Supracondylar fracture with cubitus varus deformity. For long question ms orthopaedic university examination
supracondylar fracture cubitus varus deformity MS orthopaedics long question examination
supracondylar fracture humerus children X-ray Gartland classification
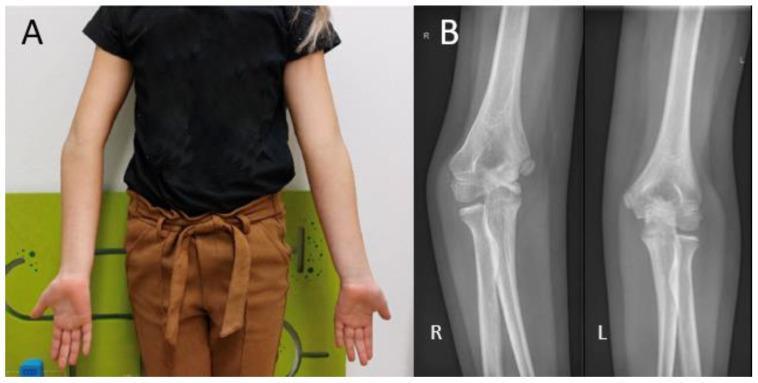
cubitus varus deformity gunstock elbow clinical photo
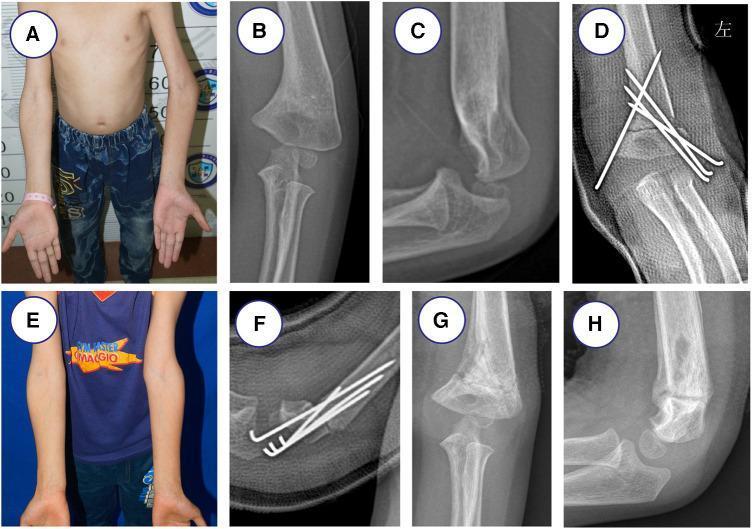
lateral closing wedge osteotomy correction cubitus varus surgical technique
Supracondylar Fracture of the Humerus with Cubitus Varus Deformity
MS Orthopaedics Long Question Answer
1. Introduction
2. Anatomy & Relevant Points
- The distal humerus is composed of two columns (medial and lateral) supporting the articular surface (trochlea + capitellum)
- Carrying angle: Normal outward deviation of the extended, supinated forearm from the arm axis — normally 10–15° (greater in females). Disappears on pronation or full flexion
- The Baumann angle (humeral–capitellar angle on AP X-ray) = normally 70–75°; reflects the carrying angle indirectly
- CRITOE — ossification centres appear in sequence: Capitellum (1–2 yr), Radial head (4–5 yr), Internal epicondyle (4–5 yr), Trochlea (8–10 yr), Olecranon (8–9 yr), External epicondyle (10–11 yr)
3. Mechanism of Injury
| Type | Mechanism | Displacement |
|---|---|---|
| Extension (98%) | Fall on outstretched hand with elbow in extension — olecranon acts as fulcrum | Distal fragment displaced posteriorly, superiorly, and internally rotated |
| Flexion (2%) | Fall on point of flexed elbow | Distal fragment displaced anteriorly |
4. Classification — Modified Gartland (Extension Type)
| Type | Description | Treatment |
|---|---|---|
| I | Minimal/no displacement; periosteum intact | Collar and cuff / backslab 3 weeks |
| IIA | Posterior cortex intact; no rotation | Reduction + above-elbow cast |
| IIB | Posterior cortex intact; rotational component | Reduction + CRPP |
| III | Complete displacement; no cortical contact | CRPP (urgent) |
| IIIA | No rotation | |
| IIIB | Posterolateral rotation of distal fragment | Higher risk for AIN, brachial artery injury |
| IV | Complete periosteal disruption; multidirectionally unstable | ORIF |
5. Clinical Features
- Swollen, flexed elbow
- S-shaped deformity in extension type (posterior swelling + anterior fullness)
- Loss of normal bony triangular relationship (medial epicondyle, lateral epicondyle, olecranon) — this triangle is preserved in supracondylar fracture (distinguishing it from elbow dislocation)
- Posterior prominence of distal humerus (not of olecranon)
- Marked tenderness in supracondylar region
- Bony triangle intact (Hueter's triangle preserved)
- Anterior interosseous nerve (AIN) — most commonly injured (tests: "OK" sign — tip-to-tip pinch; or FPL/FDP to index)
- Radial nerve — wrist/finger extension
- Median nerve — LOAF muscles
- Ulnar nerve — intrinsics
- Radial pulse — present/absent/diminished?
