to give shock (defibrillation/cardioversion) and when NOT to give shock in an ICU cardiac patient, based on ECG findings and pulse status.
Shock in ICU Cardiac Patients: When to Give and When NOT to Give
The single most important step before deciding on shock is the two-part assessment: ECG rhythm + pulse check. These two findings together determine everything.
The Core Concept: Shockable vs. Non-Shockable Rhythms
| ECG Rhythm | Pulse | Action | Type of Shock |
|---|---|---|---|
| Ventricular Fibrillation (VF) | No pulse | GIVE SHOCK | Defibrillation (unsynchronized) |
| Pulseless Ventricular Tachycardia (pVT) | No pulse | GIVE SHOCK | Defibrillation (unsynchronized) |
| VT with a pulse (unstable) | Has pulse | GIVE SHOCK | Cardioversion (synchronized) |
| SVT / AF / Atrial Flutter (unstable) | Has pulse | GIVE SHOCK | Cardioversion (synchronized) |
| Asystole (flat line) | No pulse | DO NOT SHOCK | CPR + drugs only |
| Pulseless Electrical Activity (PEA) | No pulse | DO NOT SHOCK | CPR + drugs only |
| Sinus Tachycardia | Has pulse | DO NOT SHOCK | Treat the cause |
| Any stable rhythm | Has pulse | DO NOT SHOCK | Monitor/medications |
GIVE SHOCK: Indications
1. Ventricular Fibrillation (VF) - Defibrillation Required
ECG: Chaotic, irregular, rapid electrical activity with no identifiable QRS complexes, P waves, or T waves. The waveform looks like a disorganized squiggly line.
Pulse: Absent (pulseless)
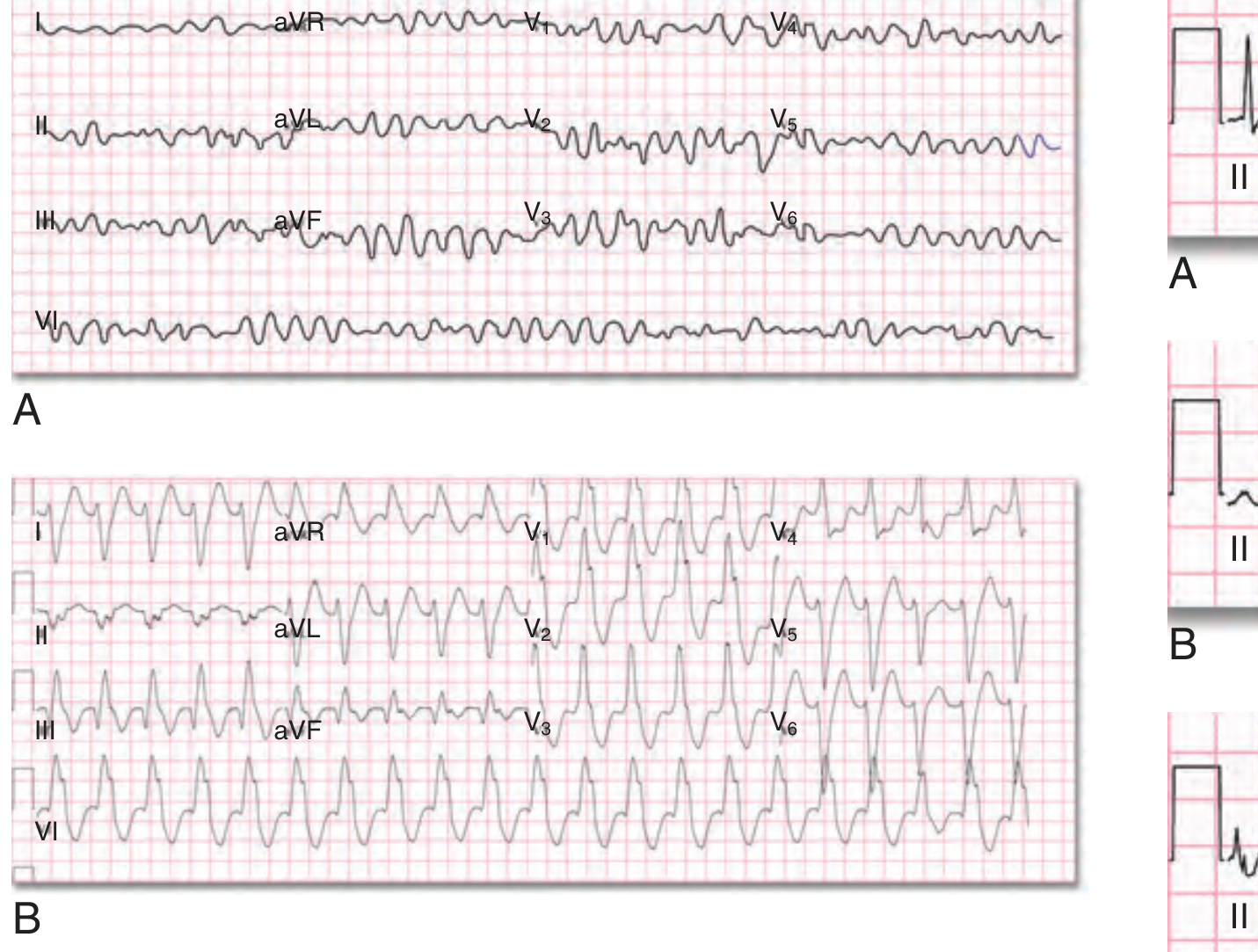
Why shock: VF is chaotic electromechanical activity in the ventricles - the heart cannot eject blood. Defibrillation passes a burst of current through the myocardium to simultaneously depolarize a critical mass of myocardial cells, interrupting the disorganized activity and allowing a normal pacemaker to take over. Every minute of VF without defibrillation reduces survival by ~10%. Immediate defibrillation in settings with <60-second response has >90% success.
Energy: Start at 200 J biphasic (adult). Biphasic waveforms are recommended as they are significantly more effective than monophasic at equivalent energies.
Mode: UNSYNCHRONIZED (because there is no QRS to synchronize to).
2. Pulseless Ventricular Tachycardia (pVT) - Defibrillation Required
