Recurrent pregnancy losss , tell me everything related to neet pg
Reading File
Finding Sources
Finding Sources
Searching PubMed
"recurrent pregnancy loss" management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Searching the Web
recurrent pregnancy loss NEET PG important points high yield 2024 2025
Loading Image
Here is a complete, high-yield NEET PG breakdown of Recurrent Pregnancy Loss (RPL):
Recurrent Pregnancy Loss (RPL) - NEET PG Complete Notes
1. DEFINITION (High Yield - Frequently Asked)
| Authority | Definition |
|---|---|
| Traditional / RCOG | 3 or more consecutive pregnancy losses before 20 weeks |
| ASRM & ESHRE (Current) | 2 or more clinically recognized pregnancy losses |
| ACOG | 2 or more failed clinical pregnancies |
- Incidence: ~1% of women (with 3+ losses); ~5% with 2+ losses
- Sporadic miscarriage rate: 15-25% of all clinically recognized pregnancies
- Sensitivity of investigation warranted after 2 losses - same prevalence of abnormal findings as after 3 losses
- Risk of subsequent loss: 24% after 2 losses, 30% after 3 losses, 40-50% after 4 losses
Even after multiple losses, a patient is more likely to have a successful pregnancy than to miscarry again.
2. ETIOLOGY - The BIG Picture
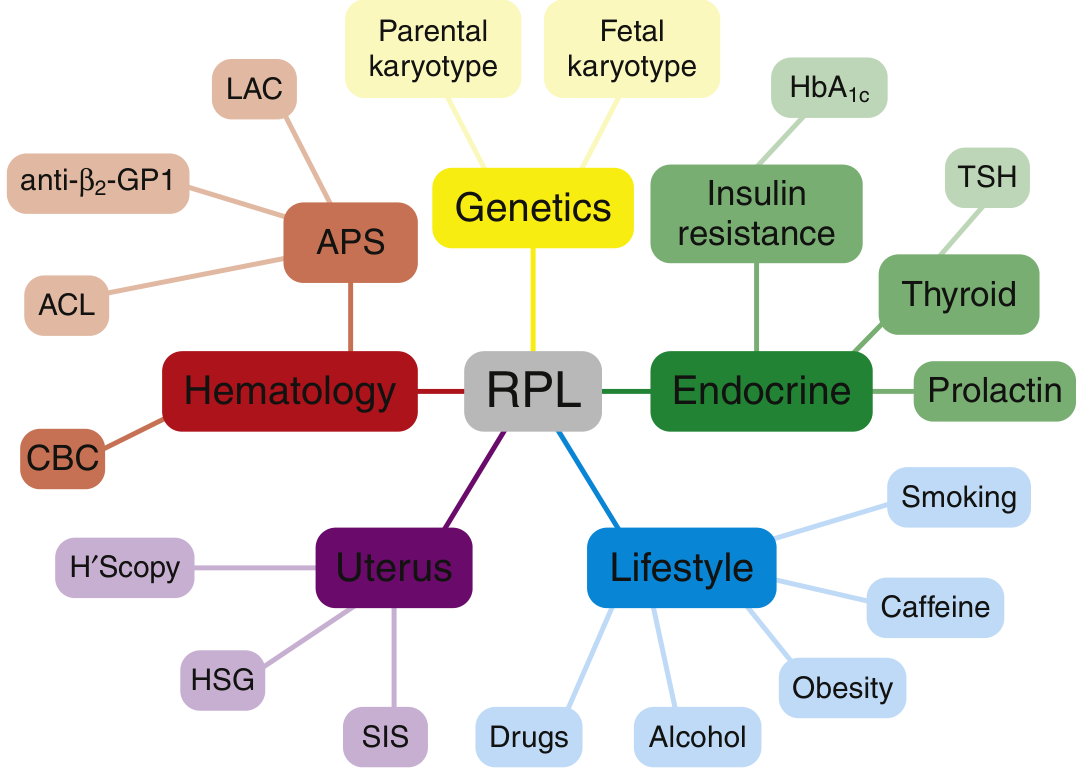
A. GENETIC FACTORS (Most Common Cause of 1st Trimester Loss)
- Fetal aneuploidy = most common cause of first trimester miscarriage overall
- Found in 50-75% of miscarriage tissue samples
- Breakdown: autosomal trisomy (~60-70%) > monosomy X (~10-20%) > polyploidy (~10-20%)
- Parental karyotype abnormalities found in only 2-5% of RPL couples (balanced translocations - Robertsonian or reciprocal)
- ASRM recommends routine parental karyotyping; ESHRE does not
Key NEET point: The most common parental chromosomal abnormality in RPL = balanced translocation
B. ANATOMIC FACTORS
Uterine anomalies account for 10-15% of RPL cases.