- Capillary refill, hand warmth, oximetry
6. Radiological Evaluation
Key Radiological Lines:
| Sign | Normal | Significance |
|---|---|---|
| Anterior humeral line (lateral view) | Intersects middle third of capitellum | If passes anterior — extension-type fracture |
| Baumann angle (AP view) | ~70–75° | Decreased → varus malunion; critical for reduction assessment |
| Radiocapitellar line | Radius always points to capitellum | Lost in radial head dislocation |
| Posterior fat pad sign | Not visible | 76% chance of occult fracture if present |
Gartland III X-ray appearance:

7. Differential Diagnosis
- Posterior dislocation of the elbow — Hueter's triangle disrupted; bony relationship between radius and capitellum lost
- Lateral condyle fracture — fracture line more distal; radius does not point to capitellum
- Medial epicondyle fracture
- Trans-physeal separation (infant/toddler)
8. Management
General Principles
- Undisplaced (Type I): Collar and cuff or posterior backslab for 3 weeks; progressive mobilisation
- Displaced (Type II–IV): Closed reduction + percutaneous K-wire fixation (CRPP) ± above-elbow cast
Closed Reduction Technique (Dunlop / modified Blount):
- Adequate anaesthesia
- Traction along the long axis, correct rotation
- Restore medial–lateral alignment on AP
- Flex elbow while pushing distal fragment forward (Blount manoeuvre)
- Confirm Baumann angle and anterior humeral line restoration
- Insert 2–3 lateral K-wires divergently (or crossed pins — more stable but 3–8% risk of iatrogenic ulnar nerve injury with medial pin)
Immobilisation:
- Above-elbow cast, elbow ~90° flexion, forearm in neutral
- Caution: Do not hyperflex if vascular compromise is present — this increases compartment pressure
Indications for ORIF:
- Failed closed reduction
- Open fracture
- Vascular injury requiring exploration
9. Neurovascular Complications
| Complication | Details | Management |
|---|---|---|
| White pulseless hand | Absent pulse + poor perfusion | Surgical emergency — urgent reduction; explore vessels if pulse does not return |
| Pink pulseless hand | Absent pulse + good perfusion | Urgent CRPP; observation 24–48 hrs; vascular consult if no pulse returns |
| Nerve injury | AIN most common (IIIB) | Usually neuropraxia; resolves after reduction and swelling subsides |
| Compartment syndrome / Volkmann's ischaemic contracture | Most serious complication | Avoid deep flexion in grossly swollen limb; early fasciotomy if suspected |
10. Cubitus Varus — The Key Complication
Definition
Incidence
Pathogenesis
- Results from malunion — specifically varus tilt + internal rotation of the distal fragment — NOT from growth arrest (this is a common examination point)
- The medial column collapses preferentially; the distal fragment tilts into varus
- Varus–valgus remodelling at the distal humerus is poor (unlike AP plane remodelling which is reasonable), hence cubitus varus persists
Clinical Features
- Cosmetic deformity — prime complaint; parents notice asymmetrical elbow
- Carrying angle reduced or reversed on the affected side
- Function generally preserved (flexion/extension and forearm rotation maintained)
- Gunstock appearance on extension
- Later complications:
- Posterolateral rotatory instability (PLRI) of the elbow
- Tardy ulnar nerve palsy — less common than in cubitus valgus, but reported
- Lateral condyle stress fracture (rare)
Investigations
- AP X-ray both elbows standing (compare Baumann angles)
- Measure Humeroulnar angle (carrying angle) bilaterally — the difference defines severity
- CT if needed for rotational deformity assessment
Indications for Surgery
- Significant cosmetic deformity causing psychological distress
- Progressive neurological symptoms
- PLRI with functional impairment
Surgical Correction — Lateral Closing Wedge Supracondylar Osteotomy
- Measure the varus angle = difference between carrying angles (affected vs normal side)
- Calculate the wedge angle to be removed from the lateral column
- Lateral approach to distal humerus (between brachioradialis and brachialis)
- Mark the osteotomy level just proximal to the olecranon fossa
- Remove a laterally based bone wedge whose apex equals the varus angle
- Close the osteotomy — medial periosteum acts as hinge
- Fix with 2–3 crossed K-wires (lateral-entry configuration) or plate fixation
- Above-elbow cast for 4–6 weeks
- Lateral scar prominence (cosmetic)
- Under/overcorrection — careful preoperative planning essential
- Ulnar nerve injury
- Lateral condyle fracture
- Loss of elbow motion
- Dome (French) osteotomy — allows correction in multiple planes; reduced prominence
- Medial opening wedge osteotomy — avoids lateral scar but requires bone graft
- Step-cut osteotomy — more stable; allows correction of rotational deformity simultaneously
11. Other Complications of Supracondylar Fracture
| Complication | Details |
|---|---|
| Malunion | Most common; leads to cubitus varus (most frequent) or cubitus valgus |
| Myositis ossificans | Avoid passive stretching; active mobilisation only |
| Stiffness | Usually resolves; rare if cast removed at appropriate time |
| Non-union | Rare due to good blood supply of metaphysis |
| Volkmann's ischaemic contracture | Most feared; missed compartment syndrome → fibrosis of forearm flexors |
| Cubitus valgus | Less common; leads to tardy ulnar nerve palsy in later years |
12. Summary Box — Examination Points
| Point | Key Fact |
|---|---|
| Most common fracture around elbow in children | Supracondylar fracture |
| Most common nerve injured | AIN (Gartland III, posterolateral displacement) |
