Acute intermittent porphyrias
Reading File
Finding Sources
Searching PubMed
"acute intermittent porphyria"[MeSH Terms]
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive data from multiple authoritative sources. Let me compile the full answer.
Acute Intermittent Porphyria (AIP)
Overview
Acute intermittent porphyria is the most common of the four acute hepatic porphyrias (AHPs), with a prevalence of approximately 1 in 1000-2000. It is inherited as an autosomal dominant trait with markedly reduced penetrance - only ~10% of gene carriers ever develop clinical disease, while 90% remain latent throughout life. AIP has a strong female predominance (women:men ratio 1.5:1 to 2:1) and rarely presents before puberty or after menopause, pointing to a pivotal role of sex hormones. It is particularly prevalent in Scandinavia.
Genetics and Enzyme Defect
AIP is caused by a heterozygous loss-of-function mutation in the HMBS gene (also called PBGD gene, located on chromosome 11q23), which encodes porphobilinogen deaminase (PBGD), also called hydroxymethylbilane synthase. Affected individuals have ~50% of normal PBGD enzymatic activity. Over 240 distinct mutations have been identified.
The enzyme defect sits at step 3 of the heme biosynthetic pathway:
Glycine + Succinyl-CoA → ALA (via ALAS1) → PBG (via ALAD) → Hydroxymethylbilane (via PBGD ← deficient here) → Uroporphyrinogen III → ... → Heme
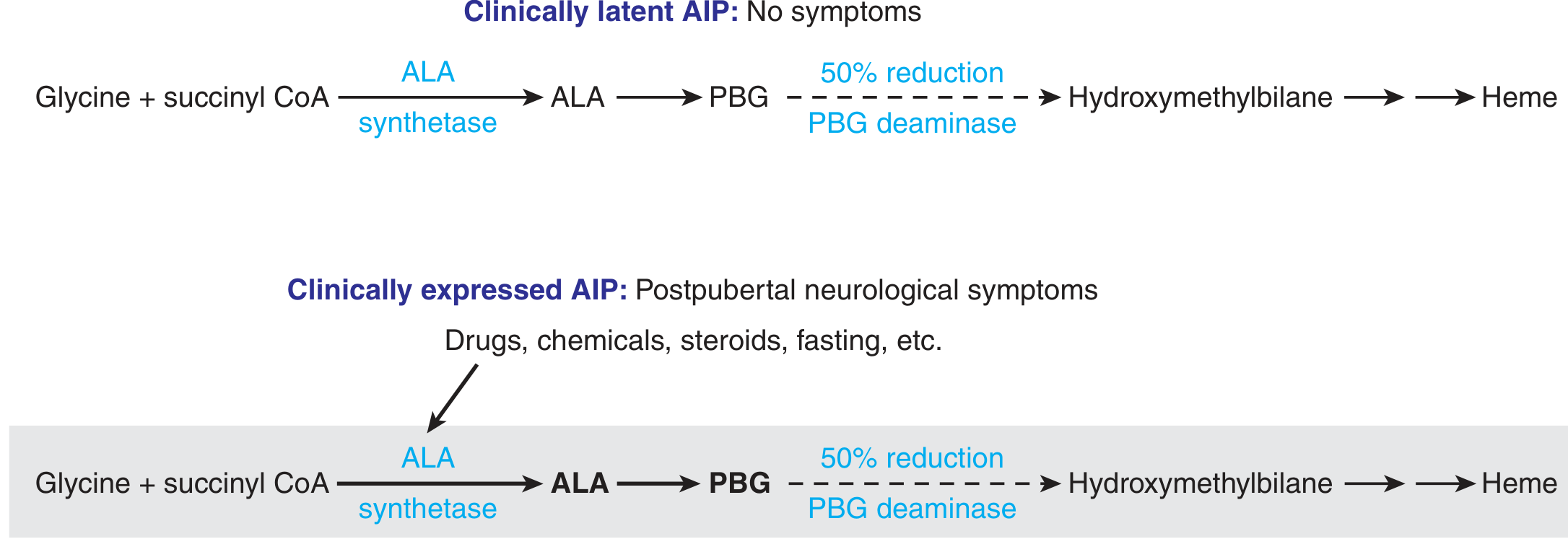
Figure: In clinically latent AIP, the 50% reduction in PBG deaminase is adequate at baseline flux. When inducing agents (drugs, steroids, fasting) upregulate hepatic ALAS1, ALA and PBG production overwhelms the reduced enzyme capacity, causing accumulation and clinical disease. - Thompson & Thompson Genetics, 9th Ed.