| Anomaly | Notes |
|---|---|
| Septate uterus | Most common congenital anomaly associated with RPL; most amenable to surgical correction |
| Bicornuate uterus | Associated more with 2nd trimester losses |
| Arcuate uterus | Debatable clinical significance |
| Asherman syndrome | Intrauterine adhesions |
| Submucosal fibroids | Distort the cavity |
| Cervical incompetence | 2nd trimester losses |
- Investigation: HSG (first line), followed by hysteroscopy (gold standard) or SIS (saline infusion sonography)
- Treatment of septum: Hysteroscopic metroplasty (resection) - dramatically improves outcome
C. ANTIPHOSPHOLIPID SYNDROME (APS) - Most Treatable Cause
The most important acquired cause of RPL. Very high yield for NEET PG.
Sapporo/Sydney Criteria for APS diagnosis:
Clinical criteria (at least 1):
- Vascular thrombosis (arterial, venous, or small vessel)
- Pregnancy morbidity:
- ≥3 unexplained consecutive losses before 10 weeks, OR
- ≥1 unexplained loss of morphologically normal fetus ≥10 weeks, OR
- ≥1 premature birth before 34 weeks due to eclampsia/placental insufficiency
Laboratory criteria (at least 1, confirmed on TWO occasions ≥12 weeks apart):
- Lupus anticoagulant (LAC) - most predictive
- Anticardiolipin antibodies (IgG or IgM) in medium-high titer (>40 GPL/MPL)
- Anti-β2 glycoprotein-1 antibodies (IgG or IgM)
Mechanism: aPL antibodies → bind β2-GP1 on trophoblast → inhibit trophoblast invasion → placental thrombosis and infarction → pregnancy loss
Treatment of APS in pregnancy:
- Without prior thrombosis: Low-molecular-weight heparin (LMWH) prophylactic dose + Low-dose aspirin (LDA) 75-81 mg/day - continue 6-12 weeks postpartum
- With prior thrombosis: Therapeutic-dose heparin + LDA
- Recent addition (conditional recommendation): Hydroxychloroquine 200-400 mg/day in APS pregnancy
- Live birth rates with heparin + aspirin: ~70-80%
NEET pearl: Warfarin is CONTRAINDICATED in pregnancy (causes embryopathy). Use heparin instead.
D. ENDOCRINE FACTORS
| Condition | Association |
|---|---|
| Poorly controlled DM | Increased RPL (HbA1c key marker) |
| Hypothyroidism / Subclinical hypothyroidism | TSH >2.5 mIU/L in 1st trimester associated with RPL |
| Antithyroid antibodies | Increased prevalence in RPL even without overt thyroid disease (rapidly gaining evidence) |
| Hyperprolactinemia | Associated with luteal phase defect; treat with cabergoline/bromocriptine |
| PCOS | Associated with RPL (LH hypersecretion, hyperandrogenism, insulin resistance) |
| Luteal phase defect | Controversial; low progesterone |
- Recommended tests: TSH, HbA1c, prolactin, fasting glucose/insulin
E. THROMBOPHILIAS (Inherited) - Controversial
| Thrombophilia | Notes |
|---|---|
| Factor V Leiden (FVL) | Most common inherited thrombophilia |
| Prothrombin gene mutation (G20210A) | 2nd most common |
| Protein C deficiency | |
| Protein S deficiency | |
| Antithrombin III deficiency | |
| MTHFR mutation (C677T) | Linked to DNA damage in males; hyperhomocysteinemia |
Key NEET point: ACOG, ASRM, and ESHRE all recommend AGAINST routine thrombophilia testing in RPL unless there is a personal/family history of thrombosis. Heparin treatment does NOT improve live birth rate in women with inherited thrombophilia + RPL (Cochrane review).
