Can you tell me the diagnositc criteria, work up and management of diabetes insipidus?
Reading File
Finding Sources
Searching PubMed
"diabetes insipidus"[MeSH Terms] AND diagnosis AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have very comprehensive content. Let me compile the full response.
Diabetes Insipidus: Diagnostic Criteria, Workup, and Management
Definition
Diabetes insipidus (DI) is the excretion of a large volume of hypotonic (insipid, tasteless) urine, usually manifested by polyuria (>50-60 mL/kg/day, or roughly >3 L/day in adults) and polydipsia. This must be distinguished from increased frequency of small urine volumes, and from large volumes of isotonic or hypertonic urine (which indicate solute diuresis instead).
- Goldman-Cecil Medicine, p. 2418
Classification
There are five pathophysiologic subtypes:
| Type | Mechanism |
|---|---|
| Central DI (arginine vasopressin deficiency) | Failure of hypothalamus/posterior pituitary to secrete ADH |
| Nephrogenic DI (arginine vasopressin resistance) | Renal tubular resistance to ADH action |
| Primary Polydipsia (dipsogenic or psychogenic) | Excessive fluid intake suppresses ADH; medullary washout |
| Gestational DI | Placental vasopressinase degrades ADH |
| Partial DI | Central or nephrogenic, incomplete |
All variants share the cardinal feature: large volumes of dilute urine (urine osmolality often <100-150 mOsm/kg) in the face of an inappropriately elevated plasma osmolality.
- Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 737
Diagnostic Criteria
Clinical Presentation
- Polyuria (>3 L/day, up to 15-20 L/day in severe cases)
- Polydipsia (compensatory; driven by hypertonicity if thirst is intact)
- No hyperglycemia, no glycosuria (distinguishes from diabetes mellitus)