| Most common late complication | Cubitus varus |
| Cause of cubitus varus | Malunion (NOT growth arrest) |
| Baumann angle normal value | 70–75° |
| Carrying angle normal value | 10–15° |
| Treatment of cubitus varus | Lateral closing wedge supracondylar osteotomy |
| Preserved in supracondylar fracture vs dislocation | Hueter's bony triangle |
| Most serious complication | Volkmann's ischaemic contracture |
| Emergency in vascular injury | White pulseless hand |
Make a academic correct PPT for ms orthopaedic conference with recent advancements
cd /home/daytona/workspace/attachments/bd4781f9-b905-4148-b774-eb4f935210cd && p…
cd /home/daytona/workspace/attachments/bd4781f9-b905-4148-b774-eb4f935210cd && p…
"giant cell tumor" knee resection arthrodesis reconstruction
"giant cell tumor" bone denosumab treatment outcomes
giant cell tumor distal femur proximal tibia X-ray MRI
Ilizarov bone transport distraction osteogenesis knee reconstruction
PMID: 34359548
Kindly.ake ppt
node /home/daytona/skills/shared/scripts/fetch_images.js \ "https://cdn.orris.…
mkdir -p /home/daytona/workspace/gct-ppt && ls /home/daytona/workspace/gct-ppt
~/gct-ppt/build.js
const pptxgen = require("pptxgenjs");
const { execSync } = require("child_process");
// ── Fetch images ──────────────────────────────────────────────────────────────
const urls = [
"https://cdn.orris.care/cdss_images/pmc_clinical_VQA_dfebed6ad353f72843470e9de88550e444ee8c616d76ba5a8589ecf1bd0c5111.jpg", // GCT xray+MRI
"https://cdn.orris.care/cdss_images/pmc_clinical_VQA_ba27348f0dbdf46c2acf9da3de202f53bb9bc8d16bccd254e381a8dfe26675dd.jpg", // CT soap-bubble
"https://cdn.orris.care/cdss_images/pmc_clinical_VQA_4e4597c3d6748f222ef94d305843178c1dc6b42c5f0c8ead09fd61b88ec89e76.jpg", // megaprosthesis
"https://cdn.orris.care/cdss_images/pmc_clinical_VQA_f49bc18a492b803597dab605e7544b62d7fe9f080992c7de3a5f8b76cab87ce5.jpg", // cement+denosumab postop
"https://cdn.orris.care/cdss_images/pmc_clinical_VQA_1a9c5c6cddaa9a65a8c1dccfa32cde79d0e9daca1e63e3d4defed510fa78cc43.jpg", // bone transport distraction
];
const imgs = JSON.parse(
execSync(`node /home/daytona/skills/shared/scripts/fetch_images.js ${urls.map(u => `"${u}"`).join(" ")}`).toString()
);
// ── Colour palette ─────────────────────────────────────────────────────────────
const BG = "0A1628"; // deep navy
const ACCENT = "E8A020"; // gold
const ACCENT2 = "3A9BD5"; // steel blue
const WHITE = "FFFFFF";
const LGREY = "CBD5E1";
const CARD = "132035"; // slightly lighter navy card
// ── Helper: slide header bar ───────────────────────────────────────────────────
function addHeader(slide, title, subtitle) {
// top colour bar
slide.addShape("rect", { x: 0, y: 0, w: 13.33, h: 0.9, fill: { color: ACCENT }, line: { color: ACCENT } });
slide.addText(title, { x: 0.3, y: 0.1, w: 12, h: 0.65, fontSize: 22, bold: true, color: BG, fontFace: "Calibri" });
if (subtitle) {
slide.addShape("rect", { x: 0, y: 0.9, w: 13.33, h: 0.38, fill: { color: ACCENT2 }, line: { color: ACCENT2 } });
slide.addText(subtitle, { x: 0.3, y: 0.92, w: 12, h: 0.32, fontSize: 13, color: WHITE, fontFace: "Calibri", italic: true });
}
}
// ── Helper: card box ───────────────────────────────────────────────────────────
function addCard(slide, x, y, w, h, heading, bullets) {
slide.addShape("rect", { x, y, w, h, fill: { color: CARD }, line: { color: ACCENT2, pt: 1.2 }, rectRadius: 0.08 });
if (heading) {
slide.addText(heading, { x: x + 0.12, y: y + 0.08, w: w - 0.24, h: 0.35,
fontSize: 13, bold: true, color: ACCENT, fontFace: "Calibri" });
}
if (bullets && bullets.length) {
const items = bullets.map((b, i) => ({
text: b, options: { bullet: { code: "25B8", color: ACCENT2 }, fontSize: 11.5, color: LGREY,
fontFace: "Calibri", breakLine: i < bullets.length - 1 }
}));
slide.addText(items, { x: x + 0.14, y: y + (heading ? 0.46 : 0.12), w: w - 0.28, h: h - (heading ? 0.56 : 0.22) });
}
}
// ── Helper: background ────────────────────────────────────────────────────────
function setBG(slide) {
slide.background = { color: BG };
}
// ─────────────────────────────────────────────────────────────────────────────
// BUILD PRESENTATION
// ─────────────────────────────────────────────────────────────────────────────
let pres = new pptxgen();
pres.layout = "LAYOUT_WIDE"; // 13.33" × 7.5"
pres.author = "MS Orthopaedics Conference 2026";
pres.title = "GCT Around Knee – Resection Arthrodesis with Ilizarov";
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 1 – TITLE
// ══════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide(); setBG(sl);
// decorative left stripe
sl.addShape("rect", { x: 0, y: 0, w: 0.55, h: 7.5, fill: { color: ACCENT }, line: { color: ACCENT } });
sl.addShape("rect", { x: 0.55, y: 0, w: 0.18, h: 7.5, fill: { color: ACCENT2 }, line: { color: ACCENT2 } });
sl.addText("RESECTION ARTHRODESIS\nWITH ILIZAROV FIXATOR", {
x: 1.0, y: 1.1, w: 11.5, h: 2.2, fontSize: 40, bold: true, color: WHITE,
fontFace: "Calibri", align: "left", lineSpacingMultiple: 1.3
});
sl.addShape("rect", { x: 1.0, y: 3.4, w: 7.5, h: 0.06, fill: { color: ACCENT }, line: { color: ACCENT } });
sl.addText("In Advanced Cases of Giant Cell Tumour (GCT) Around the Knee", {
x: 1.0, y: 3.55, w: 11, h: 0.65, fontSize: 20, color: ACCENT, fontFace: "Calibri", italic: true
});
sl.addText("Outcome · Problems · Obstacles · Complications", {
x: 1.0, y: 4.3, w: 11, h: 0.5, fontSize: 16, color: LGREY, fontFace: "Calibri"
});
sl.addText([
{ text: "Dr. Jishnu Prakash Baruah", options: { bold: true } },
{ text: " · Dr. Suresh Bora · Dr. Debanga Sarma Barua\nDr. Hemjit Das · Dr. Shyam Sunder S · Dr. Aswin Deepak Rajan AS", options: {} }
