Hydrocephalus
Reading File
Finding Sources
Searching PubMed
hydrocephalus
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
I now have rich, comprehensive content from multiple authoritative sources. Let me compose the full answer.
Hydrocephalus
Definition
Hydrocephalus is a pressure-dependent enlargement of the cerebral ventricles resulting from an imbalance between CSF production and absorption - most commonly due to obstruction of CSF flow or impaired resorption, and rarely due to overproduction. The word literally means "water on the brain," though it is a nonspecific term that must be distinguished from ventriculomegaly caused by brain atrophy (hydrocephalus ex vacuo).
- Bradley and Daroff's Neurology in Clinical Practice, p. 1853
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1149
Pathophysiology and CSF Circulation
CSF is produced by the choroid plexuses within the ventricles. It circulates from the lateral ventricles → third ventricle → cerebral aqueduct of Sylvius → fourth ventricle → exits via the foramina of Magendie (midline) and Luschka (lateral) into the subarachnoid space → bathes the cerebral convexities → absorbed primarily by the arachnoid granulations. Cerebrovascular pulsations also influence net CSF flow. Overproduction (e.g., choroid plexus papilloma) is a rare cause.
When outflow is obstructed, increased CSF volume expands the ventricles and can elevate intracranial pressure (ICP). In acute noncommunicating hydrocephalus, 80% of maximal ventricular enlargement occurs within the first 6 hours. Continued CSF production despite obstruction leads to periventricular interstitial (transependymal) edema as fluid leaches through the ependymal lining into surrounding white matter.
Classification
| Type | Mechanism | Site of Obstruction |
|---|---|---|
| Noncommunicating (obstructive) | Intraventricular block; ventricles not in continuity with subarachnoid space | Aqueduct of Sylvius, foramina of Monro, 4th ventricle outflow |
| Communicating | Ventricular system remains patent; block is extraventricular in subarachnoid space | Arachnoid granulations, basal cisterns |
| Hydrocephalus ex vacuo | Compensatory enlargement due to loss of brain parenchyma (atrophy) | Not a true obstruction |
| Overproduction (rare) | Excess CSF production | Choroid plexus papilloma/carcinoma |
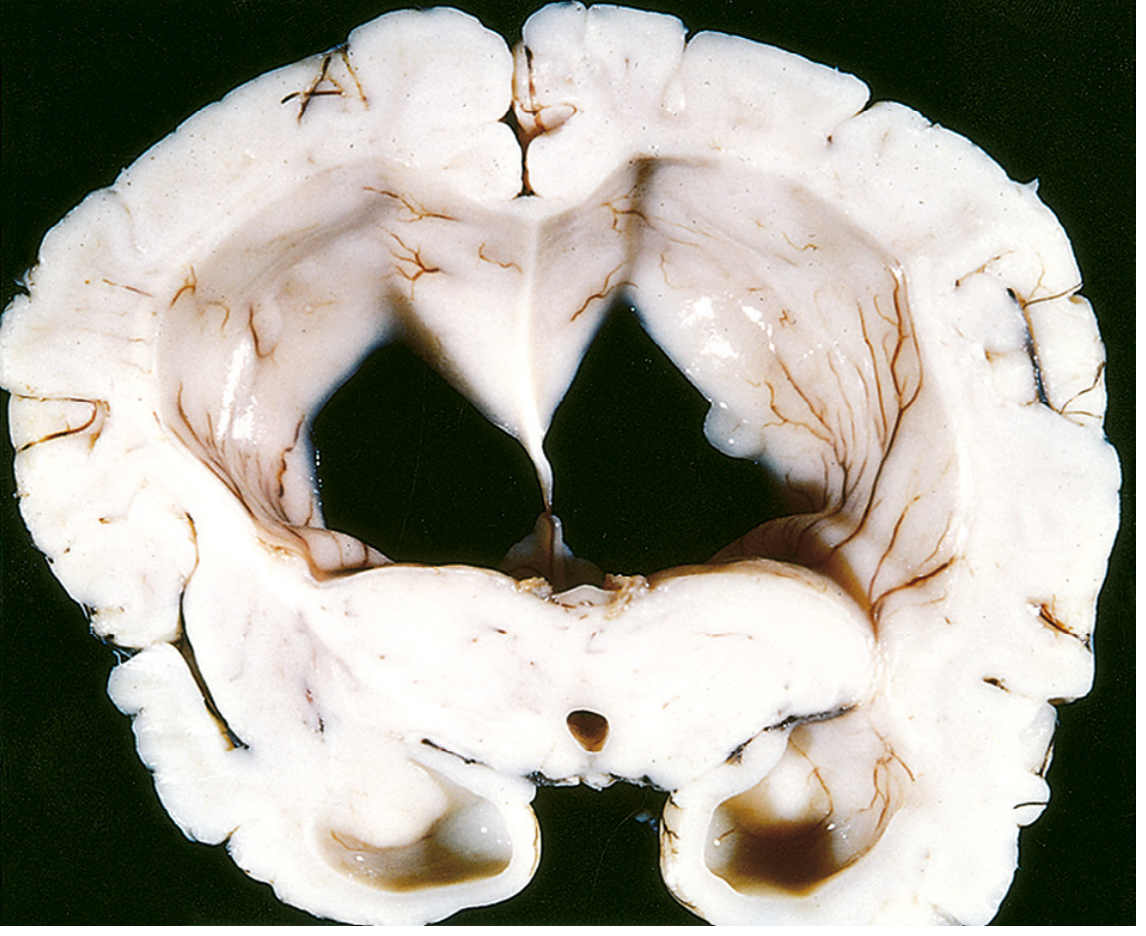
Gross Pathology
The classic appearance is massively dilated lateral ventricles with thinned surrounding white matter:
Causes by Age Group
Neonates and Infants
- Intrauterine infections causing aqueductal stenosis/gliosis (most common congenital cause)
- Chiari II malformation (associated with lumbosacral myelomeningocele)
- Dandy-Walker malformation (atresia of foramen of Magendie/Luschka)
- Posthemorrhagic hydrocephalus (intraventricular hemorrhage - especially in preterm infants <1500 g; ~25% develop progressive ventricular enlargement)
- Post-infective (bacterial meningitis causing meningeal scarring)
- Congenital midline tumors; vein of Galen malformations
Older Children
- Posterior fossa neoplasms (medulloblastoma, astrocytoma)
- Aqueductal stenosis
- Chiari I malformation
Adults
- Colloid cyst of the third ventricle (ball-valve mechanism causing intermittent acute obstruction)
- Cerebellar hemorrhage or infarct with edema compressing the aqueduct
- Post-subarachnoid hemorrhage (communicating)
- Meningitis (fungal, TB, syphilis, bacterial) causing subarachnoid fibrosis
- Intraventricular tumors (ependymoma, intraventricular metastases)
- Neurocysticercosis (racemose form)
Clinical Features
Infants (sutures open, before ~2 years)
The skull expands to accommodate raised ICP:
- Progressive macrocephaly - head circumference crossing centile lines
- Frontal bossing, calvarial thinning
- Tense, bulging anterior fontanelle (even when upright and relaxed)
- Sutural diastasis, dilated scalp veins
- "Sunset sign" (sunsetting eyes) - failure of upward gaze from pressure on the dorsal midbrain
- Lateral rectus palsies (CN VI - false localizing sign)
- Lower limb spasticity (stretching of corticospinal tracts around dilated ventricles)
- Irritability, poor feeding, lethargy
- Macewen's "cracked-pot" sign on skull percussion
Children (sutures fused)
- Headache (especially morning - worsened by recumbency)
- Vomiting (morning, projectile)
- Papilledema
- Diplopia (CN VI palsy)
- Ataxia, wide-based gait
- Endocrine dysfunction if chronic (short stature, DI, amenorrhea)
Adults
- Headache, papilledema, diplopia
- Mental status changes
- Sudden death with severe acute rises in ICP
- Akinetic mutism (pressure on structures around the 3rd ventricle)
- Temporal lobe seizures, CSF rhinorrhea, obesity (3rd ventricular dysfunction)
Normal-Pressure Hydrocephalus (NPH)
NPH is chronic communicating hydrocephalus in adults where lumbar puncture reveals normal or only minimally elevated CSF pressure (though long-term monitoring shows intermittent nocturnal pressure rises).
