Hernia. Clinical classification. General characteristics of hernia.Rare forms of hernia. Everything in detail
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive, textbook-based overview of hernia — clinical classification, general characteristics, and rare forms.
Hernia: Clinical Classification, General Characteristics, and Rare Forms
1. Definition and General Characteristics
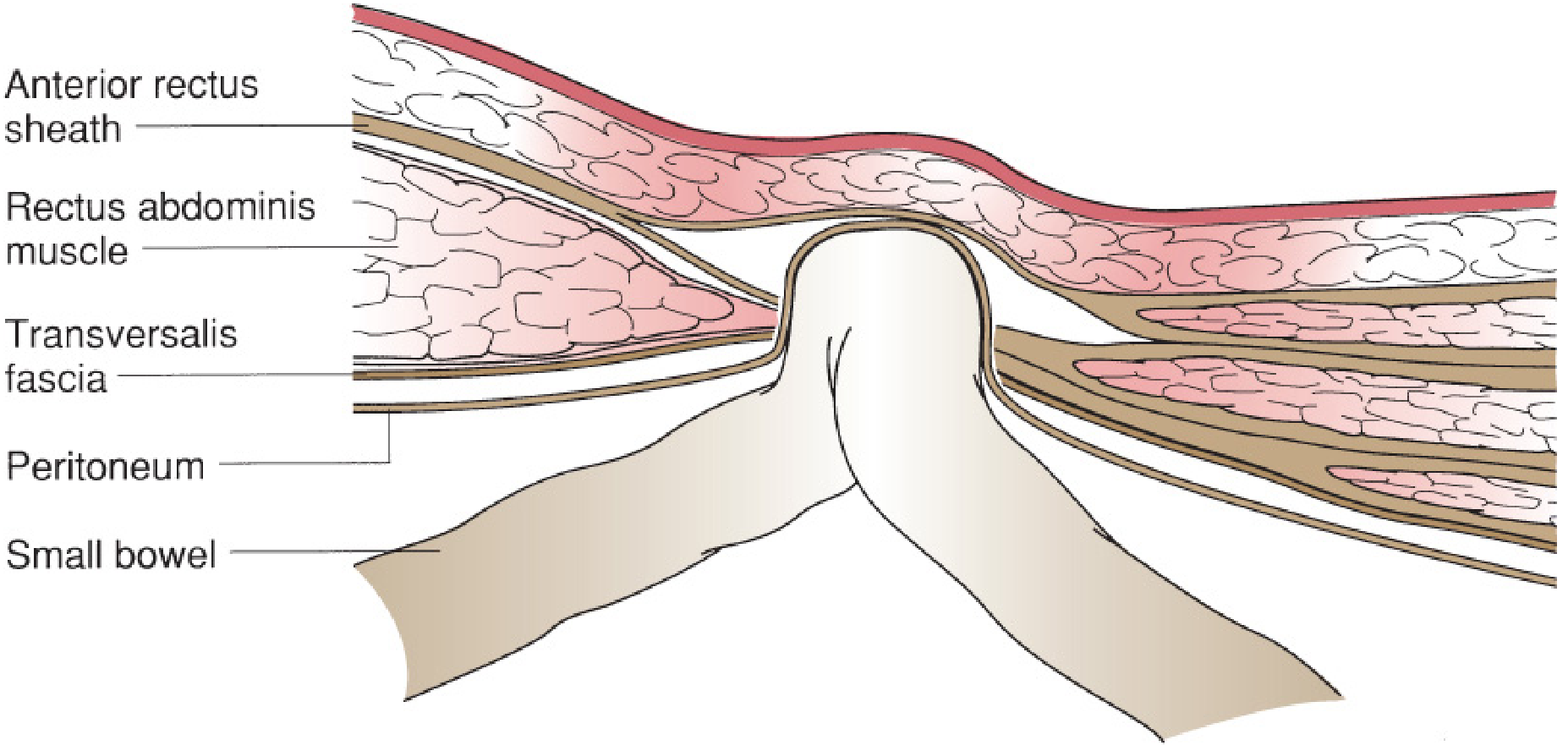
A hernia is the protrusion of a viscus, or part of a viscus, through a defect in the wall of the cavity in which it is normally contained. Every hernia has three anatomical components:
| Component | Description |
|---|---|
| Sac | A peritoneal diverticulum that envelops the hernia contents; has a neck, body, and fundus |
| Neck | The narrowest part at the hernia orifice; determines the risk of incarceration |
| Contents | Typically omentum, small bowel, or large bowel; rarely bladder, ovary, or appendix |
Abdominal hernias form in regions where the muscular and fascial wall is inherently weak:
- The inguinal region (the most common site)
- The femoral canal
- The umbilicus
- Surgical incision sites
- Natural foramina (obturator, sciatic, esophageal hiatus)
The abdominal wall is reinforced by layered muscles running at oblique angles to each other. In the groin, the external and internal oblique muscles thin to a fascial aponeurosis only, leaving no muscular support of the transverse abdominal fascia and the peritoneum. Upright posture and transient rises in intra-abdominal pressure (cough, straining, lifting) are directed to this area continuously.