], { x: 1.0, y: 5.1, w: 11, h: 0.8, fontSize: 13, color: LGREY, fontFace: "Calibri" });
sl.addText("Dept. of Orthopaedics · Assam Medical College Hospital, Dibrugarh", {
x: 1.0, y: 5.9, w: 11, h: 0.4, fontSize: 12, color: ACCENT2, fontFace: "Calibri"
});
sl.addText("Int. Journal of Orthopaedics Sciences 2021; 7(2): 755-763 | MS Orthopaedics Conference 2026", {
x: 1.0, y: 6.9, w: 11.8, h: 0.35, fontSize: 10, color: "607080", fontFace: "Calibri"
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 2 – TABLE OF CONTENTS
// ══════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide(); setBG(sl);
addHeader(sl, "PRESENTATION OUTLINE", "");
const items = [
["01", "GCT – Epidemiology & Pathology"],
["02", "WHO 2020 Classification & RANKL/RANK Pathway"],
["03", "Clinical Presentation & Investigations"],
["04", "Campanacci / Enneking Staging"],
["05", "Treatment Options for Advanced GCT around Knee"],
["06", "Rationale for Resection Arthrodesis + Ilizarov"],
["07", "Materials & Methods – Patient Series"],
["08", "Surgical Technique – Step by Step"],
["09", "Results & Functional Outcomes (MSTS)"],
["10", "Complications – Analysis & Management"],
["11", "Comparative Literature Review"],
["12", "Recent Advances: Denosumab, Navigation, 3D Printing"],
["13", "Conclusions & Take-Home Messages"],
];
items.forEach(([num, text], i) => {
const col = i < 7 ? 0 : 1;
const row = i < 7 ? i : i - 7;
const x = col === 0 ? 0.4 : 6.9;
const y = 1.5 + row * 0.74;
sl.addShape("rect", { x, y, w: 0.52, h: 0.42, fill: { color: ACCENT }, line: { color: ACCENT }, rectRadius: 0.05 });
sl.addText(num, { x, y: y + 0.02, w: 0.52, h: 0.38, fontSize: 14, bold: true, color: BG, align: "center", fontFace: "Calibri" });
sl.addText(text, { x: x + 0.6, y: y + 0.04, w: 5.8, h: 0.38, fontSize: 13, color: WHITE, fontFace: "Calibri" });
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 3 – EPIDEMIOLOGY & PATHOLOGY
// ══════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide(); setBG(sl);
addHeader(sl, "GCT OF BONE – EPIDEMIOLOGY & PATHOLOGY", "Benign but locally aggressive · Intermediate malignant (WHO 2020)");
addCard(sl, 0.3, 1.45, 4.1, 2.7, "Epidemiology", [
"3–8% of all primary bone tumours globally",
"~20% in Asian populations (India, China)",
"Peak age: 20–40 years; F > M (1.5:1)",
"50% involve the knee joint (distal femur > proximal tibia)",
"80% benign course; 20–50% local recurrence",
"Malignant transformation: ~10%",
"Pulmonary metastasis: 1–4%",
]);
addCard(sl, 4.55, 1.45, 4.5, 2.7, "Pathology & Molecular Biology", [
"Stromal cells: express RANKL (key driver)",
"Giant cells: RANK+ osteoclast-like; cause osteolysis",
"H3F3A mutation: specific diagnostic marker (WHO 2020)",
"p63, vimentin positive on IHC",
"Soap-bubble lytic lesion: eccentric, epiphyseal",
"Cortical expansion ± breakthrough in grade III",
"Secondary malignant GCT: post-RT or recurrence",
]);
addCard(sl, 9.2, 1.45, 3.85, 2.7, "WHO 2020 Update", [
"Reclassified as intermediate malignant",
"H3F3A G34W mutation → diagnostic",
"Distinguishes from other giant cell-rich lesions",
"Guides targeted therapy decisions",
"Prognostic significance under study",
]);
// image strip bottom
if (imgs[1] && imgs[1].base64) {
sl.addImage({ data: imgs[1].base64, x: 0.3, y: 4.35, w: 4.0, h: 2.75 });
sl.addText("CT: Soap-bubble lytic lesion, distal femur", {
x: 0.3, y: 7.12, w: 4.0, h: 0.28, fontSize: 9, color: LGREY, align: "center", fontFace: "Calibri"
});
}
if (imgs[0] && imgs[0].base64) {
sl.addImage({ data: imgs[0].base64, x: 4.55, y: 4.35, w: 4.5, h: 2.75 });
sl.addText("AP X-ray + MRI: Campanacci Grade III, cortical breakthrough + soft tissue", {
x: 4.55, y: 7.12, w: 4.5, h: 0.28, fontSize: 9, color: LGREY, align: "center", fontFace: "Calibri"
});
}
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 4 – STAGING & CLASSIFICATION
// ══════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide(); setBG(sl);
addHeader(sl, "STAGING SYSTEMS", "Campanacci · Enneking (Musculoskeletal Tumour Society)");
// Campanacci table
sl.addText("Campanacci Grading", { x: 0.3, y: 1.45, w: 6.0, h: 0.38, fontSize: 15, bold: true, color: ACCENT, fontFace: "Calibri" });
const campRows = [
["Grade", "Cortex", "Soft Tissue", "Treatment"],
["I", "Intact, mature shell", "None", "Curettage + adjuvant"],
["II", "Thin, expanded", "None", "Curettage + cement / bone graft"],
["III ★", "Disrupted, breakthrough", "Component present", "Wide resection / en bloc"],
];
campRows.forEach((row, ri) => {
row.forEach((cell, ci) => {
const isHeader = ri === 0;
const isStudy = ri === 3;
sl.addShape("rect", {
x: 0.3 + ci * 1.52, y: 1.88 + ri * 0.55, w: 1.52, h: 0.52,
fill: { color: isHeader ? ACCENT2 : isStudy ? "1C3A5A" : CARD },
line: { color: "203050", pt: 0.5 }
});
sl.addText(cell, {
x: 0.34 + ci * 1.52, y: 1.9 + ri * 0.55, w: 1.44, h: 0.48,
fontSize: isHeader ? 11 : 10.5, bold: isHeader, color: isHeader ? WHITE : (isStudy ? ACCENT : LGREY),
fontFace: "Calibri", align: "center", valign: "middle"
});
});
});
sl.addShape("rect", { x: 0.3, y: 4.2, w: 6.05, h: 0.06, fill: { color: ACCENT }, line: { color: ACCENT } });
sl.addText("★ All 20 cases in this study were Campanacci Grade III", {
x: 0.3, y: 4.3, w: 6.05, h: 0.38, fontSize: 11, color: ACCENT, italic: true, fontFace: "Calibri"
});
// Enneking
addCard(sl, 6.7, 1.45, 6.3, 3.5, "Enneking Surgical Staging (Musculoskeletal Neoplasm)", [
"Stage 1 (Inactive): Latent, confined, asymptomatic",
"Stage 2 (Active): Progressive, cortex intact, no soft tissue",
"Stage 3 (Aggressive ★): Cortex perforated, soft tissue extension",