- If the thirst mechanism is impaired: rapid dehydration and hypernatremia
Initial Biochemical Screen
- Plasma osmolality elevated (>295 mOsm/kg; normal 280-295) - or inappropriately normal despite ongoing polyuria
- Serum sodium elevated or high-normal
- Urine osmolality inappropriately low (<300 mOsm/kg, often <100)
- Urine specific gravity <1.005
- Rule out glycosuria, hypercalcemia, hypokalemia (common causes of acquired nephrogenic DI)
Diagnostic Workup
Step 1: Confirm Water Diuresis vs. Solute Diuresis
The first step in any case of polyuria is to measure urine osmolality:
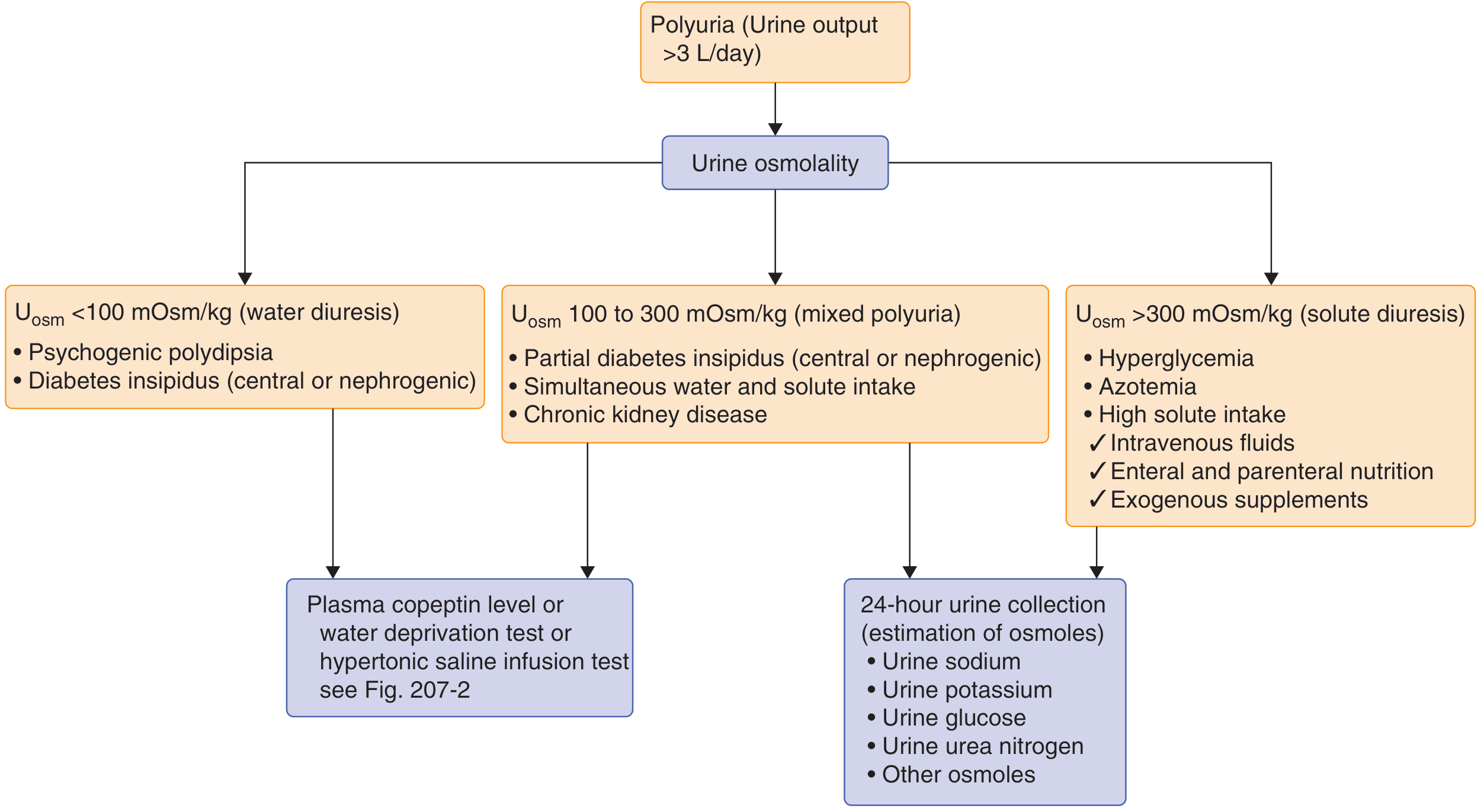
- Uosm <100 mOsm/kg → water diuresis: DI (central or nephrogenic) or psychogenic polydipsia
- Uosm 100-300 mOsm/kg → mixed or partial DI; also consider CKD
- Uosm >300 mOsm/kg → solute diuresis (hyperglycemia, post-obstructive, high solute intake) - proceed with 24-hour urine collection
Step 2: Water Deprivation Test
This is the preferred confirmatory test for DI.
Protocol:
- For mild polyuria: withhold fluids from 10 PM onward. For severe polyuria (8-10 L/day): begin in the morning under close observation.
- Baseline: urine volume (Uvol), urine osmolality (Uosm), plasma osmolality (Posm), serum Na, weight, BP and pulse (sitting and standing).
- Collect urine and plasma hourly for Uvol, Uosm, Posm. Monitor weight, BP, pulse.
- Stop when:
- Uosm plateaus (hourly increase <30 mOsm/kg for 3 consecutive hours), OR
- Body weight falls by 3-5%, OR
- Systolic BP drops >20 mmHg
- Administer 1 µg desmopressin IV or IM (or 5 µg AVP SC). Measure Uosm and urine output at 30, 60, and 120 minutes post-injection. Use the highest Uosm to evaluate response.
Precautions: Discontinue any medications affecting ADH secretion. Observe for hypotension and nausea (both stimulate ADH). Do not allow smoking during the test.