Pathophysiology
The central mechanism is a two-hit process:
-
Baseline enzyme insufficiency: All carriers have ~50% PBGD activity (consistent with heterozygous dominant inheritance). Homozygous deficiency would presumably be lethal.
-
Precipitant-driven ALAS1 induction: The rate-limiting enzyme of heme synthesis, ALAS1 (delta-aminolevulinic acid synthase 1), is normally feedback-regulated by free hepatic heme. When a precipitant (drug, hormone, fasting) depletes free heme or directly upregulates ALAS1 via nuclear receptor signaling (e.g., pregnane X receptor, constitutive androstane receptor), the flux of ALA and PBG through the pathway increases dramatically.
-
Bottleneck at PBGD: The elevated flux exceeds the reduced PBGD capacity, causing accumulation of ALA and PBG in plasma, urine, and tissues.
-
Neurotoxicity: ALA (structurally similar to GABA) is directly neurotoxic and disrupts the peripheral, autonomic, and central nervous systems. The pathogenesis of neurological disease is not fully resolved, but elevated ALA and PBG are always present during attacks.
-
Hyperhomocysteinemia: A secondary effect - reduced heme availability impairs the heme-dependent enzyme cystathionine-beta-synthase, elevating homocysteine. - Goldman-Cecil Medicine
Precipitating Factors (Triggers)
| Category | Examples |
|---|---|
| Drugs | Barbiturates, sulfonamides, rifampin, griseofulvin, carbamazepine, phenytoin, valproate, estrogens/progesterone |
| Hormones | Endogenous progesterone (luteal phase), oral contraceptives |
| Nutritional | Fasting, crash dieting, low-carbohydrate diets, alcohol |
| Other | Surgery, infections, smoking, emotional stress |
Drugs with CYP3A or CYP2C9 induction are particularly porphyrogenic because they increase the demand for heme-containing cytochrome P450 enzymes. A continuously updated drug safety list is maintained at www.porphyria-europe.com.
Clinical Features
The Acute Attack
The attack evolves through characteristic phases:
Prodrome: Mild behavioral disturbance, anxiety, restlessness.
Abdominal phase (cardinal presentation):
- Severe, generalized abdominal pain (95% of patients), often colicky, radiating to back/buttocks/thighs
- Nausea, vomiting, constipation or diarrhea (up to 90%)
- No abdominal rigidity (important clue - pain without peritoneal signs)
- Abdominal distension
Autonomic phase:
- Tachycardia, hypertension, sweating (sympathetic overactivity)
- Urinary retention
Neurological phase (if attack progresses):
- Peripheral neuropathy - predominantly motor (50-70%)
- Proximal limb weakness, flaccid quadriplegia in severe cases
- Diaphragmatic weakness, respiratory paralysis (life-threatening)
- Cranial nerve involvement: optic atrophy, facial palsy, dysphagia
- Seizures (10-20%)
Psychiatric features (40-60%):
- Agitation, anxiety, hallucinations, depression, confusion, psychosis
Hyponatremia is common (SIADH mechanism) - can itself trigger/worsen seizures.
Urine discoloration: Port-wine red or dark urine on standing/light exposure - characteristic of AIP.