ECG: Wide, regular, rapid QRS complexes (rate >100/min), often >150/min. QRS is broad (>0.12s). No identifiable P waves.
Pulse: Absent
Why shock: The ventricles are contracting so fast and ineffectively that they cannot generate a cardiac output. This is treated identically to VF - unsynchronized defibrillation is the priority. Do not delay for compressions once the defibrillator is charged.
3. VT with Pulse (Hemodynamically Unstable) - Synchronized Cardioversion
ECG: Same as VT pattern above (wide, rapid QRS)
Pulse: Present but patient is unstable (hypotension, altered consciousness, chest pain, pulmonary edema)
Why shock: The rhythm is too fast to maintain adequate cardiac output. Shock is given synchronized to the QRS complex to avoid delivering the shock during the vulnerable T-wave period (which could precipitate VF).
Energy: 100-200 J synchronized (adult)
4. Supraventricular Tachycardia (SVT), Atrial Fibrillation, Atrial Flutter (Unstable) - Synchronized Cardioversion
ECG:
- SVT: Narrow QRS, regular, rapid (150-220/min), no visible P waves
- AF: Irregularly irregular rhythm, no P waves, variable QRS rate
- Atrial Flutter: Sawtooth flutter waves at 300/min, ventricular rate often 150/min
Pulse: Present but patient is hemodynamically unstable
Why shock: When these arrhythmias cause hemodynamic compromise (BP drop, chest pain, altered consciousness), electrical cardioversion converts them to sinus rhythm faster and more reliably than drugs alone.
Important: For AF/flutter present >48 hours - risk of thrombus. In the ICU emergency setting, shock is not withheld for hemodynamic instability, but elective cardioversion requires anticoagulation for 3 weeks prior or TEE to rule out atrial thrombus.
DO NOT GIVE SHOCK: Contraindications
1. Asystole ("Flat Line") - NEVER Shock
ECG: No electrical activity. Flat or near-flat line. No QRS, no P waves.
Pulse: Absent
Why no shock: There is no electrical activity to "reset." Delivering a shock to asystole will not generate a rhythm - it only wastes time and delays CPR. Shocking asystole has zero benefit and is one of the most common errors in resuscitation. The treatment is immediate CPR + epinephrine + search for reversible causes (the "H's and T's").