- Henry's Clinical Diagnosis, pp. 745-756
Step 3: Interpret Results
| Condition | Pre-AVP Uosm vs. Posm | Response to AVP |
|---|---|---|
| Normal | Uosm > Posm | <10% further rise |
| Complete Central DI | Uosm < Posm | >50% increase in Uosm |
| Nephrogenic DI | Uosm < Posm | <10% increase |
| Partial Central DI | Uosm may exceed Posm | 10-50% increase |
| Partial Nephrogenic DI | Uosm may exceed Posm | >10% increase |
| Primary Polydipsia | Uosm > Posm (medullary washout may blunt this) | <10% change |
For ambiguous cases, plot basal and post-dehydration Uosm against plasma ADH using the Zerbe-Robertson nomograms for further distinction between partial nephrogenic DI, partial central DI, and primary polydipsia.
Step 4: Copeptin Testing (Modern Approach)
Plasma ADH measurement has poor ex-vivo stability and only ~38% accuracy in differentiating DI from primary polydipsia. Copeptin (the C-terminal segment of pre-pro-arginine vasopressin) is a superior surrogate:
- Baseline copeptin >21.4 pmol/L (without prior thirsting): diagnostic of nephrogenic DI
- Copeptin ≤4.9 pmol/L after hypertonic saline infusion test: central DI (complete or partial)
- Copeptin >4.9 pmol/L after stimulation: primary polydipsia
- Combined with hypertonic infusion test: diagnostic accuracy 97% vs. ~80% for water deprivation test alone
A recent meta-analysis (PMID 37225043) confirmed the superior diagnostic accuracy of copeptin in differentiating DI subtypes.
- Henry's Clinical Diagnosis, pp. 787-789; Tietz Textbook of Laboratory Medicine, 7th Ed.
Step 5: Localize the Cause
For Central DI:
- MRI brain/pituitary with gadolinium: look for absence of the posterior pituitary "bright spot" on T1, thickened pituitary stalk, hypothalamic mass
- If no obvious cause: check CSF (tumor cells, ACE level for neurosarcoidosis, β-HCG for germinoma)
- Genetic testing if family history suggests inherited mutation (vasopressin or AVP receptor gene)
- Important: Spontaneous central DI should not be labeled idiopathic until at least 4 years of follow-up with annual CT or MRI to exclude occult tumor or infiltrative process
Causes of Central DI: Trauma, neurosurgery, tumors (craniopharyngioma, germinoma, metastases), granulomas (Langerhans cell histiocytosis, sarcoidosis, TB), autoimmune (lymphocytic infundibuloneurohypophysis - especially postpartum women), congenital
For Nephrogenic DI:
-
Check for causative medications: lithium, demeclocycline, amphotericin, cidofovir, foscarnet
-
Check electrolytes: hypokalemia, hypercalcemia
-
Genetic testing: AVPR2 mutations (X-linked, >90% of congenital cases), AQP2 mutations (<10%)
-
Renal biopsy rarely needed
-
Goldman-Cecil Medicine, pp. 2174-2320
Management
The overall treatment goal is to reduce polyuria and polydipsia to a tolerable level while avoiding overtreatment (which causes hyponatremia).
Central DI
First-line: Desmopressin (DDAVP) - synthetic V2 receptor agonist, the drug of choice
| Route | Dose |
|---|---|
| Intranasal spray | 10-40 µg in 2-3 divided doses/day |
| Oral tablet | 0.1-0.2 mg 2-3 times/day (take fasting; absorption decreased 50% with food) |
| Subcutaneous injection | 1-4 µg every 12-24 hours as needed |
| IV/IM | 1-4 µg for acute management |
Desmopressin acts selectively on V2 receptors to increase water permeability in the distal tubule and collecting duct. It has no V1 vasoconstrictor activity (unlike native vasopressin), making it much safer.
Monitoring: Titrate to lowest effective dose. Risk of water intoxication and hyponatremia with overdosage. Watch for headache, nausea, abdominal cramps. Nasal formulation less effective if nasal congestion present.