"",
"Surgical margins:",
" Intralesional – curettage through lesion",
" Marginal – through pseudocapsule",
" Wide – through normal tissue cuff",
" Radical – entire compartment removed",
]);
// MSTS score intro
addCard(sl, 0.3, 4.75, 6.05, 2.35, "MSTS Functional Score (0–35)", [
"7 parameters × 5 points each:",
"Pain · Function · Emotional acceptance",
"Hand positioning · Manual dexterity (upper) / Walking · Gait (lower)",
"Score ≥ 24/35 = satisfactory outcome",
"Mean score this study: 26.4 / 35 ✓",
]);
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 5 – TREATMENT OPTIONS (comparison)
// ══════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide(); setBG(sl);
addHeader(sl, "TREATMENT OPTIONS FOR ADVANCED GCT AROUND THE KNEE", "When curettage is insufficient — Comparative overview");
const opts = [
{
title: "Curettage + Adjuvant",
bullets: ["Phenol / H₂O₂ / liquid N₂ / PMMA cement", "Recurrence: 8–34%", "Only if peripheral shell intact", "Grade I–II"],
color: "1C3A5A"
},
{
title: "Endoprosthesis\n(Megaprosthesis)",
bullets: ["Immediate stability, knee preserved", "Costly (₹8–12 lakh)", "5-yr survival 73–83%", "Infection 5–12%, loosening 8–56%"],
color: "1A3850"
},
{
title: "Osteoarticular Allograft",
bullets: ["Biologic reconstruction", "Non-union, fracture, infection", "Limited availability in India", "Long-term results uncertain"],
color: "1C3A5A"
},
{
title: "Vascularised Fibula",
bullets: ["High union + hypertrophy", "Complex microsurgery", "High complication rate", "Suitable for motivated patients"],
color: "1A3850"
},
{
title: "Resection Arthrodesis\n+ Ilizarov ★",
bullets: ["Wide resection + bone transport", "Cost-effective, durable", "No graft/prosthesis needed", "THIS STUDY — Grade III"],
color: "0F2A44",
highlight: true
},
];
opts.forEach((opt, i) => {
const x = 0.3 + i * 2.56;
const border = opt.highlight ? ACCENT : ACCENT2;
sl.addShape("rect", { x, y: 1.45, w: 2.45, h: 5.65,
fill: { color: opt.color }, line: { color: border, pt: opt.highlight ? 2.5 : 1 }, rectRadius: 0.1 });
if (opt.highlight) {
sl.addShape("rect", { x, y: 1.45, w: 2.45, h: 0.55,
fill: { color: ACCENT }, line: { color: ACCENT } });
}
sl.addText(opt.title, {
x: x + 0.1, y: 1.5, w: 2.25, h: 0.48,
fontSize: 12.5, bold: true, color: opt.highlight ? BG : WHITE,
fontFace: "Calibri", align: "center", valign: "middle"
});
const items = opt.bullets.map((b, bi) => ({
text: b, options: { bullet: { code: "25BA", color: ACCENT2 }, fontSize: 11.5,
color: LGREY, fontFace: "Calibri", breakLine: bi < opt.bullets.length - 1 }
}));
sl.addText(items, { x: x + 0.14, y: 2.1, w: 2.2, h: 4.8 });
});
sl.addText("★ = Technique used in this series | All 20 patients Campanacci Grade III · Mean defect 14 cm", {
x: 0.3, y: 7.18, w: 12.8, h: 0.28, fontSize: 10, color: ACCENT, italic: true, fontFace: "Calibri"
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 6 – MATERIALS & METHODS
// ══════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide(); setBG(sl);
addHeader(sl, "MATERIALS & METHODS", "Retrospective case series · 20 patients · 2010–2015");
addCard(sl, 0.3, 1.45, 4.0, 5.6, "Inclusion Criteria", [
"Campanacci Grade III GCT around knee",
"Consent for resection arthrodesis",
"≥ 3 years follow-up",
"Confirmed histology on incision biopsy",
"CT thorax: no pulmonary metastasis",
"MRI: soft tissue extent mapped",
]);
addCard(sl, 4.5, 1.45, 4.5, 2.65, "Patient Demographics", [
"n = 20 (from 28 operated; 8 excluded)",
"Sex: 8 male · 12 female",
"Mean age: 30.5 years (range 19–38)",
"Mean symptom duration: 4 months",
"8 patients: pathological fracture at presentation",
"Follow-up: mean 36 months (30–42)",
]);
addCard(sl, 4.5, 4.3, 4.5, 2.75, "Tumour Distribution", [
"Distal femur: 14 lesions (70%)",
"Proximal tibia: 6 lesions (30%)",
"Right side: 12 · Left side: 8",
"Mean resection gap: 14 cm (12–16 cm)",
"Mean regenerate achieved: 10.8 cm",
]);
addCard(sl, 9.2, 1.45, 3.85, 5.6, "Pre-op Work-up", [
"Clinical exam: NV status, skin condition",
"Plain X-ray AP + lateral both limbs",
"MRI for soft tissue mapping",
"CT thorax to exclude lung mets",
"Incision biopsy → histology",
"Routine bloods + coagulation",
"Chest X-ray",
"Zoledronic acid given in 5 cases pre-op",
"Patient counselling (prolonged fixation!)",
]);
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 7 – SURGICAL TECHNIQUE
// ══════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide(); setBG(sl);
addHeader(sl, "SURGICAL TECHNIQUE", "Wide marginal resection + Primary Ilizarov bone transport arthrodesis");
const steps = [
{ n:"01", title:"Approach", text:"Anterior midline + medial parapatellar approach for wide access to distal femur / proximal tibia." },
{ n:"02", title:"Wide Marginal Resection", text:"Through normal bone with cuff of surrounding soft tissue. Posterior NV bundles protected. H₂O₂ irrigation + saline washout. Drain clamped post-op if drainage excessive." },
{ n:"03", title:"Intraoperative Gap Measurement", text:"Mean gap 14 cm measured. 13 cases: preconstructed Ilizarov ring fixator applied same sitting with 4 cm acute docking. 7 cases: rigid knee brace → fixator at second sitting." },
{ n:"04", title:"Corticotomy", text:"Always performed at second sitting after 7–10 day waiting. Distraction at 0.25 mm every 6 hours (1 mm/day total)." },
{ n:"05", title:"Docking", text:"Gap docked subacutely ~2 cm/week over 4–6 weeks. Tibial spine removed with osteotome at docking. Local grafts applied at docking site." },
{ n:"06", title:"Compression & Union", text:"Docking site compressed at 0.25 mm/alternate day until union. Mean time to union: 6 months. Fixator removed after radiological calcification + 2-week dynamisation." },