Chronic/Long-term Complications
- Hypertension and chronic renal disease (up to 59% of symptomatic patients develop CKD)
- Hepatocellular carcinoma - markedly increased risk; hepatic imaging recommended every 6 months
- Neuropathy, fatigue, chronic pain, depression/anxiety
- Hyperhomocysteinemia
Diagnosis
During an Acute Attack
The diagnosis is straightforward during an attack:
| Test | Finding in AIP |
|---|---|
| Urine PBG (spot or 24h) | Markedly elevated (diagnostic) - PBG > ALA |
| Urine ALA | Elevated |
| Urine color | Red/port-wine after light/air exposure |
| Plasma fluorescence scan | Peak at 615-620 nm |
| Erythrocyte porphyrins | Normal (distinguishes from erythropoietic porphyrias) |
| Fecal porphyrins | Normal (distinguishes from VP and HCP) |
Between Attacks (Asymptomatic)
- Urinary PBG/ALA may be normal
- RBC PBGD enzyme activity (reduced to ~50%) - confirms carrier status in ~88%
- HMBS gene mutation analysis in leukocyte DNA - definitive; also enables family screening
Differential Diagnosis
AIP must be distinguished from:
- Variegate porphyria (VP) - elevated fecal protoporphyrin, plasma peak at 625-627 nm
- Hereditary coproporphyria (HCP) - elevated fecal coproporphyrin III
- ALA dehydratase deficiency porphyria (ALAD) - autosomal recessive, elevated ALA but normal/slight PBG, resembles AIP clinically
- Abdominal emergencies (appendicitis, bowel obstruction - no peritoneal signs in AIP)
- Lead poisoning (elevated ALA, normal PBG)
- Guillain-Barre syndrome (motor neuropathy)
Treatment
Acute Attack Management
Supportive care:
- Remove and avoid all precipitating drugs/factors
- IV fluids and electrolyte correction (especially hyponatremia)
- Narcotic analgesics (opioids) for abdominal pain
- Phenothiazines (e.g., chlorpromazine) for nausea, vomiting, anxiety
- Benzodiazepines (low dose, probably safe) for insomnia/agitation
- Chloral hydrate for insomnia
- Respiratory monitoring; ICU if motor neuropathy progresses
Carbohydrate loading:
- IV glucose ≥300 g/day suppresses ALAS1 by providing caloric substrate
- Effective in mild attacks when hemin is unavailable
- Not adequate for severe attacks with paresis or hyponatremia
IV Hemin (first-line specific therapy):
- Standard regimen: 3-4 mg/kg/day for 4 days
- Available as: lyophilized hemin (Panhematin), heme arginate (Orphan Europe, preferred in Europe - more stable, less phlebitis), or heme albumin
- Repletes the free hepatic heme pool, suppresses ALAS1, reduces ALA and PBG production
- FDA approved since 1984
- Early treatment produces best outcomes; recovery from motor neuropathy may take months to years if delayed
Long-term/Prophylactic Therapy
Givosiran (Givlaari) - RNAi therapy:
- FDA and EMA approved in 2019 for acute hepatic porphyrias
- Mechanism: siRNA that silences hepatic ALAS1 mRNA, reducing ALA and PBG production at source
- Dose: 2.5 mg/kg subcutaneously once monthly
- Phase 3 trial showed significant reduction in attack frequency, reduced hemin utilization, improved daily pain scores
- Currently first-line for patients with recurrent attacks - Harrison's 22E (2025)
Prevention of cyclic attacks:
- GnRH analogue (e.g., leuprolide) - prevents ovulation and progesterone production; effective for perimenstrual attacks
- Prophylactic hemin infusions
- Givosiran
Advanced/Refractory Cases
Orthotopic liver transplantation (OLT):
- Corrects the hepatic enzyme defect - the liver is the principal site of ALA/PBG overproduction
- Indicated for severe, disabling, treatment-refractory attacks
- Results in normalization of urinary PBG/ALA, no further attacks, improvement in neuropathy
- Associated with significant morbidity/mortality - last resort
- Some patients with both recurrent attacks and end-stage renal disease have benefited from combined liver-kidney transplantation
Liver-directed gene therapy:
- Under investigation (promising early results)
Summary Table: AIP vs. Other Acute Porphyrias
| Feature | AIP | VP | HCP |
|---|---|---|---|
| Enzyme defect | PBGD (HMBS) | PPOX | CPOX |
| Inheritance | AD | AD | AD |
| Neurovisceral | +++ | +++ | +++ |
| Skin lesions | None | +/- | +/- |
| Urine ALA/PBG | Both ↑↑ | Both ↑↑ | Both ↑↑ |
| Fecal porphyrins | Normal | PPOX + copro III ↑ | Copro III ↑ |
| Plasma fluorescence | 615-620 nm | 625-627 nm | 615-620 nm |
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
- Goldman-Cecil Medicine, International Ed.
- Thompson & Thompson Genetics & Genomics in Medicine, 9th Ed.
- Andrews' Diseases of the Skin, Clinical Dermatology
- Yamada's Textbook of Gastroenterology, 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.