Dual anti platelets ticaglor and aspirin for inferior stemi
Reading File
Finding Sources
Finding Sources
Searching PubMed
ticagrelor aspirin STEMI dual antiplatelet
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
I have comprehensive information from multiple authoritative sources. Here is a detailed, well-structured answer:
Dual Antiplatelet Therapy (DAPT): Ticagrelor + Aspirin in Inferior STEMI
Rationale for DAPT
Aspirin alone exerts only modest platelet inhibition via irreversible COX-1 inhibition, reducing thromboxane A2 synthesis. Adding a P2Y12 receptor antagonist — forming DAPT — provides more potent, complementary antiplatelet action by blocking ADP-mediated platelet activation. This is critical in STEMI because the culprit plaque rupture triggers intense platelet aggregation and thrombus formation regardless of the infarct territory (inferior, anterior, lateral).
Inferior STEMI does not change the DAPT regimen — the evidence base and guideline recommendations apply uniformly to all STEMI presentations.
Ticagrelor: Mechanism & Pharmacology
Ticagrelor is a reversible, direct-acting P2Y12 receptor antagonist (cyclopentyl-triazolo-pyrimidine class) — it does not require hepatic activation (unlike clopidogrel/prasugrel). Key pharmacokinetic features:
| Property | Detail |
|---|---|
| Onset of action | Rapid; peak plasma concentration ~2.5 hours |
| Binding | Reversible (allosteric) |
| Duration of effect | Prolonged — platelet function recovers over ~3–5 days after last dose |
| Dosing (STEMI) | 180 mg loading dose, then 90 mg twice daily |
| Hold before surgery | 5 days pre-operatively |
Because it doesn't require CYP conversion, there is no genetic variability in response (unlike clopidogrel's CYP2C19 poor-metabolizer issue).
Key Evidence: The PLATO Trial
The pivotal trial is PLATO (Platelet Inhibition and Patient Outcomes):
- n = 18,624 patients with ACS; 38% had STEMI
- Ticagrelor 180 mg load → 90 mg BID vs. clopidogrel 300–600 mg load → 75 mg daily
- ~2/3 underwent PCI
Results at 12 months:
- 16% relative reduction in composite of vascular death, MI, or stroke with ticagrelor (9.8% vs 11.7%)
- CV death alone reduced (4.0% vs 5.1%; HR 0.79)
- Major bleeding unrelated to CABG: slightly higher with ticagrelor (4.5% vs 3.8%; P = 0.03)
- Fatal intracranial bleeding: higher with ticagrelor
- Stroke in STEMI subgroup: slightly higher with ticagrelor (1.7% vs 1.0%; P = 0.02) — a signal requiring attention
— Fuster and Hurst's The Heart, 15th Ed., p. 610
Dosing Regimen
| Drug | Loading Dose | Maintenance Dose | Duration |
|---|---|---|---|
| Aspirin | 162–325 mg (non-enteric-coated, chewed) | 75–100 mg daily | Indefinitely |
| Ticagrelor | 180 mg PO | 90 mg PO twice daily | 12 months |
- Aspirin should be non-enteric-coated in the acute setting to ensure rapid absorption
- IV aspirin 150 mg is an alternative for those unable to swallow (European guidelines)
- DAPT duration: 12 months is the standard recommendation for all STEMI patients regardless of revascularization strategy, absent high bleeding risk
"Dual antiplatelet therapy with aspirin and a P2Y12 receptor antagonist (clopidogrel, prasugrel, or ticagrelor) is recommended for 12 months after a STEMI, in the absence of high bleeding risk or the occurrence of bleeding complications."