];
steps.forEach((s, i) => {
const col = i < 3 ? 0 : 1;
const row = i < 3 ? i : i - 3;
const x = col === 0 ? 0.3 : 6.85;
const y = 1.45 + row * 2.0;
sl.addShape("rect", { x, y, w: 6.35, h: 1.85, fill: { color: CARD }, line: { color: ACCENT2, pt: 1 }, rectRadius: 0.08 });
sl.addShape("rect", { x, y, w: 0.72, h: 1.85, fill: { color: ACCENT2 }, line: { color: ACCENT2 }, rectRadius: 0.08 });
sl.addText(s.n, { x: x + 0.02, y: y + 0.62, w: 0.68, h: 0.55, fontSize: 18, bold: true, color: BG, align: "center", fontFace: "Calibri" });
sl.addText(s.title, { x: x + 0.8, y: y + 0.08, w: 5.45, h: 0.38, fontSize: 13, bold: true, color: ACCENT, fontFace: "Calibri" });
sl.addText(s.text, { x: x + 0.8, y: y + 0.5, w: 5.45, h: 1.25, fontSize: 11, color: LGREY, fontFace: "Calibri" });
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 8 – RESULTS
// ══════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide(); setBG(sl);
addHeader(sl, "RESULTS & FUNCTIONAL OUTCOMES", "20 patients · Mean follow-up 36 months (30–42 months)");
// Big KPI boxes
const kpis = [
{ val: "26.4/35", label: "Mean MSTS Score", sub: "Satisfactory" },
{ val: "16 mo", label: "Mean Duration in Fixator", sub: "" },
{ val: "10.8 cm", label: "Mean Regenerate Achieved", sub: "of 14 cm gap" },
{ val: "6 mo", label: "Mean Time to Union", sub: "Docking site" },
{ val: "4 mo", label: "Mean Hospital Stay", sub: "" },
{ val: "100%", label: "Ambulatory at Final FU", sub: "No bone graft needed" },
];
kpis.forEach((k, i) => {
const x = 0.3 + i * 2.17;
sl.addShape("rect", { x, y: 1.45, w: 2.0, h: 1.85, fill: { color: CARD }, line: { color: ACCENT, pt: 1.5 }, rectRadius: 0.1 });
sl.addText(k.val, { x, y: 1.55, w: 2.0, h: 0.75, fontSize: 28, bold: true, color: ACCENT, align: "center", fontFace: "Calibri" });
sl.addText(k.label, { x, y: 2.3, w: 2.0, h: 0.5, fontSize: 11, color: WHITE, align: "center", fontFace: "Calibri" });
if (k.sub) sl.addText(k.sub, { x, y: 2.82, w: 2.0, h: 0.35, fontSize: 10, color: ACCENT2, align: "center", fontFace: "Calibri", italic: true });
});
// Patient table header
sl.addText("Selected Patient Data (Table 1)", {
x: 0.3, y: 3.5, w: 9, h: 0.38, fontSize: 14, bold: true, color: ACCENT, fontFace: "Calibri"
});
const tHeaders = ["#", "Age/Sex", "Site", "Defect(cm)", "Union(mo)", "MSTS", "Regen(cm)"];
const tRows = [
["1","26F","Dis.Fem","12.5","7","26","9"],
["2","29M","Prox.Tib","13","5.5","27","11"],
["4","28F","Dis.Fem","15","6","28","12"],
["7","29M","Prox.Tib","15.5","6","24","11.5"],
["10","34F","Prox.Tib","16","7","26","12"],
["16","33F","Dis.Fem","16","6","26","12"],
["20","31F","Dis.Fem","13.5","6.5","27","10.5"],
];
const colW = [0.45, 0.95, 1.0, 1.1, 0.9, 0.75, 1.0];
const rowH = 0.4;
tHeaders.forEach((h, ci) => {
const x = 0.3 + colW.slice(0,ci).reduce((a,b)=>a+b,0);
sl.addShape("rect", { x, y: 3.95, w: colW[ci], h: rowH, fill: { color: ACCENT2 }, line: { color: "203050", pt: 0.5 } });
sl.addText(h, { x, y: 3.96, w: colW[ci], h: rowH - 0.02, fontSize: 10, bold: true, color: WHITE, align: "center", fontFace: "Calibri", valign: "middle" });
});
tRows.forEach((row, ri) => {
row.forEach((cell, ci) => {
const x = 0.3 + colW.slice(0,ci).reduce((a,b)=>a+b,0);
sl.addShape("rect", { x, y: 3.95 + (ri+1)*rowH, w: colW[ci], h: rowH,
fill: { color: ri%2===0 ? CARD : BG }, line: { color: "203050", pt: 0.5 } });
sl.addText(cell, { x, y: 3.95 + (ri+1)*rowH + 0.02, w: colW[ci], h: rowH - 0.04,
fontSize: 10, color: LGREY, align: "center", fontFace: "Calibri", valign: "middle" });
});
});
sl.addText("Full data: 20 cases, all Campanacci Grade III · See Table 1 in published paper (IJOS 2021;7(2):755–763)", {
x: 0.3, y: 7.1, w: 9.5, h: 0.3, fontSize: 9, color: "607080", fontFace: "Calibri"
});
// image
if (imgs[4] && imgs[4].base64) {
sl.addImage({ data: imgs[4].base64, x: 9.6, y: 3.4, w: 3.45, h: 3.7 });
sl.addText("Bone transport distraction osteogenesis progression", {
x: 9.6, y: 7.12, w: 3.45, h: 0.28, fontSize: 9, color: LGREY, align: "center", fontFace: "Calibri"
});
}
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 9 – COMPLICATIONS
// ══════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide(); setBG(sl);
addHeader(sl, "COMPLICATIONS – ANALYSIS & MANAGEMENT", "Problems · Obstacles · Complications (Table 2 from study)");
const comps = [
{ pct: "30%", n:"6/20", title:"Equinus Deformity (Ankle)", detail:"Gradual development during fixation; 1 case required surgical TA lengthening. Prevention: early physiotherapy, ankle orthosis.", color: ACCENT },
{ pct: "20%", n:"4/20", title:"Pin Site Infection & Loosening", detail:"All half-pins affected to some extent. Managed with local Gentamicin injection and dressing. 4 distal pins loose at removal; 1 lytic tract curetted.", color: ACCENT2 },
{ pct: "20%", n:"4/20", title:"Axial Varus Deviation", detail:"Universal in ALL femoral cases. Medial migration of transported segment. Due to contracted adductor magnus. Corrected by extra pins + ring translation.", color: "E85C3A" },
{ pct: "20%", n:"4/20", title:"Residual Limb Length Discrepancy", detail:"Discrepancy > 4 cm in 4 patients (patients 6,7,10,16). < 4 cm considered clinically insignificant. Managed with shoe raise.", color: "9B6ECC" },
{ pct: "20%", n:"4/20", title:"Abscess at Docking Site", detail:"4 cases with collections that spontaneously pointed through surgical wound. Evacuated and allowed secondary healing. No recurrence.", color: "3ABFAB" },