Classic Triad (Hakim-Adams triad):
- Gait disturbance - "magnetic gait" / apraxic gait (feet stuck to the floor, shuffling, wide-based; resembles Parkinson disease)
- Urinary incontinence (particularly in those with prominent gait disturbance)
- Dementia - subcortical type with psychomotor slowing, apathy; cortical functions (language, visuospatial) relatively preserved
Gait is the presenting feature in most cases, and gait disturbance as the dominant symptom predicts better response to treatment.
Etiology: Secondary to prior SAH, trauma, or infection in ~2/3 of patients; idiopathic in ~1/3.
Diagnosis: MRI shows enlarged ventricles + transependymal CSF absorption (periventricular hyperintensity on T2/FLAIR). LP reveals normal/low-normal pressure. A large-volume tap test (removing 30-50 mL CSF) with subsequent clinical improvement in gait is a supportive diagnostic maneuver.
A 2024 Cochrane systematic review on shunting for idiopathic NPH confirms benefit of shunting but highlights limited high-quality RCT data (PMID 39105473).
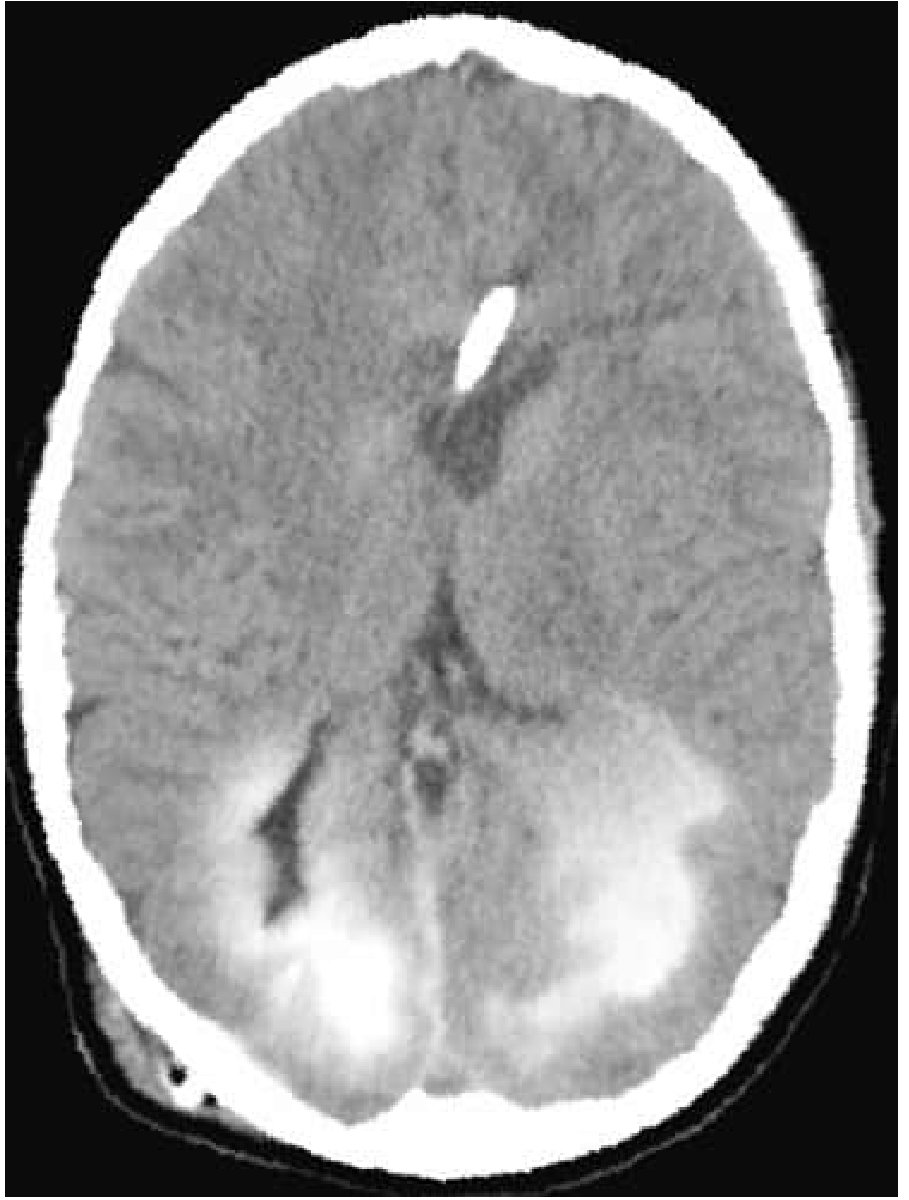
Imaging
CT findings (noncommunicating/obstructive):
- Dilatation of temporal horns disproportionate to lateral ventricular size
- Enlargement of anterior and posterior recesses of the 3rd ventricle with inferior bowing of the floor
- Periventricular lucency (transependymal edema)
- Sulcal spaces, major fissures, and basal cisterns are effaced/small
The CT below shows acute hydrocephalus with transependymal contrast diffusion:
MRI advantages:
- Better for identifying the cause (aqueductal stenosis on sagittal, tectal gliomas, posterior fossa masses)
- Aqueductal stenosis: lateral and third ventricles dilated, fourth ventricle normal size, focal narrowing of aqueduct on sagittal sequences
- Demonstrates transependymal edema as periventricular T2/FLAIR hyperintensity
- Cine phase-contrast MRI can assess aqueductal CSF flow dynamics
Key sites of obstruction to identify:
- Foramina of Monro - colloid cysts, suprasellar tumors, arachnoid cysts
- Cerebral aqueduct - tectal plate gliomas, pineal region tumors, gliosis
- Fourth ventricular outflow - Dandy-Walker, posterior fossa tumors, Chiari II
