Management of pleural abscess
Reading File
Finding Sources
Finding Sources
Searching PubMed
"empyema thoracis" AND management
Reading File
Reading File
Reading File
Searching PubMed
"pleural empyema" AND treatment
Reading File
Reading Article
PMID: 37820359
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Here is a detailed, well-structured guide on the management of pleural abscess (empyema):
Management of Pleural Abscess (Empyema Thoracis)
A "pleural abscess" is clinically synonymous with empyema thoracis - the end stage of pleural space infection characterized by frank pus, fibrin cortex over the lung, and often loculated collections. Management follows the natural disease stage and escalates in a stepwise fashion.
Pathological Staging (BTS Classification)
Understanding the stage is the foundation of management decisions:
| Stage | Phase | Characteristics | Implication |
|---|---|---|---|
| 1 | Exudative | Protein-rich effusion (>30 g/L), free-flowing | Antibiotics ± aspiration often sufficient |
| 2 | Fibrinopurulent | Thick fluid, fibrin deposition, early loculation | Drainage mandatory; antibiotics alone likely to fail |
| 3 | Organising | Thick fibrous peel trapping the lung | Surgical management often required |
- Bailey & Love's Short Practice of Surgery, 28th Ed.
CT Imaging: Empyema vs. Lung Abscess
The key imaging distinction: empyema has a lenticular shape with no visible wall and multiple separate gas locules (septation), while a lung abscess is round with a thick, irregular wall.
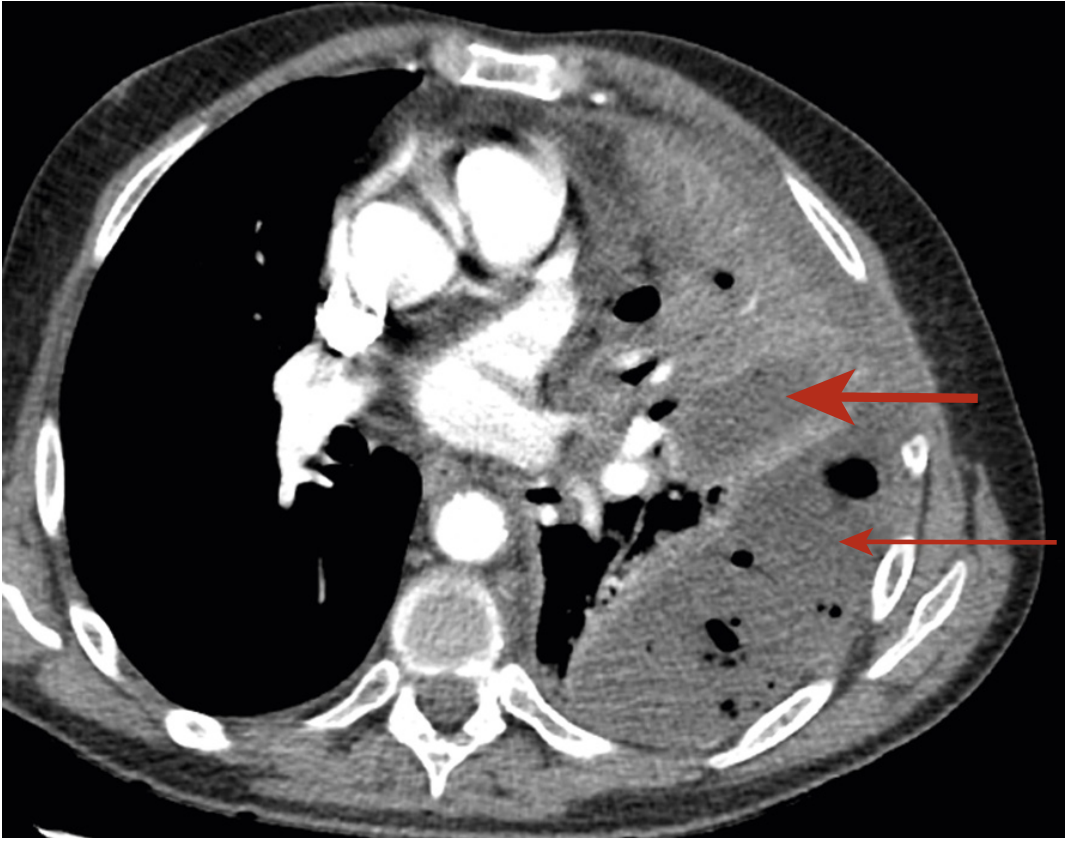
Fig: Contrast-enhanced CT distinguishing pleural empyema from lung abscess. - Murray & Nadel's Textbook of Respiratory Medicine
Step 1 - Initial Resuscitation and Assessment
-
Hospitalize all patients with suspected pleural infection
-
Blood cultures before antibiotics (positive in ~15% of cases)
-
Pleural fluid sampling - diagnostic thoracentesis is mandatory
- pH <7.2, glucose <3.4 mmol/L, LDH >1000 IU/L, or frank pus = drainage indicated
-
Thoracic ultrasonography in all cases - detects loculations/septations more accurately than CT, guides tube placement, reduces iatrogenic injury
-
Contrast-enhanced CT - reserved for persistent collections despite chest tube drainage, suspected airway obstruction, or if surgery is being planned. NOT needed routinely.