{ pct: "15%", n:"3/20", title:"Non-union at Docking Site", detail:"3 cases: 1 = local recurrence → amputation; 1 = severe infection+fibrosis → rail fixator + grafting; 1 = hardware fatigue.", color: "CC6E3A" },
{ pct: "5%", n:"1/20", title:"Local Recurrence", detail:"Identified on biopsy after non-union. Progressive lysis in both bones. Patient underwent amputation after >1 year on fixator.", color: "CC3A3A" },
];
comps.forEach((c, i) => {
const col = i < 4 ? 0 : 1;
const row = i < 4 ? i : i - 4;
const x = col === 0 ? 0.3 : 6.85;
const y = 1.45 + row * 1.46;
sl.addShape("rect", { x, y, w: 6.35, h: 1.35, fill: { color: CARD }, line: { color: c.color, pt: 1.5 }, rectRadius: 0.07 });
sl.addShape("rect", { x, y, w: 1.1, h: 1.35, fill: { color: c.color }, line: { color: c.color }, rectRadius: 0.07 });
sl.addText(c.pct, { x: x + 0.02, y: y + 0.2, w: 1.06, h: 0.55, fontSize: 20, bold: true, color: BG, align: "center", fontFace: "Calibri" });
sl.addText(c.n, { x: x + 0.02, y: y + 0.78, w: 1.06, h: 0.38, fontSize: 11, color: BG, align: "center", fontFace: "Calibri" });
sl.addText(c.title, { x: x + 1.18, y: y + 0.06, w: 5.07, h: 0.38, fontSize: 12, bold: true, color: WHITE, fontFace: "Calibri" });
sl.addText(c.detail, { x: x + 1.18, y: y + 0.46, w: 5.07, h: 0.82, fontSize: 10.5, color: LGREY, fontFace: "Calibri" });
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 10 – COMPARATIVE LITERATURE
// ══════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide(); setBG(sl);
addHeader(sl, "COMPARATIVE LITERATURE REVIEW", "Arthrodesis vs Arthroplasty – published series");
sl.addText("Table 3 – Comparison with Published Series", {
x: 0.3, y: 1.4, w: 12.7, h: 0.38, fontSize: 14, bold: true, color: ACCENT, fontFace: "Calibri"
});
const lit = [
["Study / Method", "n", "5-yr Prosthesis Survival", "10-yr Survival", "Infection%", "Mean MSTS"],
["Myers et al. – Knee Arthroplasty", "192", "83%", "67%", "35%", "–"],
["Sharma et al. – Arthroplasty", "77", "84%", "79%", "–", "30"],
["Ahlmann et al. – Arthroplasty", "108", "76.9%", "56.3%", "2.4%", "22.25"],
["Morgan et al. – Arthroplasty", "105", "73%", "59%", "17.1%", "30"],
["Saikia et al. – Arthrodesis (plate)", "32", "–", "–", "0%", "26"],
["Natarajan et al. – Mixed", "143", "92.3%", "–", "4.2%", "–"],
["★ Present Study – Arthrodesis (Ilizarov)", "20", "N/A", "N/A", "20%*", "26.4"],
];
const cw = [4.2, 0.55, 1.7, 1.5, 1.2, 1.2];
lit.forEach((row, ri) => {
const isH = ri === 0;
const isStudy = ri === lit.length - 1;
row.forEach((cell, ci) => {
const x = 0.3 + cw.slice(0,ci).reduce((a,b)=>a+b,0);
const y = 1.85 + ri * 0.52;
sl.addShape("rect", { x, y, w: cw[ci], h: 0.5,
fill: { color: isH ? ACCENT2 : isStudy ? "0F2A44" : (ri%2===0?CARD:BG) },
line: { color: "1C3A5A", pt: 0.5 } });
sl.addText(cell, { x: x+0.06, y: y+0.04, w: cw[ci]-0.12, h: 0.42,
fontSize: isH ? 10 : 10.5, bold: isH || isStudy,
color: isH ? WHITE : isStudy ? ACCENT : LGREY,
fontFace: "Calibri", valign: "middle" });
});
});
sl.addText("* 20% pin-site infection (minor, managed conservatively) + 20% docking site abscess (self-limiting)\n★ Arthrodesis provides durable, cost-effective reconstruction — particularly relevant in developing countries / resource-limited settings", {
x: 0.3, y: 6.25, w: 12.7, h: 0.65, fontSize: 10.5, color: LGREY, fontFace: "Calibri"
});
addCard(sl, 0.3, 6.95, 12.7, 0.48, null, []);
sl.addText("Key Insight: Arthrodesis (plate or Ilizarov) yields MSTS ~26 vs arthroplasty ~22–30 — but arthroplasty carries 17–35% infection and 8–56% loosening rates over 5–10 years", {
x: 0.5, y: 6.97, w: 12.4, h: 0.44, fontSize: 11, color: ACCENT, italic: true, fontFace: "Calibri"
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 11 – RECENT ADVANCES
// ══════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide(); setBG(sl);
addHeader(sl, "RECENT ADVANCES IN GCT MANAGEMENT", "2020–2026 · Molecular · Pharmacological · Surgical · Imaging");
const advances = [
{
icon: "💊", title: "Denosumab (RANKL Inhibitor)",
bullets: [
"Human monoclonal anti-RANKL antibody (Prolia®)",
"WHO 2020: now standard for inoperable/recurrent GCT",
"Hardens tumour → facilitates en bloc resection",
"Downsizing of soft tissue in pelvic/spinal GCT",
"CAUTION: pre-op use may increase local recurrence post-curettage (Tsukamoto 2021)",
"Dose: 120 mg SC monthly; continues 6 months post-resection",
"Ref: Cancers 2021 (PMID 34359548)",
]
},
{
icon: "🔬", title: "H3F3A Mutation — Diagnostic Marker",
bullets: [
"G34W/L mutation in H3F3A gene — specific for GCT",
"WHO 2020 reclassification: intermediate malignant",
"Differentiates from other giant cell-rich bone lesions",
"Immunohistochemistry: H3.3 G34W antibody (>95% sensitivity)",
"Guides prognosis & targeted therapy trials",
"Ref: Bone 2025 (PMID 40532838)",
]
},
{
icon: "🦾", title: "3D-Printed Custom Implants & Navigation",
bullets: [
"Patient-specific 3D-printed megaprostheses (titanium)",
"Computer-aided design → exact anatomical fit",
"Navigation-assisted resection → negative margins",
"Reduces operative time and intraoperative blood loss",
"Combined use with Ilizarov in hybrid constructs",
"Growing role in complex peri-articular GCT",
]
},
{
icon: "📡", title: "Advanced Imaging & Intraoperative Tools",
bullets: [
"FDG-PET CT: staging + response monitoring",
"Dynamic contrast MRI: soft tissue extent + vascularity",
"Intraoperative frozen section for margin assessment",
"Cementation (PMMA) under CT fluoroscopy guidance",
"Microwave ablation + curettage: early data promising",
]
},
{
icon: "🔄", title: "Bone Transport Innovations",
bullets: [
"Motorised IM transport nail (PRECICE® system)",
"Bone transport + IM nail hybrid: shorter fixator time",
