Advantages and disadvantages of anterior and superior approach of clavicle
Reading File
Finding Sources
Finding Sources
Searching the Web
anterior vs superior approach clavicle fracture fixation advantages disadvantages
Reading File
Reading Web Page
https://surgeryreference.aofoundation.org/orthopedic-trauma/…
Reading File
I have comprehensive, authoritative information from Rockwood and Green's (2025) and the AO Surgery Reference. Here is the full answer:
Surgical Approaches to the Clavicle: Anterior (Anteroinferior) vs. Superior (Anterosuperior)
These are the two standard plate positions used for open reduction and internal fixation (ORIF) of clavicle fractures, each with distinct trade-offs.
Anteroinferior (Anterior) Approach
Indication: Can be used for nearly any clavicular shaft fracture. The incision is made just inferiorly to the clavicle, centered over the fracture site (oblique, 8-10 cm). The platysma is divided, supraclavicular nerves are identified and protected, and the clavipectoral fascia is incised to expose the bone.
Advantages
- Safer screw trajectory - screws are directed from anterior to posterior in the wider AP dimension of the clavicle, greatly reducing the risk of inadvertent drill plunge into the lung, subclavian vessels, or brachial plexus
- Longer screws - the AP diameter is larger than the superoinferior dimension, allowing more purchase
- Less hardware prominence - the plate sits on the anterior (less subcutaneous) surface, reducing skin irritation
- Lower plate removal rates - a large meta-analysis showed 5% vs. 11% removal rate compared to superior plating (p = .008)
- Easier plate contouring - technically simpler to bend a small-fragment compression plate along the anterior border (though precontoured plates have largely negated this benefit)
- Better cosmesis - the incision is slightly inferior to the bone, not directly over it, reducing scar visibility
- Similar clinical outcomes - union rates, plate failure, and functional scores are equivalent to superior plating in all comparative studies
Disadvantages
- Less familiar - not the traditional approach; less commonly taught and performed
- Obscures fracture radiographically - the plate overlies the fracture site on standard AP views, making postoperative radiographic assessment harder
- Biomechanically possibly inferior - systematic reviews of biomechanical studies suggest superior plating provides greater stiffness and strength under bending loads in transverse fractures (though this does not translate to worse clinical outcomes)
Anterosuperior (Superior) Approach
Indication: Can be used for all lateral, medial, and diaphyseal clavicle fractures. The incision is made directly over or just superiorly to the clavicle, centered over the fracture site. Subcutaneous flaps are raised anteriorly and posteriorly, the clavipectoral fascia is incised, and the deltoid is reflected laterally.
Advantages
- Most familiar and widely used - the standard approach for most surgeons; easily extended medially and laterally
- Clear radiographic visualization - excellent postoperative AP views of the clavicle and fracture site for monitoring healing
- Biomechanically stronger - superior surface is the tension side of the clavicle; superior plating resists bending forces more effectively in transverse fractures
- Better fit for precontoured plates - anatomic plates are designed to match the superior surface of the clavicle's S-shaped contour
- Direct, extensile exposure - simple to extend the approach to the sternoclavicular or acromioclavicular joints
Disadvantages
- Dangerous screw trajectory - screws pass from superior to inferior; inadvertent "plunging" of the drill places the subclavian artery/vein, brachial plexus, and apex of the lung directly at risk
- Short screw length - the superoinferior dimension of the clavicle is narrow (typically 14-16 mm in females, 16-18 mm in males), limiting screw purchase
- Higher hardware prominence - the plate sits directly under the thin subcutaneous skin of the superior clavicle, causing more soft tissue irritation and symptomatic hardware
- Higher plate removal rate - approximately 11% vs. 5% for the anteroinferior approach
- Supraclavicular nerve risk - sensory branches of the supraclavicular nerve are at risk; sacrifice causes numbness and can lead to painful neuromas
Summary Comparison Table
| Feature | Anteroinferior | Anterosuperior (Superior) |
|---|---|---|
| Screw safety | Safer (AP direction) | Riskier (superior-to-inferior) |
| Screw length | Longer (AP dimension) | Shorter (SI dimension) |
| Hardware prominence | Less | More |
| Plate removal rate | ~5% | ~11% |
| Surgeon familiarity | Less familiar | Standard/most common |
| Radiographic view post-op | Obscured by plate | Clear |
| Biomechanical strength | Possibly less (bending) | Greater stiffness |
| Clinical outcomes | Equivalent | Equivalent |
| Precontoured plate fit | Less optimal | Better fit |
Key Point
Despite the biomechanical advantage of the superior surface as the tension side of the clavicle, all clinical studies comparing the two approaches show equivalent union rates, plate failure, and functional scores (Rockwood and Green's, 10th ed., 2025). The anteroinferior approach has a lower symptomatic hardware and plate removal rate, making it increasingly preferred in contemporary practice. The choice ultimately depends on surgeon experience and fracture pattern.
Source: Rockwood and Green's Fractures in Adults, 10th ed. 2025; AO Surgery Reference (Andermahr, McKee, Nam)
What are the specific neurovascular risks with each approach?