— Harrison's Principles of Internal Medicine, 22nd Ed., p. 2169
Ticagrelor vs. Alternatives in STEMI
| Agent | Benefit | Key Limitation |
|---|---|---|
| Clopidogrel | Only agent with fibrinolytic data; well-studied; cheaper | CYP2C19 variability; slower onset; less potent |
| Prasugrel | Greater anti-ischemic effect vs clopidogrel (TRITON-TIMI 38) | Higher bleeding; contraindicated in prior stroke/TIA; caution ≥75 yr or <60 kg |
| Ticagrelor | Reduced CV mortality vs clopidogrel (PLATO); no genetic variability | Twice-daily dosing; dyspnea (adenosine-mediated, ~15%); slightly higher intracranial bleeding |
| Cangrelor | IV, immediate onset; useful if unable to take oral meds or urgent CABG | IV only; short half-life (4–6 min); role still being defined |
Important: Ticagrelor and prasugrel are NOT recommended when fibrinolytic therapy is used — clopidogrel remains the only P2Y12 inhibitor indicated in the pharmaco-invasive strategy.
Timing in Inferior STEMI with Primary PCI
- Ticagrelor 180 mg loading dose should be given as early as possible — ideally at first medical contact / in the ED, before the patient reaches the cath lab
- Note: Despite rapid absorption, >30% of STEMI patients receiving a ticagrelor loading dose may show high residual platelet reactivity for up to 2 hours post-ingestion — likely due to delayed gastric emptying in the acute setting. Some centers bridge with IV cangrelor in this window
DAPT De-escalation and Duration Adjustments
Shortening DAPT (6 months)
- The DAPT-STEMI trial (n = 870) showed 6-month DAPT was non-inferior to 12 months in selected low-risk patients — but results must be interpreted cautiously (observed event rates far lower than projected)
- A larger ACS trial showed 6-month DAPT → higher MI rates vs. longer duration (1.8% vs 0.8%; P = 0.02)
- Current guidance: do not discontinue P2Y12 inhibition before 6 months post-STEMI
Aspirin-free strategy ("ticagrelor monotherapy")
Emerging data supports 1–3 months DAPT → ticagrelor alone:
- GLOBAL LEADERS (n = 15,968): 1 month DAPT → ticagrelor monotherapy reduced major bleeding by 48% vs standard DAPT (no difference in death/Q-wave MI)
- TICO trial: 3 months DAPT → ticagrelor monotherapy showed reduced MACE + bleeding vs 12-month DAPT
- Individual patient data meta-analysis (Ann Intern Med 2025, PMID 39961108): De-escalation to ticagrelor monotherapy associated with reduced bleeding without increase in ischemic events
This aspirin-dropping strategy is supported by pharmacodynamic data showing aspirin adds minimal incremental inhibition when ticagrelor is present at therapeutic levels.
Extended DAPT (>12 months)
- In PEGASUS-TIMI 54 (~53% had prior STEMI): aspirin + ticagrelor 60 mg BID for up to 3 years after MI reduced MACE (absolute risk reduction ~1%) at the cost of more bleeding
- Suitable only for high-ischemic/low-bleeding-risk patients beyond 1 year
Contraindications & Special Situations
| Situation | Recommendation |
|---|---|
| Prior intracranial hemorrhage | Ticagrelor contraindicated |
| Active pathological bleeding | Contraindicated |
| Severe hepatic impairment | Avoid ticagrelor |
| Planned CABG | Hold ticagrelor 5 days before surgery |
| Patient on oral anticoagulant (e.g., AF + STEMI) | Triple therapy: minimize duration; prefer clopidogrel over ticagrelor to reduce bleeding in combination |
| Age ≥75 years | Ticagrelor still preferred over prasugrel; weigh bleeding risk |
| Fibrinolysis given | Use clopidogrel, NOT ticagrelor |
Unique ticagrelor side effect — Dyspnea: Adenosine-mediated, non-bronchospastic; usually self-limiting. Occurs in ~15% — do not discontinue for this alone unless severe.