F. IMMUNOLOGIC FACTORS
- Cellular: NK cell dysfunction, TH1/TH2 cytokine imbalance
- Humoral: APS (covered above)
- TH1/TH2 hypothesis: Shift away from TH2-dominant (pregnancy-protective) to TH1-dominant state
- Chronic endometritis: Plasma cells on endometrial biopsy; prevalence up to 56% in RPL; associated with previous infection/retained tissue
Treatments NOT recommended (no proven benefit):
- IVIG (intravenous immunoglobulin) - RCT showed no benefit
- Leukocyte immunization / paternal cell immunization - NOT recommended
- TNF-α inhibitors (adalimumab, infliximab) - investigational only
- Intralipid infusions - no data support; can cause harm
- Routine corticosteroids - may harm fetus (anomaly rate 4.6% vs 2.6% controls)
G. MALE FACTORS
- Only evidence-based test for male partner = peripheral blood karyotype
- Increased Y chromosome microdeletions in male partners
- Increased sperm chromosomal aneuploidy (sex chromosome disomy)
- Increased sperm DNA fragmentation and lipid peroxidation
- Paternal MTHFR C677T mutation associated with DNA damage and RPL
H. INFECTIOUS CAUSES
- No single organism proven to cause RPL
- Bacterial vaginosis - significant association with 2nd trimester RPL
- HSV, CMV - can directly infect placenta
- Mycoplasma, ureaplasma, Chlamydia - studied but not proven
- Cervical cultures not routinely recommended
I. ENVIRONMENTAL / LIFESTYLE FACTORS
- Smoking, alcohol, caffeine (>200 mg/day), obesity
- Medications: antiprogestogens, antineoplastics, NSAIDs, inhalation anesthetics
- Ionizing radiation, organic solvents
- Endocrine disruptors: phthalates, bisphenol-A, heavy metals
3. INVESTIGATION (Preconception Evaluation)
Recommended/Evidence-Based Tests:
- Parental karyotype (both partners)
- Uterine anatomy: HSG → hysteroscopy/SIS if abnormal
- APS panel: Lupus anticoagulant, aCL antibodies (IgG/IgM), anti-β2-GP1 (IgG/IgM)
- TSH
- Fasting glucose / HbA1c
- Prolactin
- CBC
Tests Under Investigation (Not Routine):
- Antithyroid antibodies (gaining support - may be added soon)
- Ovarian reserve (AMH, Day 3 FSH/E2)
- Endometrial biopsy for chronic endometritis
Tests NOT Recommended:
- Routine thrombophilia panel (FVL, Prothrombin mutation, Protein C/S, AT-III, MTHFR, homocysteine)
- TH1/TH2 cytokine testing
- NK cell testing (peripheral blood or endometrial)
- Parental HLA typing
- Mixed lymphocyte cultures
- Antinuclear antibodies / antipaternal cytotoxic antibodies
NEET Favourite: "At least 50% of RPL couples have no specific etiology identified after complete evaluation" = UNEXPLAINED RPL
4. MANAGEMENT BY CAUSE
| Cause | Treatment |
|---|---|
| Septate uterus | Hysteroscopic metroplasty |
| Asherman syndrome | Hysteroscopic adhesiolysis |
| APS | LMWH + Low-dose aspirin |
| Hypothyroidism | Levothyroxine (keep TSH <2.5 in 1st trimester) |
| Hyperprolactinemia | Cabergoline or bromocriptine |
| PCOS | Metformin (reduces miscarriage risk), weight loss |
| Poorly controlled DM | Glycemic control (HbA1c < 6.5%) |
| Parental translocation | IVF + PGT (preimplantation genetic testing) |
| Progesterone deficiency (luteal phase) | Vaginal micronized progesterone 400 mg BD |
| Unexplained | Psychological support + close monitoring |
Progesterone Supplementation:
- Cochrane 2013: benefit shown in RPL patients
- PROMISE trial (Coomarasamy 2015): 400 mg vaginal micronized progesterone twice daily from positive pregnancy test; no significant difference vs placebo in women with 3+ losses
- PRISM trial (Coomarasamy 2019): benefit found in women with 1-2 previous losses + bleeding in current pregnancy
- Current stance: Consider in women with previous losses, especially those with early pregnancy bleeding
Psychological Support:
- Tender loving care (TLC) - frequent visits, early ultrasounds, reassurance
- Studies show improved live birth rates with supportive care alone in unexplained RPL (up to 70-80% success)
5. PROGNOSIS
| Clinical Scenario | Live Birth Rate in Next Pregnancy |
|---|---|