Finding Sources
Finding Sources
Searching the Web
neurovascular risks anterior inferior vs superior clavicle plating subclavian supraclavicular nerve
Reading File
Reading File
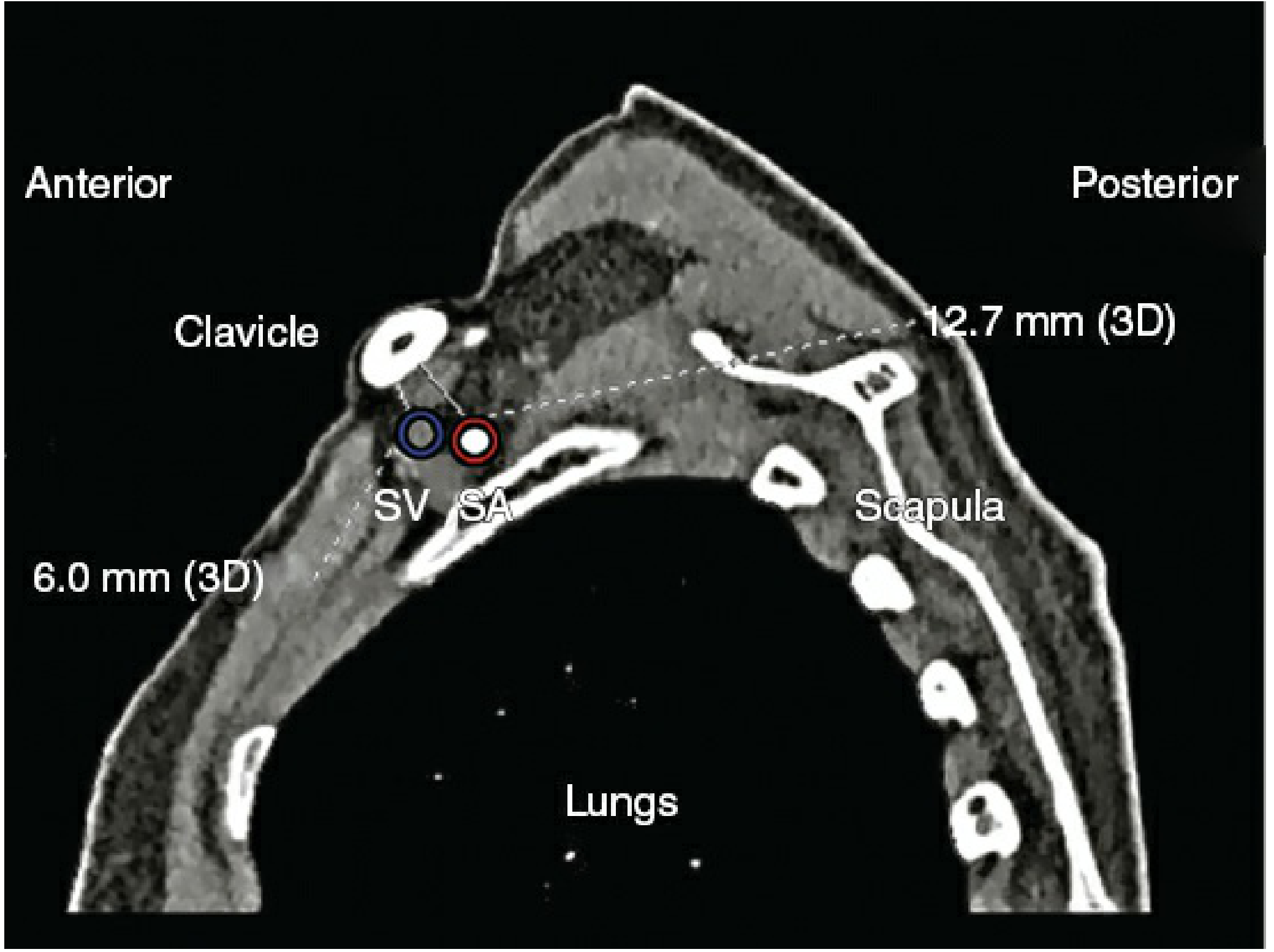
Excellent - I have all the detail needed, including the CT anatomy image. Here is the complete answer:
Neurovascular Risks: Anterior vs. Superior Approach to the Clavicle
Relevant Anatomy First
Understanding the risks requires knowing the layer-by-layer anatomy beneath the clavicle:
- Platysma - most superficial, just under skin; divided during any approach
- Supraclavicular nerves (C3, C4) - exit behind the sternocleidomastoid, run superficially as three branches (anterior, middle, posterior) crossing the clavicle medial to lateral. These are subcutaneous and at risk from the skin incision itself
- Subclavius muscle - on the undersurface of the clavicle; acts as a soft tissue buffer between the clavicle and the deep structures
- Subclavian vein - runs directly below subclavius and above the first rib; within less than 1 cm of the posterior cortex of the entire medial half of the clavicle
- Subclavian artery - more posterior, separated from the vein by the scalenus anterior muscle medially; lies within ~2 cm posteroinferiorly in the middle third
- Brachial plexus - sits most posteriorly; closest to the clavicle at the midportion (middle third)
The subclavian vessels are closest at the medial end and progressively further away laterally (artery and vein at least 45 mm away from the lateral clavicle).
