Nephrotic syndrome
Reading File
Finding Sources
Searching PubMed
"nephrotic syndrome"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
I now have enough material for a thorough, well-structured answer. Let me compile it.
Nephrotic Syndrome
Definition
Nephrotic syndrome is defined by the tetrad of:
- Massive proteinuria - >3.5 g/day in adults (>40 mg/m²/hr in children)
- Hypoalbuminemia - serum albumin <3 g/dL (typically <2.5 g/dL)
- Generalized edema (anasarca)
- Hyperlipidemia and lipiduria
A spot urine protein:creatinine ratio correlates with 24-hour proteinuria and is a practical bedside substitute for timed collections.
- Robbins Pathologic Basis of Disease, p. 844
- Frameworks for Internal Medicine, p. 464
Pathophysiology
Proteinuria
The glomerular capillary wall normally acts as a combined size and charge barrier, maintained by the glomerular basement membrane (GBM), fenestrated endothelium, and podocytes (foot processes coated with polyanionic proteins). In nephrotic syndrome, structural or physicochemical disruption of this barrier - particularly podocyte injury - increases permeability, allowing plasma proteins (primarily albumin) to escape into urine.
Hypoalbuminemia
Urinary albumin losses deplete serum albumin faster than hepatic synthesis can compensate. Increased renal catabolism of filtered albumin also contributes.
Edema - "Underfill" vs. "Overfill"
Two competing mechanisms:
| Feature | Underfill (classic) | Overfill |
|---|---|---|
| Trigger | Low oncotic pressure from hypoalbuminemia → fluid shifts to interstitium | Primary renal Na⁺ retention |
| Plasma volume | Contracted | Expanded |
| PRA / aldosterone | ↑↑ | ↓ |
| ANP | ↓ | ↑ |
| Typical disease | Minimal change disease | FSGS, membranous |
| Diuretic risk | Azotemia, electrolyte disturbances | Less |
The diagram below illustrates the divergence between these groups:
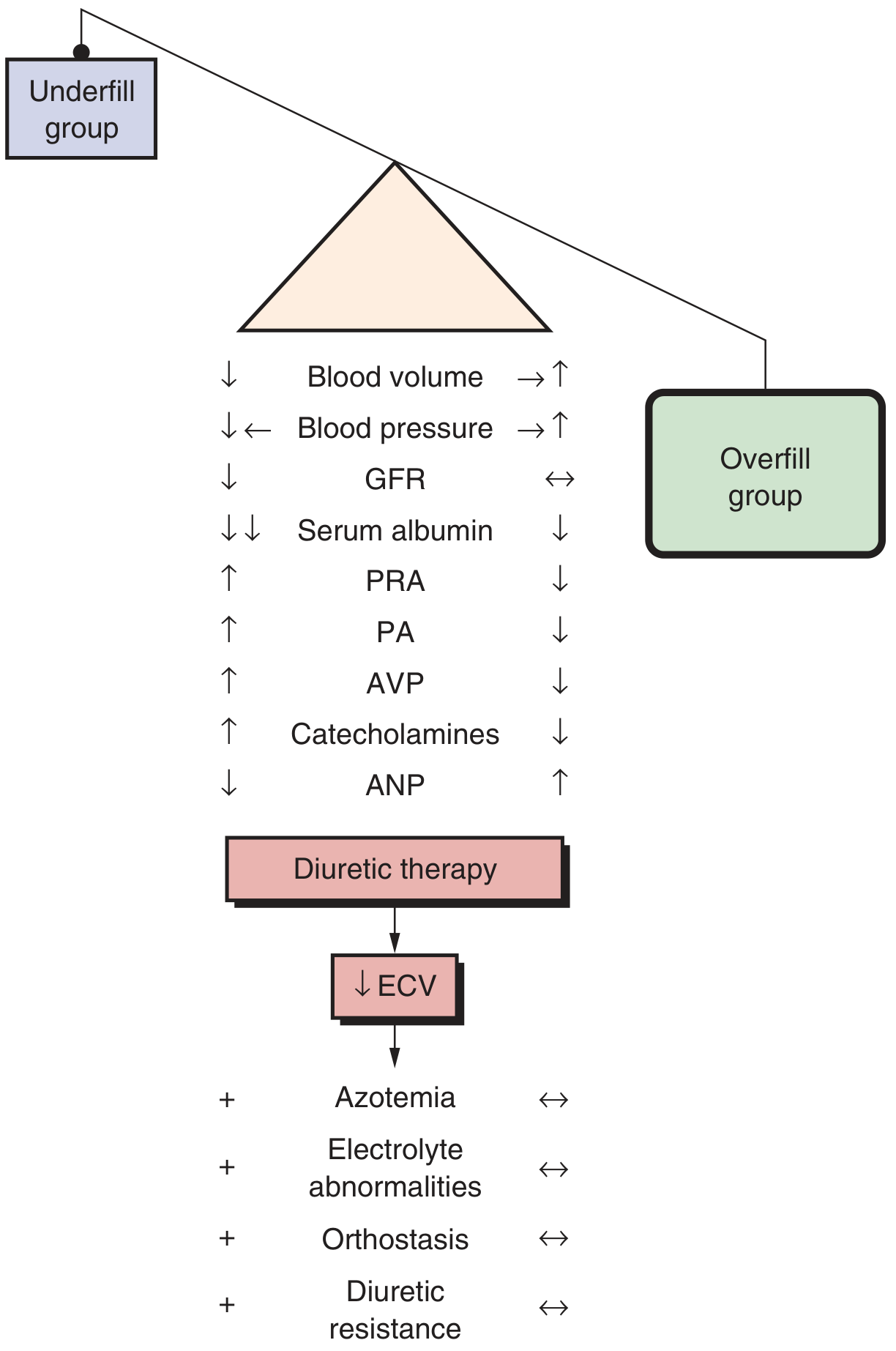
Sodium and water retention is further driven by hyperaldosteronism (from hypovolemia-driven renin secretion), sympathetic activation, and reduced atrial natriuretic peptide secretion.