2. Clinical Classification
A. By Etiology
| Type | Description |
|---|---|
| Congenital | Result of developmental failure (e.g., patent processus vaginalis → indirect inguinal hernia; paraduodenal hernia through foramen of Winslow) |
| Acquired | Result of chronic mechanical stress, aging, obesity, collagen disorders, prior surgery |
B. By Location
External (Abdominal Wall) Hernias
These are visible or palpable externally.
- Inguinal hernia — most common overall (75% of all hernias); further divided into:
- Indirect inguinal hernia: passes through the deep inguinal ring lateral to the inferior epigastric vessels, travels with the spermatic cord; associated with a patent processus vaginalis; the processus vaginalis persists in 12–20% of adults
- Direct inguinal hernia: protrudes through Hesselbach triangle (bounded medially by rectus abdominis, laterally by inferior epigastric artery, inferiorly by inguinal ligament) in the floor of the inguinal canal; medial to inferior epigastric vessels; not congenital
- Femoral hernia: passes through the femoral canal, inferior to the inguinal ligament, medial to the femoral vein, lateral to the lacunar ligament; more common in women; small fascial defect means incarceration in up to 45% of cases; strangulated at presentation in up to 40%
- Umbilical hernia: traverses the fibromuscular umbilical ring; common in infants (usually closes spontaneously by age 5), obese adults, and multiparous women
- Epigastric hernia: through a defect in the linea alba between the xiphoid and the umbilicus; contents often just preperitoneal fat
- Incisional (ventral) hernia: occurs at any prior laparotomy wound; affects up to 20% of patients after laparotomy; rate rises to 35–50% after wound infection or dehiscence; up to 50% manifest >1 year postoperatively; vertical midline incisions carry higher risk than transverse
- Spigelian hernia: through the semilunar line (lateral border of rectus sheath) at the level of the arcuate line; typically occurs in patients aged 40–70; incarceration rates up to 20%
- Parastomal hernia: occurs at the exit point of an intentional stoma through the abdominal wall; reported in up to 50% of stoma placements
- Trocar-site hernia: complication of minimally invasive surgery; trocar sites >10 mm in diameter are most at risk
Internal Hernias
Occur at natural or iatrogenic openings within the peritoneum, mesentery, or omentum; often discovered at laparotomy.
- Paraduodenal hernia — most common congenital internal hernia
- Hernia through the foramen of Winslow (epiploic foramen, posterior to the porta hepatis)
- Mesocolic hernias — increasingly seen after Roux-en-Y gastric bypass, colectomy, or pancreaticoduodenectomy (iatrogenic division of mesentery)
- Obturator, sciatic, perineal hernias — described below under rare forms
C. By Reducibility (Clinical Status)
This is the most clinically important classification:
| Status | Definition | Clinical Significance |
|---|---|---|
| Reducible | Contents can spontaneously or manually be returned to their normal position | Elective repair; much lower morbidity than emergency repair |
| Irreducible (Incarcerated) | Contents cannot be reduced; fixed in the hernia sac | Not automatically a surgical emergency; wide-necked hernias may incarcerate without compromise |
| Obstructed | Incarcerated bowel with luminal obstruction but no vascular compromise | Surgical emergency |
| Strangulated | Vascular compromise of the herniated contents (ischemia or gangrene) | True surgical emergency; mortality increases rapidly |
The thin-walled veins and lymphatics are compressed before the thick-walled arterial supply. Free fluid in the hernia sac on ultrasound is a sensitive sign of strangulation (elevated intravascular pressure → fluid extravasation).