| 2 previous losses | ~75% |
| 3 previous losses | ~70% |
| 4 previous losses | ~60% |
| 5 previous losses | ~50% |
| Unexplained RPL (any) | 66.7% achieve live birth within 5 years |
| Age <40, <6 losses, supportive care | ~80% |
6. HIGH-YIELD NEET PG ONE-LINERS
- Definition (ASRM/ESHRE): 2 or more pregnancy losses
- Definition (Traditional/RCOG): 3 or more consecutive losses before 20 weeks
- Incidence: <1% of women
- Most common cause of 1st trimester loss overall: Fetal aneuploidy
- Most common fetal chromosomal abnormality in miscarriage: Autosomal trisomy
- Most common parental chromosomal cause of RPL: Balanced translocation (2-5%)
- Most common congenital uterine anomaly in RPL: Septate uterus (treated by hysteroscopic metroplasty)
- Most treatable cause of RPL: APS (treated with heparin + aspirin)
- APS lab criteria must be confirmed: Two occasions ≥12 weeks apart
- Most predictive aPL antibody: Lupus anticoagulant
- Heparin in pregnancy: LMWH preferred; warfarin is CONTRAINDICATED
- Thrombophilia testing: NOT routinely recommended
- IVIG for RPL: No benefit (multiple RCTs and meta-analyses)
- Leukocyte immunization: Not recommended
- 50% of RPL couples: No identifiable etiology
- Gold standard for uterine cavity evaluation: Hysteroscopy
- Male factor investigation: Only peripheral blood karyotype (evidence-based)
- Progesterone trial: Vaginal micronized progesterone 400 mg BD from positive pregnancy test
- Chronic endometritis prevalence in RPL: Up to 56%
- TSH target in 1st trimester: <2.5 mIU/L
7. ANTIPHOSPHOLIPID ANTIBODIES - NEET FOCUS
The 3 antibodies tested in APS:
- Lupus anticoagulant (LAC) - paradoxically causes thrombosis, not bleeding; prolongs aPTT in vitro
- Anticardiolipin antibodies (aCL) - IgG/IgM; cardiolipin is a mitochondrial phospholipid
- Anti-β2 glycoprotein-1 (anti-β2-GP1) - IgG/IgM
DRVVT (Dilute Russell's Viper Venom Time) = preferred test for lupus anticoagulant
False positive VDRL/RPR seen in APS (because cardiolipin is used as antigen in syphilis test)
8. SURGICAL TREATMENTS
| Condition | Procedure |
|---|---|
| Septate uterus | Hysteroscopic metroplasty (resection of septum) |
| Intrauterine adhesions (Asherman) | Hysteroscopic adhesiolysis |
| Submucosal fibroids | Hysteroscopic myomectomy |
| Cervical incompetence | McDonald's suture (cerclage) |
| IVF with PGT | For parental translocation carriers or unexplained RPL |
Recent Evidence (2024-2025 Updates)
- PGT-A in unexplained RPL (Mumusoglu et al., 2025) - Meta-analysis suggests PGT-A may improve live birth rates in unexplained RPL but evidence remains limited [PMID: 39151684]
- APS in pregnancy review (Murvai et al., 2025) - Confirms LMWH + LDA as standard of care; hydroxychloroquine emerging as adjunct [PMID: 40128683]
- Risk prediction models for RPL are being developed but none are in routine clinical use yet [PMID: 40510467]
Sources: Berek & Novak's Gynecology (Chapter 33, pp. 1791-1832); Creasy & Resnik's Maternal-Fetal Medicine (Chapter 41, pp. 977-995)
Create a NEET PG question bank on APS and RPL management
Asking for Preferences
Reading File
Running Command
mkdir -p /home/daytona/workspace/neet-pg-qbank && ls /home/daytona/workspace/nee…
Writing File
~/neet-pg-qbank/generate_qbank.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm, mm
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, KeepTogether, PageBreak
)
from reportlab.lib.enums import TA_LEFT, TA_CENTER, TA_JUSTIFY
from reportlab.pdfgen import canvas
from reportlab.platypus.flowables import Flowable
OUTPUT = "/home/daytona/workspace/neet-pg-qbank/NEET_PG_APS_RPL_QBank.pdf"
# ── Colour palette ──────────────────────────────────────────────────────────
DARK_BLUE = colors.HexColor("#1A3A5C")
MED_BLUE = colors.HexColor("#2E6DA4")
LIGHT_BLUE = colors.HexColor("#D6E8F7")
ACCENT = colors.HexColor("#E8371B") # answer highlight
GOLD = colors.HexColor("#F0A500")
PALE_GREY = colors.HexColor("#F5F5F5")
GREEN = colors.HexColor("#1E7B34")
ANSWER_BG = colors.HexColor("#E8F5E9")