Treatment
Surgical (mainstay)
| Procedure | Indication |
|---|---|
| Ventriculoperitoneal (VP) shunt | Most common; CSF drained from ventricles to peritoneal cavity via one-way pressure valve |
| Ventriculoatrial (VA) shunt | Alternative if peritoneal cavity unsuitable |
| External ventricular drain (EVD) | Acute/emergency hydrocephalus (e.g., post-SAH, cerebellar hemorrhage); also allows ICP monitoring |
| Endoscopic third ventriculostomy (ETV) | Noncommunicating hydrocephalus (especially aqueductal stenosis); creates alternative CSF pathway; avoids implanted hardware |
Shunt complications: Malfunction (most common - causes abrupt decompensation resembling original presentation), infection, over-drainage, shunt revision as child grows.
Acute/Emergency situations:
- Cerebellar hemorrhage/infarct with acute hydrocephalus: urgent EVD placement + posterior fossa craniectomy
- Post-SAH hydrocephalus: EVD for acute phase; ~50% require permanent VP shunt
Medical:
- Acetazolamide (carbonic anhydrase inhibitor) and furosemide - used temporarily to reduce CSF production, particularly in post-hemorrhagic hydrocephalus of prematurity
- Not a long-term solution
Summary Table
| Feature | Noncommunicating | Communicating | NPH |
|---|---|---|---|
| Site of block | Intraventricular | Subarachnoid/arachnoid granulations | Arachnoid/subarachnoid (subtle) |
| Common causes | Aqueductal stenosis, tumor, Chiari | Post-SAH, meningitis, choroid plexus tumor | Idiopathic, post-SAH, trauma |
| Ventricles affected | Upstream from block | All (entire system) | All |
| CSF pressure | Elevated | Elevated or normal | Normal (intermittently elevated) |
| Treatment | ETV or VP shunt | VP shunt | VP shunt (tap test first) |
Sources:
- Bradley and Daroff's Neurology in Clinical Practice (9780323642613), pp. 1853-1857
- Robbins, Cotran & Kumar Pathologic Basis of Disease (9780443264528), pp. 1148-1149
- Grainger & Allison's Diagnostic Radiology (9780323760751), pp. 2027-2036
- Goldman-Cecil Medicine (9780323930345)
- Pearce et al., Cochrane 2024 - Shunting for idiopathic NPH (PMID 39105473)
This is a shared conversation. Sign in to Orris to start your own chat.