Summary
In inferior STEMI managed with primary PCI:
- Aspirin 162–325 mg (chewed, non-enteric) + Ticagrelor 180 mg loading dose as early as possible
- Continue aspirin 75–100 mg daily + ticagrelor 90 mg BID for 12 months
- Ticagrelor is preferred over clopidogrel (higher efficacy, no CYP variability) and over prasugrel (lower bleeding risk, suitable for older/lighter patients)
- Consider ticagrelor monotherapy after 1–3 months in high-bleeding-risk patients
- Do not use ticagrelor if fibrinolysis was the reperfusion strategy — use clopidogrel instead
Recent evidence (PMID 39654024 — BMC Pharmacol Toxicol, 2024): Meta-analysis of RCTs confirms ticagrelor reduces major adverse cardiac events compared to clopidogrel in STEMI, with consistent mortality benefit and manageable bleeding risk.
Sources: Fuster and Hurst's The Heart 15th Ed. | Harrison's Principles of Internal Medicine 22nd Ed. | Goodman & Gilman's Pharmacological Basis of Therapeutics | Rosen's Emergency Medicine | Tintinalli's Emergency Medicine
How to assess dermatones for upper and lower limbs
Reading File
Finding Sources
Finding Sources
Searching Images
dermatome map upper limb lower limb sensory assessment
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive, well-illustrated answer. Here it is:
Dermatome Assessment: Upper & Lower Limbs
What Is a Dermatome?
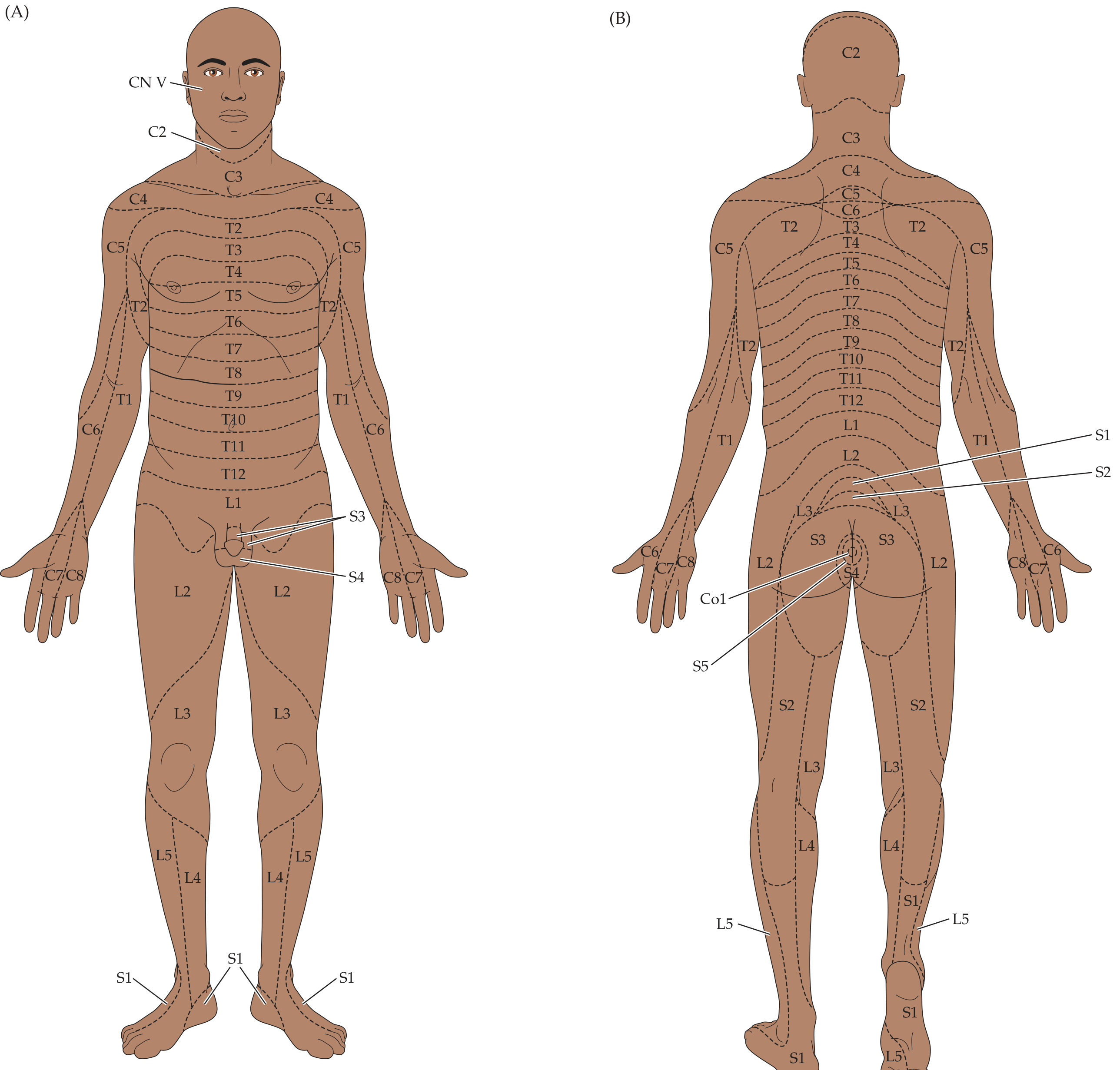
A dermatome is the area of skin innervated by a single spinal cord segment (nerve root). Because dermatomes in the limbs arise from plexus formation during embryonic development — where migrating primordia drag their segmental innervation along — the pattern is not simply horizontal as on the trunk. Adjacent dermatomes overlap considerably, so a single nerve root lesion typically causes reduced, not absent, sensation in a given area.
"There is considerable overlap between adjacent dermatomes, so lesions of a single nerve root ordinarily cause a decrease but not a complete loss of sensation in a given dermatome. There may be less overlap for smaller fibers, so pinprick is a more sensitive test for dermatomal sensory loss than touch." — Neuroanatomy Through Clinical Cases, 3rd Ed.