VIGNETTE_BG = colors.HexColor("#FFF8E1")
AR_BG = colors.HexColor("#F3E5F5")
# ── Page number footer ───────────────────────────────────────────────────────
def add_page_number(canvas_obj, doc):
canvas_obj.saveState()
canvas_obj.setFont("Helvetica", 8)
canvas_obj.setFillColor(colors.grey)
page_num = canvas_obj.getPageNumber()
canvas_obj.drawCentredString(A4[0] / 2, 1.2 * cm,
f"NEET PG Question Bank • APS & RPL Management • Page {page_num}")
canvas_obj.setStrokeColor(MED_BLUE)
canvas_obj.setLineWidth(0.5)
canvas_obj.line(2*cm, 1.5*cm, A4[0]-2*cm, 1.5*cm)
canvas_obj.restoreState()
# ── Styles ───────────────────────────────────────────────────────────────────
styles = getSampleStyleSheet()
title_style = ParagraphStyle("Title", fontName="Helvetica-Bold", fontSize=22,
textColor=colors.white, alignment=TA_CENTER,
spaceAfter=4, leading=28)
subtitle_style = ParagraphStyle("Subtitle", fontName="Helvetica", fontSize=11,
textColor=colors.white, alignment=TA_CENTER,
spaceAfter=4)
section_style = ParagraphStyle("Section", fontName="Helvetica-Bold", fontSize=13,
textColor=colors.white, alignment=TA_LEFT,
spaceAfter=2, leading=18)
q_num_style = ParagraphStyle("QNum", fontName="Helvetica-Bold", fontSize=11,
textColor=DARK_BLUE, spaceBefore=6, spaceAfter=2)
q_text_style = ParagraphStyle("QText", fontName="Helvetica", fontSize=10.5,
textColor=colors.black, spaceAfter=6,
leading=16, alignment=TA_JUSTIFY)
option_style = ParagraphStyle("Option", fontName="Helvetica", fontSize=10,
textColor=colors.HexColor("#333333"), spaceAfter=3,
leftIndent=16, leading=14)
answer_style = ParagraphStyle("Answer", fontName="Helvetica-Bold", fontSize=10,
textColor=GREEN, spaceAfter=2, leading=14)
explanation_style = ParagraphStyle("Explanation", fontName="Helvetica", fontSize=9.5,
textColor=colors.HexColor("#444444"), spaceAfter=4,
leading=14, alignment=TA_JUSTIFY)
bold_exp = ParagraphStyle("BoldExp", fontName="Helvetica-Bold", fontSize=9.5,
textColor=DARK_BLUE, spaceAfter=1, leading=14)
vignette_style = ParagraphStyle("Vignette", fontName="Helvetica-Oblique", fontSize=10,
textColor=colors.HexColor("#4A2F00"),
backColor=VIGNETTE_BG,
borderPad=6, spaceAfter=6, leading=15,
alignment=TA_JUSTIFY)
ar_label = ParagraphStyle("ARLabel", fontName="Helvetica-Bold", fontSize=9,
textColor=colors.HexColor("#6A1B9A"), spaceAfter=2)
tag_style = ParagraphStyle("Tag", fontName="Helvetica-Oblique", fontSize=8,
textColor=colors.grey, spaceAfter=4)
# ── Question data ─────────────────────────────────────────────────────────────
# Format: (type, number, tag, stem/vignette, options_or_None, answer, explanation)
# type: "SBA" | "VIGNETTE" | "AR"
# For AR: stem = (assertion_text, reason_text), options = AR_OPTIONS
AR_OPTIONS = [
"A. Both A and R are true, and R is the correct explanation of A",
"B. Both A and R are true, but R is NOT the correct explanation of A",
"C. A is true but R is false",
"D. A is false but R is true",
"E. Both A and R are false",
]
questions = [
# ─── SECTION 1: SBA ───────────────────────────────────────────────────────────
("SBA", 1,
"SECTION A: Single Best Answer (SBA)",
"Which of the following is the MOST COMMON cause of first trimester recurrent pregnancy loss?",
["A. Uterine anomalies",
"B. Antiphospholipid syndrome",
"C. Fetal aneuploidy",
"D. Cervical incompetence",
"E. Hyperprolactinemia"],
"C. Fetal aneuploidy",
"Fetal aneuploidy accounts for 50-75% of all miscarriage tissue. The most common aneuploidy is autosomal trisomy (~60-70%), followed by monosomy X (~10-20%). This is the single largest known cause of first trimester pregnancy loss."),
("SBA", 2,
None,
"A 30-year-old woman has had 3 consecutive first-trimester miscarriages. APS evaluation is positive. The lupus anticoagulant test was positive on two occasions 10 weeks apart. Does this satisfy the laboratory criteria for APS?",
["A. Yes - two positive tests are sufficient regardless of interval",
"B. No - the confirmatory test must be at least 12 weeks after the first",