-
Nutritional support - a cornerstone identified by the 1918 U.S. Army Empyema Commission that remains unchanged today
-
Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume
Step 2 - Antibiotic Therapy
Empiric Regimens
Community-acquired empyema (parapneumonic):
- Cover aerobic organisms (Streptococcus milleri group, S. pneumoniae, Staphylococcus aureus) AND anaerobes
- Amoxicillin-clavulanate OR penicillin + metronidazole
- If penicillin-allergic: clindamycin or moxifloxacin
Hospital-acquired / post-procedural empyema:
- Broader Gram-negative and MRSA coverage needed
- Piperacillin-tazobactam + vancomycin (or linezolid) as empiric choice
- Anti-MRSA coverage should be routine
Aspiration-associated:
- Mandates anaerobic coverage (amoxicillin-clavulanate or clindamycin or metronidazole)
Duration
-
Typically 6 weeks of antibiotics total (oral step-down once clinically improving)
-
Infectious disease consultation is recommended given the complexity and duration
-
Antibiotics are a complement to drainage, not a substitute
-
Fischer's Mastery of Surgery, 8th Ed.; Murray & Nadel's Textbook of Respiratory Medicine
Intrapleural Antibiotics
- Routine intrapleural antibiotics are not recommended - systemic therapy achieves adequate pleural levels; local instillation has no proven benefit and can cause pain and chemical pleuritis.
Step 3 - Pleural Drainage
When to Drain
Drain whenever:
- Frank pus (empyema)
- Pleural fluid pH <7.2
- Positive Gram stain or culture
- Glucose <3.4 mmol/L
- Fibrinopurulent or organising phase clinically
Do NOT place drains in simple parapneumonic effusion - this can introduce bacteria and convert a simple effusion into a complicated one.
Chest Tube Size
- Small-bore tube (12-14 French) via Seldinger technique is the first-line approach for most patients - equivalent efficacy to large-bore tubes with significantly less pain during insertion and while in situ
- The MIST trial (n=405) showed no difference in death or surgical referral between small- and large-bore tubes, but large-bore tubes caused significantly more pain
- Large-bore drains are reserved for complex, thick empyemas not draining adequately
Tube Positioning
-
Under ultrasound guidance, into the largest locule in a dependent position
-
Regular saline flushes (30 mL every 6 hours via three-way stopcock) to prevent tube occlusion
-
Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume
Step 4 - Intrapleural Enzyme Therapy (IET)
For patients with loculated/septated empyema not adequately drained by tube alone:
The MIST2 Regimen (Standard of Care)
- Tissue plasminogen activator (tPA) 10 mg + DNase 5 mg instilled twice daily for 3 days
- tPA breaks down fibrin clots; DNase reduces pus viscosity by degrading extracellular DNA
- The MIST2 RCT (n=210) showed this combination significantly reduced pleural opacity on CXR, reduced surgical referral rates, and reduced hospital stay
- Neither agent alone is as effective as the combination - streptokinase (MIST1 trial, n=454) showed no benefit over placebo when used alone
Contraindications to IET
-
Recent (<1 week) cardiothoracic surgery
-
Known broncho-pleural fistula (risk of systemic fibrinolysis)
-
Active significant haemoptysis
-
Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume; Fischer's Mastery of Surgery, 8th Ed.