"Bone morphogenetic protein (BMP-2) at docking site",
"Zoledronic acid to augment regenerate quality",
"Taylor Spatial Frame (TSF): 6-axis correction of varus",
]
},
{
icon: "💉", title: "Emerging Targeted Therapies",
bullets: [
"Zoledronic acid: inhibits osteoclast activity, anti-recurrence",
"Imatinib (PDGFR inhibitor): trials in refractory GCT",
"Interferon-α / pegylated IFN: pulmonary metastases",
"RANK-Fc fusion proteins under investigation",
"Immunotherapy (anti-PD1) in malignant GCT: phase I",
]
},
];
advances.forEach((adv, i) => {
const col = i < 3 ? 0 : 1;
const row = i < 3 ? i : i - 3;
const x = col === 0 ? 0.3 : 6.85;
const y = 1.45 + row * 2.0;
sl.addShape("rect", { x, y, w: 6.35, h: 1.88, fill: { color: CARD }, line: { color: ACCENT2, pt: 1 }, rectRadius: 0.08 });
sl.addText(`${adv.title}`, {
x: x + 0.18, y: y + 0.07, w: 6.0, h: 0.38,
fontSize: 13, bold: true, color: ACCENT, fontFace: "Calibri"
});
const items = adv.bullets.map((b, bi) => ({
text: b, options: { bullet: { code: "25B8", color: ACCENT2 }, fontSize: 10.5, color: LGREY,
fontFace: "Calibri", breakLine: bi < adv.bullets.length - 1 }
}));
sl.addText(items, { x: x + 0.18, y: y + 0.5, w: 6.05, h: 1.3 });
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 12 – CONCLUSIONS
// ══════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide(); setBG(sl);
addHeader(sl, "CONCLUSIONS & TAKE-HOME MESSAGES", "Resection Arthrodesis with Ilizarov in Grade III GCT around the Knee");
const msgs = [
{ num:"1", msg:"Viable, durable reconstruction with MSTS 26.4/35 — comparable to arthroplasty without the cost burden or risk of implant failure." },
{ num:"2", msg:"No bone graft required in any case — corticotomy + distraction histogenesis provides de novo autogenous bone." },
{ num:"3", msg:"All 20 patients ambulatory at final follow-up — loss of knee motion is the accepted trade-off for oncological control." },
{ num:"4", msg:"Axial varus deviation is universal in femoral cases — attributed to contracted adductor magnus; managed with extra pins and ring translation." },
{ num:"5", msg:"Nonunion rate 15%: infection and local recurrence are culprit causes — vigilant surveillance is mandatory." },
{ num:"6", msg:"Prolonged fixator time (mean 16 months) demands psychological support and patient counselling throughout treatment." },
{ num:"7", msg:"Denosumab + Ilizarov hybrid strategy: pre-op denosumab may harden tumour → easier resection → Ilizarov reconstruction; emerging approach." },
{ num:"8", msg:"Salvage role: indicated after failed prosthetic replacement or osteoarticular allografting — a true last-resort limb-salvage option." },
];
msgs.forEach((m, i) => {
const row = Math.floor(i / 2);
const col = i % 2;
const x = col === 0 ? 0.3 : 6.85;
const y = 1.45 + row * 1.43;
sl.addShape("rect", { x, y, w: 6.35, h: 1.32, fill: { color: CARD }, line: { color: ACCENT2, pt: 1 }, rectRadius: 0.07 });
sl.addShape("rect", { x, y, w: 0.65, h: 1.32, fill: { color: ACCENT }, line: { color: ACCENT } });
sl.addText(m.num, { x, y: y + 0.35, w: 0.65, h: 0.55, fontSize: 20, bold: true, color: BG, align: "center", fontFace: "Calibri" });
sl.addText(m.msg, { x: x + 0.75, y: y + 0.12, w: 5.5, h: 1.1, fontSize: 11.5, color: LGREY, fontFace: "Calibri" });
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 13 – THANK YOU
// ══════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide(); setBG(sl);
sl.addShape("rect", { x: 0, y: 0, w: 0.6, h: 7.5, fill: { color: ACCENT }, line: { color: ACCENT } });
sl.addShape("rect", { x: 12.73, y: 0, w: 0.6, h: 7.5, fill: { color: ACCENT }, line: { color: ACCENT } });
sl.addShape("rect", { x: 0, y: 0, w: 13.33, h: 0.18, fill: { color: ACCENT2 }, line: { color: ACCENT2 } });
sl.addShape("rect", { x: 0, y: 7.32, w: 13.33, h: 0.18, fill: { color: ACCENT2 }, line: { color: ACCENT2 } });
sl.addText("THANK YOU", {
x: 0.7, y: 1.0, w: 11.93, h: 1.8, fontSize: 72, bold: true, color: WHITE,
fontFace: "Calibri", align: "center", charSpacing: 10
});
sl.addShape("rect", { x: 3.0, y: 2.9, w: 7.33, h: 0.07, fill: { color: ACCENT }, line: { color: ACCENT } });
sl.addText("Questions & Discussion", {
x: 0.7, y: 3.1, w: 11.93, h: 0.65, fontSize: 24, color: ACCENT,
fontFace: "Calibri", align: "center", italic: true
});
sl.addText("Int. Journal of Orthopaedics Sciences 2021; 7(2): 755-763\nDOI: 10.22271/ortho.2021.v7.i2j.2702", {
x: 0.7, y: 3.9, w: 11.93, h: 0.7, fontSize: 13, color: LGREY, fontFace: "Calibri", align: "center"
});
sl.addText([
{ text: "Dr. Jishnu Prakash Baruah · Dr. Suresh Bora · Dr. Debanga Sarma Barua\n", options: { bold: true } },
{ text: "Dr. Hemjit Das · Dr. Shyam Sunder S · Dr. Aswin Deepak Rajan AS", options: {} }
], { x: 0.7, y: 4.75, w: 11.93, h: 0.9, fontSize: 14, color: WHITE, fontFace: "Calibri", align: "center" });
sl.addText("Department of Orthopaedics · Assam Medical College & Hospital, Dibrugarh, Assam", {
x: 0.7, y: 5.75, w: 11.93, h: 0.45, fontSize: 13, color: ACCENT2, fontFace: "Calibri", align: "center"
});
sl.addText("MS Orthopaedics Conference | 2026", {
x: 0.7, y: 6.75, w: 11.93, h: 0.38, fontSize: 11, color: "607080", fontFace: "Calibri", align: "center"
});
}
// ── Write file ─────────────────────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/gct-ppt/GCT_Ilizarov_Arthrodesis_MSOrtho2026.pptx" })
.then(() => console.log("DONE"))
.catch(e => { console.error(e); process.exit(1); });
Potts spine for ms orthopaedic
Generate a comprehensive MS Ortho long answer on Pott's spine with clinical features and management
Generate PDF summary document with clinical cases and imaging examples