"C. No - the test must be repeated 6 months later",
"D. Yes - lupus anticoagulant alone is sufficient even with single test",
"E. No - only anticardiolipin antibodies count for APS diagnosis in RPL"],
"B. No - the confirmatory test must be at least 12 weeks after the first",
"Sapporo/Sydney criteria require positive aPL antibodies on TWO occasions at least 12 WEEKS apart. A 10-week interval does NOT satisfy criteria. This prevents false positives from transient antibody positivity (e.g., after infection)."),
("SBA", 3,
None,
"A woman with APS and recurrent pregnancy loss (no prior thrombosis) becomes pregnant. What is the recommended treatment?",
["A. Warfarin + Low-dose aspirin",
"B. Low-molecular-weight heparin (LMWH) + Low-dose aspirin (LDA)",
"C. Unfractionated heparin alone",
"D. Low-dose aspirin alone",
"E. Prednisolone + aspirin"],
"B. Low-molecular-weight heparin (LMWH) + Low-dose aspirin (LDA)",
"For APS without prior thrombosis, the standard of care is prophylactic-dose LMWH + LDA (75-81 mg/day). Warfarin is CONTRAINDICATED in pregnancy (causes warfarin embryopathy: nasal hypoplasia, stippled epiphyses). Aspirin alone is insufficient. Prednisolone has shown harm (increased anomaly rates)."),
("SBA", 4,
None,
"Which of the following antiphospholipid antibodies is considered the MOST PREDICTIVE for adverse pregnancy outcome?",
["A. Anti-β2 glycoprotein-1 IgM",
"B. Anticardiolipin IgG",
"C. Lupus anticoagulant",
"D. Anti-β2 glycoprotein-1 IgG",
"E. Anticardiolipin IgM"],
"C. Lupus anticoagulant",
"The lupus anticoagulant (LAC) is the most predictive aPL antibody for both thrombosis and adverse pregnancy outcomes. Despite its name, it causes thrombosis (not bleeding) in vivo, by binding phospholipid-binding proteins and activating the coagulation cascade."),
("SBA", 5,
None,
"Which thrombophilia testing is RECOMMENDED by ACOG/ASRM in all women with recurrent pregnancy loss?",
["A. Factor V Leiden mutation",
"B. Prothrombin gene mutation G20210A",
"C. Protein C and S levels",
"D. MTHFR mutation",
"E. None of the above - routine thrombophilia screening is NOT recommended"],
"E. None of the above - routine thrombophilia screening is NOT recommended",
"ACOG, ASRM, and ESHRE all recommend AGAINST routine inherited thrombophilia testing in women with RPL. Evidence shows testing and treatment with heparin does NOT improve live birth rates in women with inherited thrombophilias. Testing is reserved for women with personal/family history of thrombosis."),
("SBA", 6,
None,
"A 28-year-old G3P0+3 (all first trimester losses) has a positive VDRL test. She denies sexual risk factors. Which condition should be suspected?",
["A. Syphilis",
"B. Antiphospholipid syndrome",
"C. Systemic lupus erythematosus",
"D. HIV infection",
"E. Hepatitis C"],
"B. Antiphospholipid syndrome",
"APS causes a BIOLOGIC FALSE POSITIVE VDRL/RPR because cardiolipin is used as the antigen in the non-treponemal syphilis test. Anticardiolipin antibodies in APS cross-react with this test. Confirm with FTA-ABS (treponemal test), which will be negative in APS. This is a classic NEET PG trap question."),
("SBA", 7,
None,
"What is the minimum number of pregnancy losses before 10 weeks required to satisfy the PREGNANCY MORBIDITY clinical criterion for APS?",
["A. 1 unexplained loss",
"B. 2 unexplained losses",
"C. 3 or more unexplained consecutive losses",
"D. 2 or more non-consecutive losses",
"E. Any number with positive aPL antibodies"],
"C. 3 or more unexplained consecutive losses",
"Per Sapporo/Sydney criteria: For losses BEFORE 10 weeks, the threshold is 3 OR MORE consecutive unexplained losses. For losses AT OR AFTER 10 weeks (morphologically normal fetus), even a SINGLE unexplained loss qualifies. This distinction is frequently tested."),
("SBA", 8,
None,
"Which of the following uterine anomalies is MOST COMMONLY associated with recurrent pregnancy loss AND is most amenable to surgical correction?",
["A. Bicornuate uterus",
"B. Unicornuate uterus",