Strangulation risk by hernia type:
- Femoral: up to 40% strangulated at presentation
- Umbilical: up to 60% strangulated at emergency surgery
- Incisional: only ~2% strangulated (large orifice)
- Smaller hernias carry higher strangulation risk because the narrow neck compresses contents more readily
D. By Completeness of Bowel Wall Involvement
| Subtype | Description |
|---|---|
| Complete (classical) | The full circumference of the bowel loop herniates |
| Richter hernia | Only the antimesenteric border (a portion of the bowel wall circumference) herniates — see Rare Forms |
| Littre hernia | A Meckel diverticulum is the herniated content |
| Maydl hernia (W-hernia) | Two adjacent loops of bowel (forming a "W") herniate; the intervening loop within the abdomen may strangulate even though the herniated loops appear viable |
E. By Anatomy — The Nyhus/Rutkow Classification (Inguinal Hernias)
A widely used grading system for inguinal hernias:
| Type | Description |
|---|---|
| I | Indirect; internal ring normal in size; pediatric |
| II | Indirect; internal ring dilated; posterior wall intact |
| IIIa | Direct hernia |
| IIIb | Indirect; large defect compromising posterior wall |
| IIIc | Femoral hernia |
| IV | Recurrent hernia |
F. European Hernia Society (EHS) Classification of Incisional Hernia
Classifies by location (midline vs. lateral) and width of fascial defect (W1 <4 cm, W2 4–10 cm, W3 >10 cm).
3. Rare Forms of Hernia
Richter Hernia
Richter hernia: part of the bowel wall herniates through the defect without involving the full circumference — Mulholland & Greenfield's Surgery, 7e
First described by August Gottlieb Richter in 1785. Only the antimesenteric border of the intestine protrudes into the hernia sac, without involving the entire circumference.
Key features:
- No complete bowel obstruction (lumen is not fully occluded) — therefore, vomiting and classic obstruction signs may be absent
- Strangulation and gangrene occur more frequently than with standard hernias, precisely because it is not recognized early
- Most common site: femoral ring (36–88%), followed by inguinal canal (12–36%), abdominal wall incision (4–25%)
- Also reported at umbilical, obturator, Spigelian, trocar sites (increasingly common with laparoscopic surgery)
- Treatment: open the sac, enlarge the neck, excise any gangrene, reconstitute the bowel wall, repair the hernia
Pantaloon (Saddle-Bag) Hernia
A combination of both direct and indirect inguinal hernia on the same side, with the hernias straddling the inferior epigastric vessels. Difficult to diagnose clinically; often discovered during surgical exploration. Difficult to achieve sustained reduction using standard manual techniques.
Spigelian Hernia
An interparietal hernia through the semilunar line (junction of rectus sheath and aponeurosis of the transversus abdominis), typically at or below the level of the arcuate line. The hernia lies between muscle layers and is not subcutaneous — hence it is difficult to palpate and is often diagnosed by CT or ultrasound. Age of onset: typically 40–70 years. Incarceration rates up to 20%, often containing omentum. Requires surgical correction.
Obturator Hernia
Herniation through the obturator canal (formed by the obturator foramen and obturator membrane), then between the pectineus, adductor longus, and obturator externus muscles.