Gestational DI: Desmopressin is also the drug of choice (placental vasopressinase does not degrade DDAVP). Target plasma osmolality at the lower set-point of pregnancy (~10 mOsm/kg H2O below normal). Treatment may be required only during pregnancy.
- Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 493; Goldman-Cecil Medicine
Nephrogenic DI
There is no equivalent of desmopressin for nephrogenic DI. Management is directed at:
- Remove or treat the underlying cause (stop lithium if possible, correct hypercalcemia, correct hypokalemia)
- Low-sodium diet - reduces osmotic load and urine volume
- Thiazide diuretics (e.g., hydrochlorothiazide) - paradoxically reduce urine volume by inducing mild volume depletion, which increases proximal tubular reabsorption and reduces water delivery to the collecting duct
- Amiloride - especially useful in lithium-induced DI (blocks lithium entry into collecting duct cells via ENaC)
- NSAIDs (e.g., indomethacin) - inhibit prostaglandin synthesis, which enhances ADH action; used in combination with thiazides in refractory cases
- Guyton and Hall Medical Physiology, p. 380; Goldman-Cecil Medicine
Primary Polydipsia
- Restrict fluid intake
- Treat underlying psychiatric condition if psychogenic
- Do not give desmopressin - this will cause severe hyponatremia
- All patients should have MRI of the brain before concluding the cause is idiopathic or psychiatric
Summary Table
| Feature | Central DI | Nephrogenic DI | Primary Polydipsia |
|---|---|---|---|
| ADH/copeptin level | Low | Normal or elevated | Normal or low (suppressed by excess intake) |
| Response to desmopressin | >50% rise in Uosm | <10% rise | Minimal |
| Plasma osmolality | High or normal | High or normal | Low-normal |
| Urine osmolality | Very low | Very low | Low (may be partially concentrated) |
| MRI brain | May show lesion | Normal | Normal |
| Treatment | Desmopressin | Thiazides, low-Na diet, NSAIDs | Fluid restriction |
Key recent evidence: A 2023 meta-analysis (PMID 37225043) confirmed copeptin's superior diagnostic accuracy over the classic water deprivation test for differentiating DI subtypes. Copeptin-guided diagnosis is increasingly preferred in modern practice, particularly when water deprivation test results are equivocal.
Sources: Goldman-Cecil Medicine, Guyton & Hall Medical Physiology, Henry's Clinical Diagnosis and Management by Laboratory Methods, Tietz Textbook of Laboratory Medicine (7th Ed.), Katzung's Basic and Clinical Pharmacology (16th Ed.)
I read from harrison's and multiple different tests are given. Are they relevant or should just precisely focus on the tests you have provided from your research?
Finding Sources
Searching the Web
Harrison's principles diabetes insipidus diagnostic tests hypertonic saline water deprivation copeptin
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have everything I need for a thorough, precise comparison. Here's the full answer:
Harrison's vs. Other Textbooks: Are All the Tests Relevant?
Short answer: Yes, all those tests are real and used clinically - but Harrison's 22nd edition (2025) gives you the most current, hierarchical picture of which tests to use when, and explicitly tells you why the old water deprivation test is no longer the gold standard.
Here is how everything fits together:
The Tests Mentioned Across Textbooks and Their Status
1. Water Deprivation Test (Indirect AVP Test)
- Still relevant, but no longer the gold standard.
- Harrison's explicitly states: "The indirect water deprivation test was the gold standard for differential diagnosis for many years... the published criteria for interpretation were based on post hoc data from a small number of patients with an overall diagnostic accuracy of 70% and only 41% for patients with primary polydipsia."
- So it works, but is wrong in 30-60% of the hardest cases (partial DI vs. primary polydipsia). It is still useful when copeptin assays are unavailable.
2. Hypertonic Saline Infusion + Copeptin Measurement
- The new preferred gold standard per Harrison's 22nd edition.