"C. Septate uterus",
"D. Didelphic uterus",
"E. Arcuate uterus"],
"C. Septate uterus",
"Septate uterus is the most common congenital uterine anomaly causing RPL. The avascular fibromuscular septum impairs implantation and placentation. Treatment: Hysteroscopic metroplasty (resection of septum), which significantly improves live birth rates. Note: Bicornuate uterus is more associated with 2nd trimester losses."),
("SBA", 9,
None,
"IVIG (Intravenous Immunoglobulin) has been tried for unexplained RPL. What does current evidence show?",
["A. Significant improvement in live birth rates in primary RPL",
"B. Benefit only in secondary RPL (after at least one live birth)",
"C. No benefit - RCTs show no difference vs placebo",
"D. Benefit when combined with prednisolone",
"E. Benefit only if NK cells are elevated"],
"C. No benefit - RCTs show no difference vs placebo",
"A multicenter double-blind RCT and subsequent meta-analysis found NO difference in live birth rates between IVIG and placebo in idiopathic secondary RPL. ASRM and ESHRE do NOT recommend IVIG for RPL. It should only be given in approved research protocols."),
("SBA", 10,
None,
"According to the ASRM and ESHRE current definition, recurrent pregnancy loss is defined as:",
["A. 3 or more consecutive losses before 20 weeks",
"B. 2 or more losses before 20 weeks (consecutive or non-consecutive)",
"C. 3 or more losses before 12 weeks",
"D. 2 or more losses after fetal cardiac activity seen",
"E. 3 or more losses before 28 weeks"],
"B. 2 or more losses before 20 weeks (consecutive or non-consecutive)",
"ASRM and ESHRE currently define RPL as 2 OR MORE clinically recognized pregnancy losses (ultrasound or histopathologic confirmation). The traditional RCOG definition required 3 or more consecutive losses. The updated definition does not require them to be consecutive and applies before 20 weeks."),
# ─── SECTION 2: CLINICAL VIGNETTES ───────────────────────────────────────────
("VIGNETTE", 11,
"SECTION B: Clinical Vignettes",
"A 32-year-old woman presents with her 4th consecutive first trimester miscarriage. Workup reveals: ANA positive (low titer), TSH 3.8 mIU/L, Lupus anticoagulant positive, anticardiolipin IgG 55 GPL (high titer), anti-β2-GP1 negative. The first positive test was 8 weeks ago. Her husband's karyotype is normal. Pelvic MRI shows a normal uterine cavity. What is the MOST APPROPRIATE next step in management?",
["A. Start LMWH + aspirin immediately",
"B. Repeat the aPL antibodies in 4 weeks",
"C. Repeat the aPL antibodies in at least 4 more weeks (total 12 weeks from first test)",
"D. Diagnose APS and start warfarin",
"E. Prescribe prednisolone and aspirin"],
"C. Repeat the aPL antibodies in at least 4 more weeks (total 12 weeks from first test)",
"APS diagnosis requires confirmation at least 12 WEEKS after the first positive test. Only 8 weeks have elapsed, so criteria are not yet met. The aPL test must be repeated after the 12-week interval. Starting treatment before confirmed diagnosis could expose the patient to unnecessary anticoagulation risk. Warfarin is absolutely contraindicated in pregnancy."),
("VIGNETTE", 12,
None,
"A 27-year-old G2P0+2 is referred for RPL evaluation. Both pregnancies were lost at 8 weeks. Laboratory results: Lupus anticoagulant - positive; Anticardiolipin IgG - 52 GPL; Anti-β2-GP1 IgG - positive. Tests were confirmed 14 weeks later - all remain positive. She is now trying to conceive. She has no history of thrombosis. What is the recommended treatment once pregnancy is confirmed?",
["A. Warfarin 5 mg daily",
"B. Aspirin 75 mg daily alone",
"C. Unfractionated heparin 5000 units TDS subcutaneously",
"D. Prophylactic LMWH (e.g., enoxaparin 40 mg/day) + aspirin 75 mg/day",
"E. Hydroxychloroquine alone"],
"D. Prophylactic LMWH (e.g., enoxaparin 40 mg/day) + aspirin 75 mg/day",