Treatment: CPR, epinephrine 1 mg IV every 3-5 minutes, treat reversible causes.
2. Pulseless Electrical Activity (PEA) - NEVER Shock
ECG: Any organized electrical rhythm on monitor (may look like normal sinus, bradycardia, etc.)
Pulse: Absent (the heart is NOT mechanically contracting despite electrical activity)
Why no shock: The heart has electrical activity but is not pumping - there is a mechanical problem, not an electrical one. Examples include cardiac tamponade, tension pneumothorax, massive PE, hypovolemia. Shocking an organized rhythm will not fix this and may actually disrupt the existing organized rhythm.
Treatment: CPR, epinephrine, and aggressively identify and treat the underlying cause.
3. Sinus Tachycardia - NEVER Shock
ECG: Regular rhythm, normal P waves before every QRS, rate >100/min but usually <150/min
Pulse: Present
Why no shock: This is a normal physiologic response to an underlying problem (pain, fever, sepsis, hypovolemia, anemia, anxiety). Shocking it will not help and may harm. Treat the underlying cause.
4. Digitalis Toxicity + Cardioversion - Relative Contraindication
Cardioversion can precipitate life-threatening VT/VF in patients with digoxin toxicity. If cardioversion is absolutely necessary, start at the lowest possible energy.
5. Patient Has a Pulse + Stable Rhythm
If the patient is stable with any rhythm (even AF or VT), shock is not indicated immediately. Medical management, rate control, and monitoring are appropriate first steps.
Key Principle: The Two Questions to Ask Every Time
Question 1: Is there a pulse? Question 2: What does the ECG show?
No pulse + VF or VT on ECG → DEFIBRILLATE (unsynchronized, immediately)
No pulse + Asystole or PEA → CPR + DRUGS (never shock)
Has pulse + Unstable rhythm → CARDIOVERT (synchronized)
Has pulse + Stable rhythm → MEDICATIONS / monitor
Defibrillation vs. Cardioversion: The Key Difference
| Feature | Defibrillation | Cardioversion |
|---|---|---|
| Synchronization | Unsynchronized | Synchronized to QRS |
| Used for | VF, pulseless VT | VT with pulse, SVT, AF, flutter |
| Patient has pulse? | No | Usually yes (unstable) |
| Risk of inducing VF? | N/A (already no pulse) | Yes, if not synchronized |
"Cardioversion refers to shock delivery synchronized with the QRS complex... because a nonsynchronized shock coincident with the vulnerable period of the T wave may precipitate ventricular fibrillation." - Goldman-Cecil Medicine
Energy Settings (Adult, Biphasic Defibrillator)
| Indication | Energy |
|---|---|
| VF / pulseless VT | 200 J (subsequent: 200-360 J) |
| AF cardioversion | 120-200 J |
| Atrial flutter | 50-100 J |
| VT with pulse | 100-200 J |
| SVT | 50-100 J |
Sources:
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, Chapter 12 (Defibrillation and Cardioversion)
- Goldman-Cecil Medicine, Transthoracic Cardioversion and Defibrillation
- Tintinalli's Emergency Medicine, Chapter 109 (Cardioversion, Defibrillation, and Pacing)
- Braunwald's Heart Disease, 15th Edition (VF Management)
- Fuster and Hurst's The Heart, 15th Edition
Easy step to read ecg
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Here is a complete, easy step-by-step guide to reading an ECG, built from Harrison's, Costanzo Physiology, Kaplan & Sadock, Goldman-Cecil, and other authoritative textbooks.
Easy Steps to Read an ECG
First - Understand the Paper
The ECG paper is a grid. Every box has a meaning:
| Box | Width (time) | Height (voltage) |
|---|---|---|
| Small box | 0.04 seconds | 0.1 mV |
| Large box (5 small boxes) | 0.2 seconds | 0.5 mV |
| One full strip (10 seconds) | 50 large boxes | - |
Standard speed = 25 mm/sec. Standard calibration = 10 mm = 1 mV (you will see a calibration pulse at the start).