Dermatome Maps
Anterior and posterior full-body dermatome map (from Neuroanatomy Through Clinical Cases, 3rd Ed.):
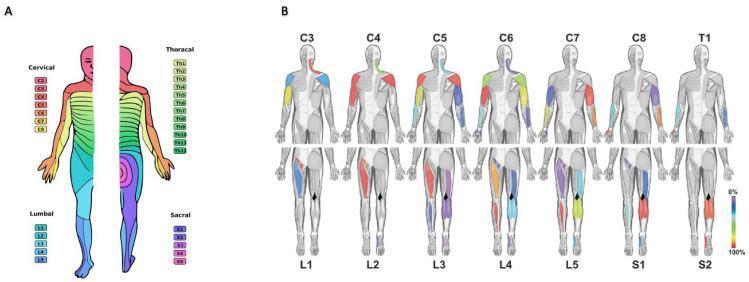
Colour-coded dermatomes and myotomes by spinal level (anterior/posterior views with muscle maps):
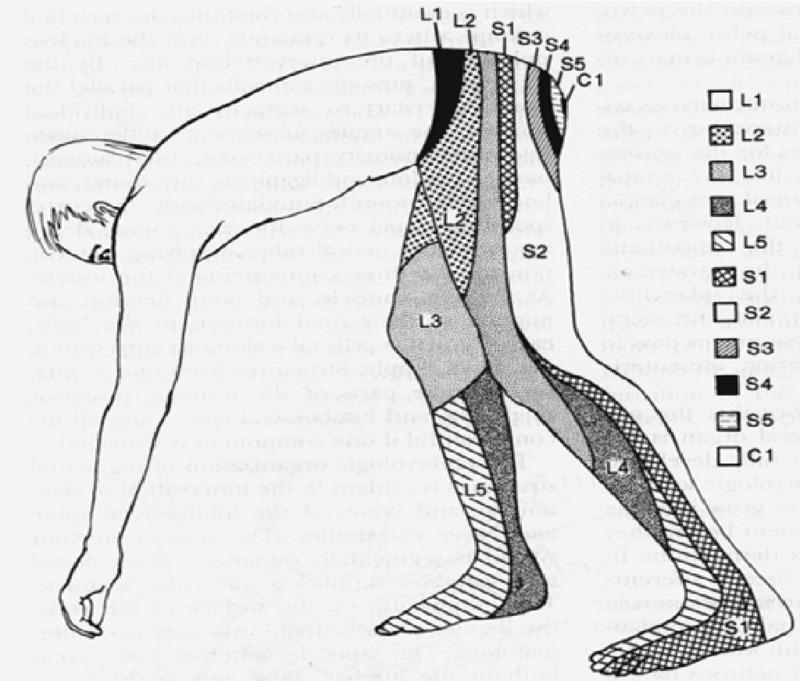
Lumbosacral dermatomes — posterior view:
How to Assess Dermatomes — Method
Tools Used
| Modality | Instrument | Pathway Tested |
|---|---|---|
| Pinprick | Disposable pin or broken wooden applicator | Spinothalamic (pain/temperature) — A-delta and C fibres |
| Light touch | Cotton wool | Posterior column (tactile) |
| Temperature | Cold/warm objects (e.g., tuning fork base) | Spinothalamic |
| Vibration | 128 Hz tuning fork over bony prominences | Posterior column |
| Proprioception | Passive joint movement | Posterior column |
Pinprick is the most sensitive modality for detecting dermatomal sensory loss due to less inter-root overlap of small fibres. Light touch is less reliable in isolation.
General Technique
- Expose the limb fully. Compare left vs. right symmetrically at each level.
- Establish baseline — test a clearly normal area first (face or chest) so the patient knows what normal feels like.
- Apply the stimulus at standardised landmark points for each dermatome (see tables below).
- Ask the patient: "Does this feel sharp/normal/less than the other side?"
- Map any deficit by moving from the abnormal area toward normal, rather than normal → abnormal (patients are more sensitive to detection of return of sensation).
- Document as: normal / reduced / absent / hyperaesthetic / allodynia.
Upper Limb Dermatomes (C5–T1)
Note: There is a normal gap between C4 and T2 on the trunk — C5 through T1 are represented entirely on the upper limb.
| Root | Key Landmark / Test Area | Associated Reflex | Key Muscles (Myotome) |
|---|---|---|---|
| C5 | Lateral arm / deltoid patch (regimental badge area) | Biceps jerk | Deltoid, biceps (shoulder abduction, elbow flexion) |
| C6 | Lateral forearm, thumb and index finger (first 2 digits) | Biceps / brachioradialis jerk | Wrist extensors, biceps |