- Classic patient: elderly, frail, cachectic, multiparous woman ("little old lady's hernia")
- The obturator foramen is larger in women; marked weight loss removes the protective fat pad
- Accounts for ~1% of all hernias in Asia; 0.07% in the West; ~800 cases reported
- Almost always presents as small bowel obstruction; Richter type is common
- Specific signs:
- Howship-Romberg sign: paresthesia/pain along the medial thigh (obturator nerve compression), worsened by hip extension/adduction/medial rotation, relieved by hip flexion; present in 25–50% and considered pathognomonic
- Hannington-Kiff sign: absent adductor reflex on percussion above the knee — strong indicator of obturator nerve impingement
- Diagnosis: CT of abdomen/pelvis (often not made preoperatively)
- Complication rate: perforation in >50%, mortality approaching 20%
Sciatic Hernia
Herniation through the greater sciatic foramen, subdivided by relation to the piriformis muscle:
| Subtype | Path |
|---|---|
| Suprapiriformis | Above the piriformis muscle |
| Infrapiriformis | Below the piriformis muscle |
| Spinotuberous | In front of the sacrotuberous ligament |
- Rarest of the pelvic hernias: fewer than 100 cases reported worldwide
- More common in older women; occasionally in children
- May contain ovary, ureter, bladder, or small/large bowel
- Abnormal development or atrophy of the piriform muscle predisposes
- May present as a gluteal mass or as bowel obstruction
Perineal Hernia
Herniation through the pelvic floor musculature:
| Type | Pathway |
|---|---|
| Anterior perineal | Through the urogenital diaphragm (anterior to deep transverse perineal muscle) |
| Posterior perineal | Behind the deep transverse perineal muscle |
| Ischioanal (ischiocectal) | Through the levator ani into the ischioanal fossa |
- Primary: usually middle-aged women; very rare
- Secondary (postoperative): after abdominoperineal resection (<1% of cases), pelvic exenteration (<3%), hysterectomy; predisposed by radiation, wound infection, and obesity
- Presents as a perineal bulge or bowel obstruction
Lumbar Hernia
Herniation in the posterolateral abdominal wall between the 12th rib and iliac crest.
| Subtype | Triangle |
|---|---|
| Superior lumbar hernia (Grynfeltt-Lesshaft) | Superior costolumbar triangle — between 12th rib and iliocostalis muscle; larger, more common |
| Inferior lumbar hernia (Petit's triangle) | Between the iliac crest, latissimus dorsi, and external oblique muscles |
- May be congenital (associated with renal agenesis, skeletal anomalies) or acquired (trauma, prior surgery, infection)
- Typically contains retroperitoneal fat, but bowel may herniate
Hernia through the Foramen of Winslow (Epiploic Foramen Hernia)
Herniation of bowel into the lesser sac through the epiploic foramen (posterior to the porta hepatis, anterior to the inferior vena cava). Presents as bowel obstruction. Most often involves the terminal ileum or right colon. Surgical reduction and closure of the foramen is required.
Paraduodenal Hernia
The most common congenital internal hernia, occurring in peritoneal recesses adjacent to the fourth part of the duodenum. Left-sided is more common (Waldeyer's fossa). Presents as recurrent or acute small bowel obstruction. Surgical repair is required.
Hernia through the Broad Ligament (Internal Hernia, Female)
Herniation of small bowel through a defect in the broad ligament of the uterus. Extremely rare; presents as acute bowel obstruction; diagnosed intraoperatively.
4. Summary Table — Rare and Special Hernia Forms
| Hernia | Location | Classic Patient | Key Feature |
|---|---|---|---|
| Richter | Femoral ring (most common), inguinal, trocar sites | Any adult | Only antimesenteric wall herniates; strangulation without obstruction |
| Littre | Any groin hernia | Any adult | Contains Meckel diverticulum |
| Maydl (W) | Any | Any adult | Intervening loop strangulates while herniated loops appear viable |
| Pantaloon | Inguinal | Males | Combined direct + indirect; straddles inferior epigastric vessels |
| Spigelian | Semilunar line at arcuate line | 40–70 yrs | Interparietal; not subcutaneous; high incarceration rate |
| Obturator | Obturator canal | Elderly cachectic woman | Howship-Romberg sign; SBO; 20% mortality |
| Sciatic | Greater sciatic foramen | Elderly woman | <100 cases reported; gluteal mass or SBO |
| Perineal | Pelvic floor | Middle-aged woman (primary); post-APR (secondary) | Perineal bulge |
| Lumbar – Grynfeltt | Superior costolumbar triangle | Adults | Posterolateral wall, above iliac crest |
| Lumbar – Petit | Inferior iliolumbar triangle | Adults | Between latissimus, external oblique, iliac crest |
| Foramen of Winslow | Epiploic foramen | Any | Bowel in lesser sac; right colon/terminal ileum |
| Paraduodenal | Waldeyer's/other paraduodenal fossae | Any | Most common congenital internal hernia |
Sources: Mulholland & Greenfield's Surgery, 7e; Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Tintinalli's Emergency Medicine; Roberts & Hedges' Clinical Procedures in Emergency Medicine; THIEME Atlas of General Anatomy and Musculoskeletal System; Goldman-Cecil Medicine.