- Raise plasma sodium to ≥150 mmol/L via hypertonic saline infusion, then measure copeptin:
- Stimulated copeptin >4.9 pmol/L → Primary polydipsia
- Stimulated copeptin ≤4.9 pmol/L → Central (AVP deficiency)
- Diagnostic accuracy: 96.5% vs. 70% for the water deprivation test
- Requires close monitoring of sodium levels during the infusion
3. Baseline Copeptin (No Prior Thirsting)
- Copeptin >21.4 pmol/L without water deprivation = diagnostic of nephrogenic DI (complete or partial)
- This alone can rule in nephrogenic DI immediately, skipping all further tests
4. Arginine Stimulation + Copeptin
- Harrison's references this as an emerging alternative to hypertonic saline
- Slightly lower diagnostic accuracy than hypertonic saline-stimulated copeptin
- Useful where hypertonic saline is not tolerated
5. Desmopressin Test (Post-Deprivation or Standalone)
- Administer 2 µg desmopressin SC, then recheck urine osmolality
- If urine Uosm increases >50%: central DI
- If <50% (or <9-10%): nephrogenic DI
- Harrison's uses this as a second-line clarifying step within the water deprivation pathway (for Uosm 300-800 mOsm/kg after deprivation)
- Also useful as a quick bedside screen: if serum Na is already >147 mmol/L, desmopressin test alone can differentiate central from nephrogenic DI without needing the full water deprivation protocol
6. Direct Plasma AVP Measurement
- Harrison's notes this was proposed but is not in routine clinical use because of technical assay limitations
- Copeptin has replaced it as the AVP surrogate
Harrison's Unified Diagnostic Algorithm (2025)
Here is the complete current algorithm from Harrison's 22nd edition:
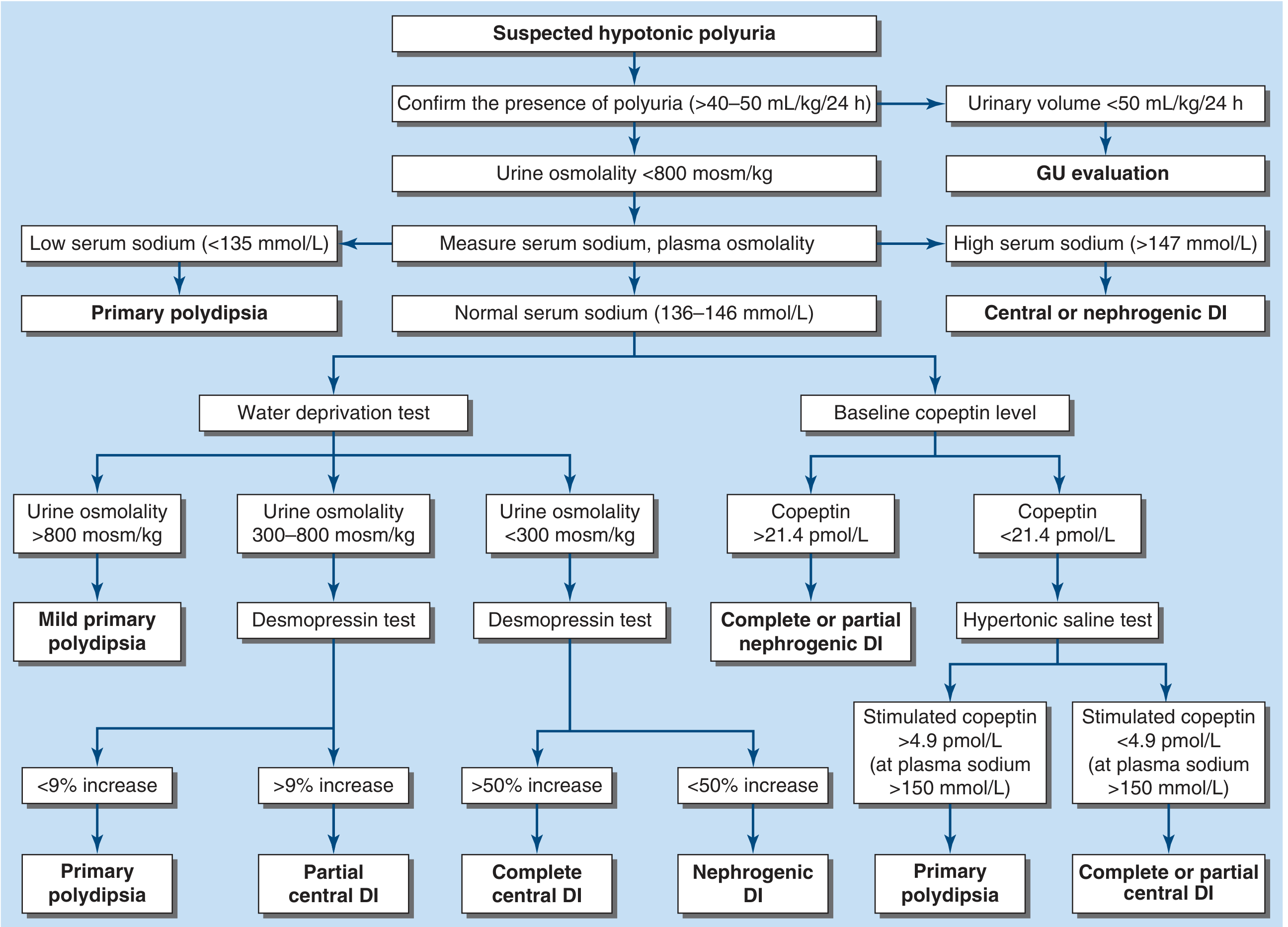
Reading the algorithm:
- Confirm polyuria (>40-50 mL/kg/24 h) + urine osmolality <800 mOsm/kg
- Measure serum sodium:
- Na <135: Primary polydipsia