| C7 | Middle finger (3rd digit) | Triceps jerk | Triceps, wrist flexors, finger extensors |
| C8 | Ring and little finger (4th & 5th digits), medial hand | — | Finger flexors, intrinsics |
| T1 | Medial forearm / elbow | — | Intrinsic hand muscles (interossei) |
Landmarks summary (Rosen's Emergency Medicine table):
| Level | Sensory Landmark |
|---|---|
| C5 | Below the clavicle |
| C6 | Thumb |
| C7 | Index finger |
| C8 | Small (little) finger |
Reflexes for upper limb:
- C5–C6 → Biceps jerk
- C6 → Brachioradialis (supinator) jerk
- C7 → Triceps jerk
Lower Limb Dermatomes (L1–S2)
| Root | Key Landmark / Test Area | Associated Reflex | Key Muscles (Myotome) |
|---|---|---|---|
| L1 | Inguinal region / femoral pulse area | — | Hip flexors (partially) |
| L2 | Anterior mid-thigh, medial thigh | — | Hip flexion (iliopsoas), hip adduction |
| L3 | Distal anterior thigh, medial knee | Knee jerk (shared with L4) | Quadriceps (knee extension) |
| L4 | Anteromedial shin / medial lower leg, medial ankle | Patellar (knee) jerk | Tibialis anterior (ankle dorsiflexion), quadriceps |
| L5 | Anterolateral shin, dorsum of foot, big toe (first web space) | — (no consistent reflex) | Extensor hallucis longus (great toe extension) |
| S1 | Lateral foot, small toe, sole, lateral heel, calf | Ankle (Achilles) jerk | Gastrocnemius/soleus (plantar flexion), peronei |
| S2 | Posterior thigh, popliteal fossa | — | Bladder/bowel sphincters (with S3–S4) |
Landmarks summary (Rosen's Emergency Medicine table):
| Level | Sensory Landmark |
|---|---|
| L1 | Femoral pulse area |
| L2–L3 | Medial aspect of thigh |
| L4 | Knee |
| L5 | Lateral aspect of calf |
| S1 | Lateral aspect of foot |
| S2–S4 | Perianal region (saddle anaesthesia) |
Key reflexes for lower limb:
- L3–L4 → Patellar (knee) jerk
- S1 → Achilles (ankle) jerk — note: absent in ~50% of those >80 years (bilaterally), so unilateral absence is more significant
Practical Mnemonics
Upper limb (C5–T1):
"Sit Down, Miss Pinky, Thank you"
- C5 = Shoulder/deltoid
- C6 = Thumb & index (lateral)
- C7 = Middle finger
- C8 = Pinky & ring (medial hand)