Neurovascular Risks by Approach
1. Anteroinferior (Anterior) Approach
| Structure at Risk | Risk | Mechanism |
|---|---|---|
| Supraclavicular nerves (C3/C4) | Moderate - most common complication | Horizontal incision crosses all three branches (anterior, middle, posterior) |
| Neuroma formation | Uncommon but serious | Transected nerve end in scar tissue; can cause chronic, debilitating pain despite an otherwise successful operation |
| Subclavian vein/artery | Low (relative) | Screws directed in AP direction; longer AP diameter gives more margin; subclavius buffer remains between plate and vessels |
| Brachial plexus | Low | AP screw trajectory keeps drill away from posteroinferior zone where plexus lies |
Key point - supraclavicular nerve detail: The nerve can be transected during incision or dissection. This produces numbness below the incision (anterior chest wall/deltoid region). This numbness often improves over time and most patients tolerate it if warned preoperatively. However, the proximal stump can form a painful neuroma in the scar - rare but potentially the most disabling complication of clavicle ORIF. For this reason the AO recommendation is explicit: do not sacrifice the supraclavicular nerve. A nerve-sparing technique or vertical incision orientation reduces this risk.
Caveat on "safer" drilling: The anterior approach is theoretically safer for the subclavian vessels because the AP diameter is wider and the drill points away from the posteroinferior neurovascular zone. However, a cadaveric study by Lo et al. (2010) challenged this assumption, demonstrating that anteroinferior plating still carries neurovascular proximity risks - the vein can lie within the screw path particularly in the medial half.
2. Anterosuperior (Superior) Approach
| Structure at Risk | Risk | Mechanism |
|---|---|---|
| Supraclavicular nerves (C3/C4) | Moderate | Incision is directly over the superior clavicle; sensory branches encountered during subcutaneous flap elevation |
| Neuroma formation | Same as anterior | Proximal nerve stump neuroma in scar - same warning applies |
| Subclavian vein | Higher (relative) | Screws directed superior-to-inferior; vein lies within <1 cm of the medial half posterior cortex; inadvertent drill plunge exits directly into this zone |
| Subclavian artery | Moderate | Posterior to vein; at risk with deep plunge, especially medially |
| Brachial plexus | Moderate | Closest to clavicle at midshaft; superior-to-inferior drill trajectory passes toward it |
| Pneumothorax / lung apex | Rare but catastrophic | Medial third drilling; the pleural apex lies posterolateral to the great vein confluence at the medial clavicle |
Key point - the "plunge" risk: The clavicle is narrow superoinferiorly (only 14-18 mm in most patients). Screws are typically just 14-16 mm (females) to 16-18 mm (males). A drill that overshoots even a few millimeters exits the inferior cortex and can enter the subclavicular space. This is the most feared intraoperative complication. The standard prevention is to use both hands on the drill, advance slowly, and use drill sleeves. Fluoroscopy can help in difficult cases.
Medial third is the danger zone for both approaches: Here the subclavian vein is within 1 cm of the posterior cortex. The subclavius muscle is thinnest here, providing least protection. Extreme caution is mandatory when manipulating medial fracture fragments or placing medial screws from either approach.
Side-by-Side Summary
| Neurovascular Risk | Anteroinferior | Anterosuperior (Superior) |
|---|---|---|
| Supraclavicular nerve division | Yes - from incision | Yes - from subcutaneous flap |
| Painful neuroma | Yes (rare) | Yes (rare) |
| Sensory numbness below incision | Common if nerve divided | Common if nerve divided |
| Subclavian vein injury from drilling | Lower | Higher (superoinferior trajectory) |
| Subclavian artery injury | Lower | Higher (superoinferior trajectory) |
| Brachial plexus injury | Lower | Higher |
| Pneumothorax | Very rare | Rare (medial drilling) |
| Screw cutout into subclavicular space | Less likely (AP direction) | More likely (short SI dimension) |
Clinical Bottom Line
Despite the theoretical anatomical advantage of the anterior approach for deep neurovascular safety, clinical studies and meta-analyses show no statistically significant difference in rates of neurovascular injury between the two approaches - because true iatrogenic vascular injury remains rare with either technique when performed carefully. The 2025 systematic review (Rompen et al.) confirmed no significant difference in neurovascular injury rates (OR 5.35, 95% CI 0.25-116.31, P=0.29), though the event rate was so low that the comparison was underpowered.
The supraclavicular nerve is the structure most commonly injured in practice with either approach, and its protection is a priority in both.
Sources: Rockwood and Green's Fractures in Adults, 10th ed. 2025; AO Surgery Reference (Andermahr, McKee, Nam); Lo et al. Orthopedics 2010; Sinha et al. J Bone Joint Surg Br 2011
This is a shared conversation. Sign in to Orris to start your own chat.