Hyperlipidemia and Lipiduria
- ↑ hepatic lipoprotein synthesis (compensatory response to low oncotic pressure)
- Abnormal transport of circulating lipid particles
- ↓ lipid catabolism
- Results in ↑ cholesterol, triglycerides, VLDL, LDL, Lp(a); ↓ HDL in some cases
- Lipoproteins also leak across the glomerular wall → lipiduria (free fat, oval fat bodies, fatty casts)
Complications
Thromboembolism - Urinary loss of antithrombotic factors (antithrombin III, proteins C and S) combined with increased hepatic production of procoagulant factors (fibrinogen, factor V, factor VIII) creates a prothrombotic state. The most common sites are the renal veins and deep veins of the lower extremities. Membranous nephropathy carries the highest thrombotic risk.
Infections - Loss of IgG in urine, reduced complement activity, and diminished T-cell function predispose to infections, especially with encapsulated organisms (Streptococcus pneumoniae, Staphylococcus aureus).
Protein selectivity - "Highly selective" proteinuria = mostly low-molecular-weight proteins (albumin, transferrin) - seen in minimal change disease. "Poorly selective" = higher-molecular-weight globulins also excreted.
Causes
Primary (Idiopathic) Glomerular Diseases
| Disease | Children (%) | Adults (%) | Notes |
|---|---|---|---|
| Minimal change disease | 75 | 8 | Most common in children |
| Focal segmental glomerulosclerosis | 10 | 35 | Most common in adults overall; highest in Black patients |
| Membranous nephropathy | 3 | 30 | Most common in older White adults |
| MPGN / dense deposit disease | 10 | 10 | Mixed nephrotic/nephritic |
| Other (IgA, focal proliferative) | 2 | 17 | - |
Primary disease accounts for ~95% of nephrotic syndrome in children, ~60% in adults.
Secondary Causes (~40% of adults)
- Diabetes mellitus (Kimmelstiel-Wilson nodular glomerulosclerosis)
- Amyloidosis (AL > AA)
- SLE (membranous pattern, Class V lupus nephritis)
- Drugs: NSAIDs, gold, penicillamine, heroin, captopril
- Infections: hepatitis B and C, HIV, malaria, syphilis, schistosomiasis
- Malignancy: carcinoma of lung/colon, melanoma, lymphoma (especially Hodgkin's with MCD)
- Preeclampsia (pregnancy-related)
- Endocarditis / shunt nephritis
Major Primary Glomerular Diseases in Detail
1. Minimal Change Disease (MCD)
- Demographics: #1 cause in children; also in adults (associated with NSAIDs, lymphoma/Hodgkin's)
- Pathogenesis: Systemic factor (likely T-cell derived) causing podocyte injury and effacement of foot processes; no immune complex deposition
- Light microscopy: Normal glomeruli
- Immunofluorescence: Negative
- Electron microscopy: Diffuse effacement (fusion) of podocyte foot processes - pathognomonic
- Clinical: Highly selective proteinuria; rapid onset; responds well to steroids
- Treatment: Corticosteroids - >80% remission rate; relapses are common; some become steroid-dependent or resistant
2. Focal Segmental Glomerulosclerosis (FSGS)
- Demographics: #1 in Black patients (APOL1 high-risk alleles); occurs at all ages
- Variants: Primary (idiopathic), secondary (reduced renal mass, obesity, HIV, COVID-19 - collapsing variant), genetic
- Pathogenesis: Podocyte injury and loss → denuded GBM → protein accumulation in mesangium → mesangial proliferation → progressive sclerosis. A vicious cycle of nephron loss drives further compensatory hyperfiltration and injury.