The Normal ECG Waveform - Know Each Part

| Wave / Segment | What it Represents |
|---|---|
| P wave | Atrial depolarization (atria contracting) |
| PR interval | Time from atria firing to ventricles firing (AV node conduction) |
| QRS complex | Ventricular depolarization (ventricles contracting) |
| ST segment | Ventricles fully depolarized (isoelectric normally) |
| T wave | Ventricular repolarization (ventricles resetting) |
| QT interval | Total ventricular electrical activity (depolarization + repolarization) |
| U wave | Seen after T wave, represents late repolarization of Purkinje fibers |
The 12 Leads - What They Look At
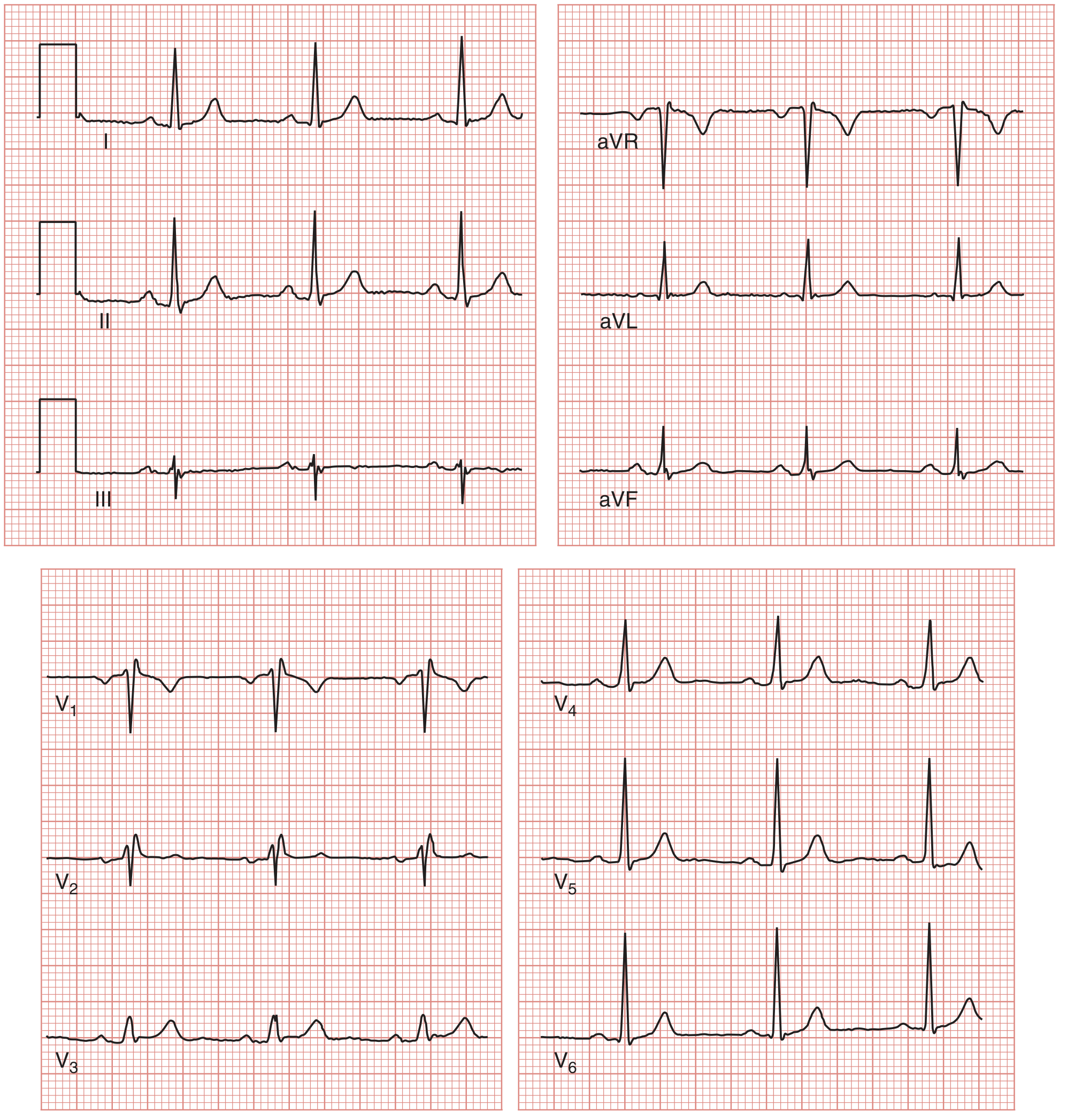
The 12 leads are like 12 cameras placed around the heart:
Limb Leads (look at heart from front):
- I, II, III - Standard limb leads
- aVR, aVL, aVF - Augmented limb leads
Chest Leads (look at heart from front to back):
- V1, V2 - Right ventricle
- V3, V4 - Septum/anterior wall
- V5, V6 - Left ventricle (lateral wall)
Lead II is the best single lead for rhythm analysis (it runs parallel to the heart's electrical axis).