Risk factor
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Excellent — I now have complete, authoritative data from textbooks. Here is the full answer.
Risk Factors for Hernia
Risk factors operate through two fundamental mechanisms: (1) increased intra-abdominal pressure that forces contents through weak points, and (2) defective abdominal wall integrity due to connective tissue/collagen abnormalities. Both often coexist in the same patient.
1. Demographic / Non-Modifiable Factors
Male Sex
The most powerful risk factor for inguinal hernia. Men have a lifetime risk ~27% vs ~3% in women. The inguinal canal is larger in men (transmits spermatic cord vs. round ligament), and testicular descent creates an inherent weakness at the deep inguinal ring.
Increasing Age
Hernia prevalence follows a bimodal pattern — an initial peak at 0–5 years (patent processus vaginalis) and a second major peak at 70–80 years (progressive collagen degradation and abdominal wall atrophy). In Denmark's nationwide registry of 90,648 operations, >4% of all males aged 75–80 were operated for a groin hernia at least once.
Family History
A positive family history increases the risk of inguinal hernia up to 8 times. This reflects inherited connective tissue abnormalities affecting collagen synthesis and matrix metalloproteinase (MMP) regulation.
Sex-Specific Anatomy
- Women are predisposed to femoral hernia (the obturator foramen is anatomically larger; femoral canal is relatively wider).
- In elderly, cachectic women, loss of the protective fat pad in the obturator foramen specifically predisposes to obturator hernia ("little old lady's hernia").
2. Conditions Causing Chronically Elevated Intra-Abdominal Pressure
These act as a sustained hydraulic force directed at natural abdominal wall weak points:
| Condition | Mechanism |
|---|---|
| Obesity | Persistently raised intra-abdominal pressure; fat infiltration weakens abdominal wall |
| Chronic obstructive pulmonary disease (COPD) | Repeated vigorous coughing causes repeated pressure spikes |
| Chronic constipation | Straining during defecation |
| Benign prostatic hyperplasia (prostatism) | Straining during urination |
| Ascites | Sustained elevated intra-abdominal pressure; particularly predisposes to umbilical hernia |
| Peritoneal dialysis | Repeated fluid infusion raises intra-abdominal pressure; associated with inguinal and umbilical hernias |
| Pregnancy / multiparity | Stretches and weakens the abdominal wall; raises intra-abdominal pressure |
| Heavy lifting / prolonged standing | Occupational and cumulative exposure to lifting and prolonged standing/walking increases risk of indirect inguinal hernia repair, particularly in those with a patent processus vaginalis |
Note on lifting: The role of a single strenuous event is unsettled. A systematic review by Svendsen et al. could not establish a causal relationship between specific mechanical insults and inguinal hernia development. However, cumulative daily lifting exposure in male cohort studies was associated with increased indirect inguinal hernia repair.
3. Connective Tissue and Collagen Disorders
The abdominal wall depends on collagen integrity. Type I collagen provides tensile strength; Type III collagen is thinner, serves as a temporary remodeling scaffold. A decreased type I : type III collagen ratio is detected in fascial and skin specimens from hernia patients.
Inherited Connective Tissue Diseases
- Marfan syndrome — defect in fibrillin-1; systemic connective tissue weakness
- Ehlers-Danlos syndrome — defective collagen cross-linking
- Osteogenesis imperfecta — type I collagen mutation
- Congenital hip dislocation — associated with groin hernia in childhood
Aortic Aneurysm (Thoracic or Abdominal)
Both thoracic and abdominal aortic aneurysms are listed as independent risk factors for inguinal hernia. This reflects a shared systemic collagen/elastin abnormality affecting both the aortic wall and the transversalis fascia, not a mechanical effect.