- Light microscopy: Segmental sclerosis (collapse, matrix deposition, hyalinosis, foamy macrophages) in a focal distribution - biopsy may miss involved glomeruli
- EM: Diffuse foot process effacement in primary FSGS; focal in secondary
- Clinical: Often poorly selective proteinuria; hypertension common; higher risk of progression to ESRD; highest thromboembolic risk among primary nephropathies
- Treatment: Steroids (less responsive than MCD); calcineurin inhibitors (tacrolimus/cyclosporine); RAS blockade for secondary FSGS; SGLT2 inhibitors for proteinuria reduction
3. Membranous Nephropathy (MN)
- Demographics: Most common primary nephrotic syndrome in older White adults; bimodal age distribution
- Pathogenesis: Immune complex-mediated - antibodies against podocyte surface antigens form subepithelial deposits:
- Anti-PLA2R (M-type phospholipase A2 receptor) - ~60% of primary MN; clinically useful biomarker
- Other antigens: THSD7A, NELL1, EXT1/2, NCAM1
- IgG4 is the predominant subclass (poor classical complement activator)
- Complement activation (C5b-9 membrane attack complex) causes podocyte injury
- Light microscopy: Diffuse thickening of capillary walls; "spike and dome" pattern on silver stain
- EM: Subepithelial electron-dense deposits
- IF: Granular IgG and C3 along capillary walls
- Clinical: Insidious onset; "rule of thirds" - one-third remit spontaneously, one-third stable/partial remission, one-third progress to ESRD
- Treatment: ACE inhibitor/ARB (first-line); immunosuppression for high-risk disease (cyclophosphamide + steroids [Ponticelli protocol]; rituximab increasingly preferred)
Diagnosis and Workup
- Urine: Spot protein:creatinine ratio (correlates with 24-hr collection), urinalysis (oval fat bodies, fatty casts, lipid droplets), urine electrophoresis
- Blood: Serum albumin, lipid panel, creatinine, CBC, complement (C3/C4 for secondary causes)
- Serology for secondary causes: ANA, anti-dsDNA (SLE), HBsAg/HCV Ab, HIV, serum PLA2R antibodies (MN), SPEP (amyloid/myeloma), blood glucose/HbA1c
- Renal biopsy: Indicated in adults (to determine cause and guide treatment); generally NOT required in children with classic presentation (presumed MCD, try steroids first)
Management
General Measures
- Edema: Loop diuretics (furosemide); note that hypoalbuminemia reduces furosemide binding to plasma proteins, enlarging its volume of distribution and sometimes causing resistance. In the underfill group, aggressive diuresis risks azotemia - use cautiously.
- Proteinuria reduction: ACE inhibitors or ARBs - reduce proteinuria, slow disease progression, and address coagulopathy and dyslipidemia. Adding a loop diuretic to ACE-I/ARB further reduces proteinuria.
- Hyperlipidemia: Statins
- Thromboembolism prophylaxis: Anticoagulation considered when serum albumin <2 g/dL, particularly in membranous nephropathy or when albumin is very low
- Infection prevention: Pneumococcal vaccination; prophylactic penicillin in children
Disease-Specific Therapy
| Disease | First-line | Second-line |
|---|---|---|
| MCD (adults) | Prednisone | Cyclosporine, tacrolimus, rituximab |
| MCD (children) | Prednisone | Cyclophosphamide, levamisole, rituximab |
| FSGS (primary) | High-dose prednisone | Calcineurin inhibitors, rituximab |
| Membranous nephropathy | ACE-I/ARB + observation (low risk) | Rituximab or cyclophosphamide/steroids (high risk) |
| Secondary FSGS | Treat underlying cause + RAS blockade | SGLT2 inhibitors |
Recent Evidence (2025-2026)
A 2025 Cochrane review (PMID 40337980) evaluated interventions for idiopathic steroid-resistant nephrotic syndrome in children, and a 2026 systematic review (PMID 41843217) found that rituximab-induced hypogammaglobulinemia is a significant concern in childhood nephrotic syndrome, warranting immunoglobulin monitoring. A 2025 meta-analysis (PMID 41357184) characterized the histopathological subtypes in steroid-resistant nephrotic syndrome in children (FSGS predominates).
Sources: Robbins & Cotran Pathologic Basis of Disease, pp. 843-847 | Brenner and Rector's The Kidney | Frameworks for Internal Medicine, pp. 463-465 | NKF Primer on Kidney Diseases, 8e
This is a shared conversation. Sign in to Orris to start your own chat.