- Na >147: Central or nephrogenic DI → give desmopressin to differentiate
- Na 136-146 (most patients): need further testing
- For normal Na, use two parallel pathways:
- Baseline copeptin: if >21.4 pmol/L → nephrogenic DI confirmed. If <21.4 pmol/L → proceed to hypertonic saline test
- Water deprivation test: still an option where copeptin is unavailable, but inferior
- Hypertonic saline-stimulated copeptin at Na ≥150:
-
4.9 → Primary polydipsia
- ≤4.9 → Central DI
-
Practical Takeaway
| Test | When to Use | Accuracy | Status |
|---|---|---|---|
| 24-h urine collection | First step always | Confirmatory | Essential |
| Serum Na + plasma osmolality | Initial screen | High for extremes | Essential |
| Baseline copeptin >21.4 pmol/L | Screen for nephrogenic DI | Excellent | Modern first-line |
| Hypertonic saline + copeptin | Differentiating central DI vs. primary polydipsia | 96.5% | New gold standard |
| Water deprivation + desmopressin | Where copeptin unavailable | ~70% | Still valid, second-line |
| Arginine stimulation + copeptin | Alternative to hypertonic saline | Good (slightly lower) | Emerging |
| Direct plasma AVP | Rarely used | Poor | Largely abandoned |
Bottom line: The tests in older textbooks (water deprivation, desmopressin response) are not wrong - they are still used, especially when copeptin assays are unavailable (copeptin is currently commercially available in Europe, Australia, India, and Mexico, per Harrison's). But Harrison's 22nd edition, based on the landmark 2018 NEJM copeptin trial by Fenske et al. and a 2023 NEJM arginine-stimulated copeptin study (Refardt et al.), now positions copeptin-based testing as the preferred approach when available. So all the tests you read about are relevant - you just need to understand where each one sits in the hierarchy.
This is a shared conversation. Sign in to Orris to start your own chat.