Step 5 - Surgical Intervention
Indicated when:
- Persistent pleural sepsis despite chest tube drainage + IET for 3-5 days
- Highly loculated, multilocular empyema not amenable to tube drainage
- Organizing phase with lung entrapment (thick fibrous peel preventing lung re-expansion)
- CT shows complex empyema or trapped lung
Surgical Options (Escalating Invasiveness)
1. VATS (Video-Assisted Thoracoscopic Surgery)
- Operation of choice for most patients requiring surgery
- Allows debridement, division of septations, lavage, and decortication under direct vision with minimal access
- Superior cosmesis, less pain, faster recovery than open surgery
- The MIST-3 trial (2023 RCT) showed early VATS reduced length of stay to 7 days vs. 10 days for standard care, supporting early surgical escalation when needed
2. Open Decortication (Thoracotomy)
- Reserved for advanced organising phase where the thick fibrous peel trapping the lung cannot be removed by VATS
- Fowler's decortication - formal peeling of the visceral pleural peel to allow lung re-expansion
- Higher morbidity but may be the only option for a completely trapped lung
3. Open Drainage (Eloesser Flap / Rib Resection)
-
For patients who are too debilitated for major surgery (high anaesthetic risk)
-
A permanent window into the pleural space allowing daily dressing changes and gradual healing by secondary intention
-
Also used for specific situations: fungal empyema (Aspergillus) - open drainage with gauze impregnated with amphotericin B
-
Bailey & Love's Surgery, 28th Ed.; Murray & Nadel's Textbook of Respiratory Medicine; Washington Manual of Medical Therapeutics
4. Thoracoplasty
- Rarely used today
- Involves resection of ribs to allow the chest wall to collapse onto the pleural cavity, obliterating the space
- Historical role in TB empyema; now used in refractory cases where lung cannot re-expand and other approaches have failed
Special Situations
Tuberculous Empyema
- Anti-TB chemotherapy for at least 6 months is the backbone
- Drainage if frank pus is present
- Decortication may be needed for trapped lung; risk of bronchopleural fistula is higher
Fungal Empyema (Aspergillus)
- Closed chest tube drainage mandatory
- Systemic antifungal therapy: initial 2-4 weeks of amphotericin B, then longer-term azole (total at least 6 months)
- Lung resection is usually necessary as infection destroys underlying lung
- For patients unfit for surgery: Eloesser flap + topical amphotericin B-impregnated gauze packing
Post-traumatic / Post-surgical Empyema
- Broad empiric antibiotic coverage (including Gram-negative organisms)
- Image-guided drain placement for loculated collections
- Early VATS for retained hemothorax converting to empyema
Bronchopleural Fistula Complicating Empyema
- Closed drainage (to prevent contamination of the contralateral lung)
- Bronchoscopic identification of fistula site
- Surgical repair (VATS or open) usually required
Management Algorithm Summary
Suspected Pleural Infection
|
v
Ultrasound + Diagnostic Thoracentesis
|
_____|_____
| |
Simple Complicated/Empyema
Effusion (pH<7.2, pus, +culture)
| |
Antibiotics Chest Tube (small-bore, US-guided)
alone + Antibiotics (6 weeks)
|
Draining adequately?
YES → Continue, remove when <50mL/day
NO (after 3-5 days)
|
Add tPA + DNase (IET × 3 days)
|
Draining adequately?
YES → Continue to resolution
NO
|
VATS (operation of choice)
|
Dense organising peel?
YES → Open decortication
NO → VATS decortication
|
Unfit for major surgery?
YES → Eloesser flap (open drainage)
Key Evidence Milestones
| Trial | Year | Finding |
|---|---|---|
| U.S. Army Empyema Commission | 1918 | Closed drainage + avoid early open drainage + obliterate space = mortality fell from 70% to 4% |
| MIST1 | 2005 | Intrapleural streptokinase alone = no benefit over placebo (n=454) |
| MIST2 | 2011 | tPA + DNase combination significantly superior to either agent alone or placebo |
| MIST-3 (RCT) | 2023 | Early VATS vs. early IET feasible; both shortened hospital stay vs. standard care; IET showed earlier resolution of pain (Bedawi et al., Am J Respir Crit Care Med, PMID 37820359) |
Outcome Predictors
Poor prognostic factors:
- Age >65
- Hospital-acquired infection
- Low serum albumin / malnutrition
- Anaerobic/Gram-negative organisms
- Delay in diagnosis or drainage
- Organism: S. aureus or Gram-negative bacilli carry worse outcomes than streptococcal infections
Sources:
- Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume (Chapter 109: Bacterial Pleural Empyema)
- Bailey & Love's Short Practice of Surgery, 28th Edition (Chapter 60: Pleural Infection and Empyema)
- Fischer's Mastery of Surgery, 8th Edition (Empyema/Fibrinolytics)
- The Washington Manual of Medical Therapeutics (Surgical Management)
- Bedawi EO et al. MIST-3 RCT. Am J Respir Crit Care Med. 2023. PMID 37820359
This is a shared conversation. Sign in to Orris to start your own chat.