- T1 = medial forearm
Lower limb (L1–S1):
"I Go Kick, Let's Start"
- L1 = Inguinal
- L2 = Groin/upper thigh
- L3 = Knee area (medial)
- L4 = Lateral shin / Leg medial
- L5 = Lateral shin + dorsum of foot
- S1 = Sole + lateral foot
Common Clinical Pitfalls
| Issue | Explanation |
|---|---|
| Dermatomal overlap | A single root lesion rarely causes complete sensory loss — only a reduction. Two adjacent roots must be affected for a clear deficit to be clinically apparent |
| Root vs. peripheral nerve | Radiculopathy follows dermatomal distribution; peripheral nerve injury follows the territory of that specific nerve (e.g., carpal tunnel = median nerve distribution, not C6 alone) |
| Unreliable ankle reflexes in elderly | Bilaterally absent ankle jerks are physiological in >65 yrs. Focus on asymmetry |
| L5 has no reflex | L5 radiculopathy is the most common disc lesion (L4–5 level) but has no reliable associated deep tendon reflex — motor (great toe extension) and sensory (1st web space) are your primary tools |
| Non-organic loss | Stocking/glove pattern, non-dermatomal, or variable sensory loss suggests a functional cause |
Provocative Tests to Support Dermatomal Findings
| Test | Positive Finding | Significance |
|---|---|---|
| Straight leg raise (SLR) | Radicular pain below knee at 30–70° elevation | L4–S1 nerve root irritation (sens. 72–97%) |
| Crossed SLR | Contralateral leg raises reproduces ipsilateral radicular pain | Highly specific for disc herniation (spec. 85–100%) |
| Braggart sign | SLR positive, lower leg, ankle dorsiflexion reproduces pain | Confirms nerve root stretch |
| Spurling's test (upper limb) | Neck extension + rotation + axial load → radicular arm pain | Cervical foraminal stenosis |
| Femoral stretch test | Prone, passive hip extension → anterior thigh pain | L2–L3–L4 radiculopathy |
Sources: Neuroanatomy Through Clinical Cases 3rd Ed. | Rosen's Emergency Medicine | Goldman-Cecil Medicine International Edition | General Anatomy and Musculoskeletal System — Thieme Atlas of Anatomy
This is a shared conversation. Sign in to Orris to start your own chat.