8 Easy Steps - The Systematic Approach
(Harrison's Principles of Internal Medicine recommends analyzing 14 parameters in every ECG - here simplified into 8 practical steps)
STEP 1 - Check Calibration & Technical Quality
- Look for the calibration pulse at the left edge: should be 10 mm tall = 1 mV
- Check all 12 leads are present and not inverted/swapped
- Look for artefact (patient movement, poor electrode contact)
- If limb leads are inverted or leads look wrong, check electrode placement before interpreting
STEP 2 - Calculate Heart Rate
Method 1: The 300 Rule (for regular rhythms)
- Count the number of large boxes between two R waves
- Divide 300 by that number
| Large boxes between R-R | Heart Rate |
|---|---|
| 1 box | 300/min |
| 2 boxes | 150/min |
| 3 boxes | 100/min |
| 4 boxes | 75/min (normal) |
| 5 boxes | 60/min |
| 6 boxes | 50/min |
Memory trick: 300 - 150 - 100 - 75 - 60 - 50
Method 2: Count QRS complexes (for irregular rhythms like AF)
- Count QRS complexes in the 10-second strip
- Multiply by 6 = rate per minute
Normal heart rate = 60-100 bpm
- <60 = Bradycardia
-
100 = Tachycardia
STEP 3 - Check Rhythm (Regular or Irregular?)
- Is the R-R interval the same throughout? Use a paper/ruler to check
- Regular: all R-R intervals are equal
- Regularly irregular: a pattern (e.g., every 3rd beat drops)
- Irregularly irregular: no pattern at all (classic = Atrial Fibrillation)
Ask: Is there a P wave before every QRS? Is there a QRS after every P wave?
| Finding | Meaning |
|---|---|
| P before every QRS, regular | Sinus rhythm (normal) |
| No P waves, irregular rhythm | Atrial Fibrillation |
| Sawtooth waves, rate ~300 | Atrial Flutter |
| P waves present but some QRS dropped | Heart Block |
| Wide bizarre QRS, no P wave | Ventricular rhythm |
STEP 4 - Measure the Intervals
PR Interval (from start of P to start of QRS)
- Normal: 0.12 - 0.20 seconds (3-5 small boxes)
- Short PR (<0.12 sec): WPW syndrome, junctional rhythm
- Long PR (>0.20 sec): 1st degree heart block (AV delay)
- PR gets longer until a QRS drops: 2nd degree block (Wenckebach)
- No relationship between P and QRS: 3rd degree (complete) heart block
QRS Duration (width of the QRS complex)
- Normal: <0.12 seconds (<3 small boxes)
- Narrow QRS (<0.12): Normal conduction through His-Purkinje
- Wide QRS (>0.12): Bundle branch block, ventricular rhythm, hyperkalemia, drugs
QT Interval (from start of QRS to end of T wave)
- Normal: <0.44 sec in men, <0.46 sec in women (rate-dependent)
- Prolonged QT: Risk of Torsades de Pointes (life-threatening VT)
- Causes of long QT: drugs (quinidine, amiodarone, haloperidol), hypokalemia, hypomagnesemia, congenital LQTS
STEP 5 - Determine the Axis
The axis is the net direction of ventricular depolarization. Use Lead I and aVF:
| Lead I | aVF | Axis | What it means |
|---|---|---|---|
| Positive (upright) | Positive (upright) | Normal (-30 to +90°) | Normal heart position |
| Positive | Negative | Left axis deviation (<-30°) | LVH, left anterior fascicular block, inferior MI |
| Negative | Positive | Right axis deviation (>+90°) | RVH, LBBB, lateral MI, pulmonary hypertension |
| Negative | Negative | Extreme axis | Severe pathology |
Quick trick: If I and aVF are both pointing UP = NORMAL AXIS. Think of it as both thumbs up.