4. Smoking
Smoking carries a dual mechanism of harm:
- "Metastatic emphysema": Cannon and Read demonstrated that smokers with inguinal hernias have significantly greater circulating serum elastolytic activity, degrading the elastic fibers of the transversalis fascia at a distance from the lungs
- MMP upregulation: Smoking increases expression of matrix metalloproteinases (particularly MMP-1 and MMP-2), which degrade the extracellular collagen matrix
- Impaired wound healing: Tissue hypoxia from nicotine-mediated vasoconstriction increases the risk of incisional hernia after surgery and recurrence after repair
Smoking cessation for at least 4 weeks before hernia repair is advocated by most surgeons to reduce perioperative and healing-related complications.
5. Matrix Metalloproteinase (MMP) Abnormalities
MMPs are 23 structurally related zinc-dependent enzymes with collagenolytic activity. They maintain the extracellular matrix (ECM) in a balance of synthesis and degradation regulated by TIMPs (tissue inhibitors of MMPs).
- MMP overexpression in the transversalis fascia was first demonstrated by Bellon et al. in direct and indirect inguinal hernia patients
- MMP/TIMP imbalance → accelerated ECM degradation → fascial weakness
- Factors that may suppress MMP expression (with therapeutic interest): tetracyclines (especially doxycycline), aspirin, statins, thiazolidinediones
- Additional molecular factors implicated: deficiency of the elastic fiber system, decreased tropoelastin, decreased lysyl oxidase-like 1 synthesis, elastase overexpression, TGF-β1 overexpression
6. Surgical and Iatrogenic Factors (Incisional Hernia)
Incisional hernia is an almost exclusively acquired hernia driven by postoperative wound failure.
| Risk Factor | Details |
|---|---|
| Wound infection | Increases risk from ~20% to 35–50%; the single most powerful postoperative predictor |
| Vertical midline incision | Higher risk than transverse incision; no crossing muscular support |
| Obesity | Most important modifiable patient factor |
| Diabetes mellitus | Impaired collagen synthesis and wound healing |
| Immunosuppression / glucocorticoids | Suppress collagen crosslinking and tissue repair |
| Collagen vascular disease | Intrinsic fascial weakness |
| Smoking | Tissue hypoxia, MMP overexpression |
| COPD / pulmonary complications | Chronic cough + raised postoperative intra-abdominal pressure |
| Advanced age | Progressive collagen atrophy |
| Malnutrition / cachexia | Impaired healing substrate |
| Ascites | Sustained high intra-abdominal pressure on healing fascia |
| Trocar size >10 mm (laparoscopic) | Larger fascial defect not closed → trocar-site hernia |
| Lateral vs. midline trocar | Lateral trocar placement has lower hernia risk |
| Prior hernia repair | Recurrence risk 15–40%; each re-repair carries higher recurrence |
7. Developmental / Embryological Factors
| Factor | Hernia Type |
|---|---|
| Patent processus vaginalis (present in 12–20% of adults) | Indirect inguinal hernia; the patent channel provides a pre-formed peritoneal sac |
| Umbilical ring failure to close | Umbilical hernia in infants |
| Peritoneal mesocolic recess formation after bariatric/colorectal surgery | Internal hernia (Roux-en-Y limb herniation) |
Summary Table — Risk Factors by Category
| Category | Key Risk Factors |
|---|---|
| Demographic | Male sex, age >60, family history |
| Raised IAP | Obesity, COPD, chronic cough, constipation, prostatism, ascites, peritoneal dialysis, multiparity |
| Connective tissue | Marfan, Ehlers-Danlos, osteogenesis imperfecta, aortic aneurysm (TAA/AAA) |
| Biochemical/molecular | MMP/TIMP imbalance, ↓type I:III collagen ratio, elastolytic enzyme excess |
| Modifiable lifestyle | Smoking, obesity, physical inactivity, poor nutrition |
| Surgical | Wound infection, vertical incision, immunosuppression, diabetes, large trocars |
| Developmental | Patent processus vaginalis, umbilical ring failure |
Sources: Mulholland & Greenfield's Surgery, 7e (Table 72.2 and "Why Do Human Beings Develop Abdominal Wall Hernias?"); Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Roberts & Hedges' Clinical Procedures in Emergency Medicine; Current Surgical Therapy, 14e; Sabiston Textbook of Surgery.
This is a shared conversation. Sign in to Orris to start your own chat.