STEP 6 - Examine the P Wave
- Normal P wave: Upright in leads I, II, aVF; inverted in aVR
- Peaked/tall P (>2.5mm in II): Right atrial enlargement ("P pulmonale")
- Broad/notched P (>0.12 sec in II): Left atrial enlargement ("P mitrale")
- Absent P waves: AF, junctional rhythm, sinoatrial block
- Inverted P in II: Ectopic atrial rhythm or junctional rhythm
STEP 7 - Look at the QRS Complex
Check for:
1. Pathological Q waves
- Small Q waves in lateral leads are normal
- Pathological Q: width >0.04 sec OR depth >25% of the R wave
- Presence = old MI (dead tissue does not depolarize)
- Location tells you which artery was blocked:
| Leads with Q waves | Territory | Artery |
|---|---|---|
| II, III, aVF | Inferior | RCA |
| V1-V4 | Anterior | LAD |
| I, aVL, V5-V6 | Lateral | LCx |
2. R-wave progression in chest leads
- R wave should grow from V1 to V5 (small in V1, tall in V5-V6)
- Poor R-wave progression = anterior MI or LBBB
3. Bundle Branch Block (BBB)
- QRS >0.12 sec (wide)
- RBBB: "RSR' pattern" (rabbit ears) in V1; wide S in V5-V6. Think: "WiLLiaM MaRRoW" - W in V1 and M in V6 = LBBB; M in V1 and W in V6 = RBBB
4. Voltage (hypertrophy)
- LVH: S in V1 + R in V5 or V6 >35 mm (Sokolow-Lyon criteria)
- RVH: Tall R in V1, right axis deviation
STEP 8 - Examine ST Segment and T Waves
This is the most clinically urgent step in the ICU.
Normal ST segment: Flat (isoelectric), at the baseline
ST Elevation - EMERGENCY
- >1mm in 2+ contiguous limb leads OR >2mm in 2+ chest leads
- Causes:
- STEMI (ST elevation MI) - convex/tombstone shape
- Pericarditis - saddle-shaped, widespread leads, no reciprocal changes
- Prinzmetal angina (coronary spasm)
- Benign early repolarization (young, athletic patients)
ST Depression - URGENT
- Subendocardial ischemia / NSTEMI
- Digoxin effect (downsloping "sagging" depression)
- Reciprocal change (opposite to ST elevation area)
T Wave Changes
- Inverted T waves: Ischemia, LVH strain, bundle branch block, PE
- Peaked/tall T waves: Hyperkalemia (early), hyperacute STEMI
- Flat T waves: Hypokalemia, ischemia
Hyperacute STEMI Sequence to Remember:
Peaked T → ST elevation → Q wave develops → T inversion → ST normalizes → Q wave persists
Quick Summary Cheat Sheet
STEP 1 → Check calibration and lead quality
STEP 2 → Heart rate (300 ÷ large boxes between R-R)
STEP 3 → Rhythm (regular? P before every QRS?)
STEP 4 → Intervals (PR, QRS, QT)
STEP 5 → Axis (Lead I + aVF)
STEP 6 → P wave (shape, size, presence)
STEP 7 → QRS (Q waves, BBB, voltage, R progression)
STEP 8 → ST segment + T waves (most urgent in ICU!)
Normal Values at a Glance
| Parameter | Normal Value |
|---|---|
| Heart rate | 60-100 bpm |
| PR interval | 0.12-0.20 sec (3-5 small boxes) |
| QRS duration | <0.12 sec (<3 small boxes) |
| QT interval | <0.44 sec (men), <0.46 sec (women) |
| P wave duration | <0.12 sec |
| P wave height | <2.5 mm |
| Axis | -30° to +90° |
| ST segment | Isoelectric (flat at baseline) |
Sources:
- Harrison's Principles of Internal Medicine, 22nd Edition - Clinical Interpretation of the ECG
- Costanzo Physiology, 7th Edition - Electrocardiogram
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry - ECG Basics
- Medical Physiology (Boron & Boulpaep) - ECG intervals and waveforms
This is a shared conversation. Sign in to Orris to start your own chat.