"This patient has definite APS (meets all Sydney criteria). Without prior thrombosis, she receives PROPHYLACTIC dose LMWH + LDA during pregnancy, continuing 6-12 weeks postpartum. This woman is also 'triple positive' (LAC + aCL + anti-β2GP1) which confers the highest obstetric risk and strictest management. Warfarin is teratogenic. Aspirin alone is insufficient."),
("VIGNETTE", 13,
None,
"A 35-year-old woman is investigated for RPL (3 losses). Her APS panel is negative twice. Parental karyotype: normal. HSG: normal cavity. TSH: 3.0. HbA1c: 5.4%. She has irregular cycles and elevated LH on day 3. Ultrasound shows polycystic ovaries. What is the MOST LIKELY contributing diagnosis and its mechanism of loss?",
["A. Premature ovarian insufficiency - low estrogen",
"B. PCOS - LH hypersecretion leads to premature oocyte maturation and luteal defect",
"C. Hypothyroidism - low T4 causes luteal phase defect",
"D. Diabetes mellitus - hyperglycemia causes embryo toxicity",
"E. Prolactinoma - high prolactin suppresses progesterone"],
"B. PCOS - LH hypersecretion leads to premature oocyte maturation and luteal defect",
"PCOS is associated with RPL through multiple mechanisms: (1) LH hypersecretion causes premature oocyte maturation and poor embryo quality; (2) hyperinsulinemia/insulin resistance; (3) hyperandrogenism affecting endometrial receptivity. This patient has classic PCOS features: irregular cycles, elevated LH, PCO morphology. Management includes metformin (reduces miscarriage risk) and weight loss."),
("VIGNETTE", 14,
None,
"A 29-year-old woman with 3 unexplained losses presents with positive pregnancy test at 5 weeks. She is desperate to continue the pregnancy. Her GP asks whether progesterone supplementation should be started. What does CURRENT evidence suggest?",
["A. Proven benefit - start 400 mg vaginal progesterone twice daily immediately",
"B. No proven benefit in women with RPL and no current bleeding (PROMISE trial)",
"C. Proven benefit only if given from conception",
"D. Progesterone is contraindicated in the first trimester",
"E. Benefit proven in all RPL patients regardless of bleeding status"],
"B. No proven benefit in women with RPL and no current bleeding (PROMISE trial)",
"The PROMISE RCT (Coomarasamy, 2015) randomized women with 3+ prior losses to 400 mg vaginal micronized progesterone twice daily vs placebo from positive pregnancy test. Result: NO significant difference in live birth rates. The PRISM trial (2019) showed benefit specifically in women with 1-2 previous losses WHO ALSO HAD BLEEDING in the current pregnancy. Current recommendation: progesterone is NOT routinely prescribed for RPL without bleeding."),
("VIGNETTE", 15,
None,
"A woman with confirmed APS (LAC positive, prior DVT) is now 8 weeks pregnant with her 4th pregnancy (3 previous losses at 9-11 weeks). What anticoagulation regimen is appropriate?",
["A. Prophylactic LMWH + aspirin",
"B. Therapeutic-dose LMWH + aspirin",
"C. Aspirin alone (prior DVT was treated)",
"D. Warfarin + aspirin throughout pregnancy",
"E. Unfractionated heparin prophylaxis only"],
"B. Therapeutic-dose LMWH + aspirin",
"For APS patients WITH A HISTORY OF THROMBOSIS, therapeutic-dose (not prophylactic) LMWH + LDA is recommended throughout pregnancy and for 6-12 weeks postpartum. The prior DVT elevates her thrombotic risk category. Warfarin is contraindicated in pregnancy. This distinction (prophylactic vs therapeutic dosing based on thrombosis history) is a key NEET PG differentiator."),
# ─── SECTION 3: ASSERTION-REASON ─────────────────────────────────────────────
("AR", 16,
"SECTION C: Assertion-Reason",
("Assertion (A): Warfarin is contraindicated in pregnancy for management of APS.",
"Reason (R): Warfarin crosses the placenta and can cause warfarin embryopathy."),
AR_OPTIONS,
"A. Both A and R are true, and R is the correct explanation of A",
"Warfarin crosses the placenta and is teratogenic during weeks 6-12 (organogenesis), causing warfarin embryopathy: nasal hypoplasia, stippled epiphyses (chondrodysplasia punctata), and CNS/eye abnormalities. LMWH is the safe alternative as it does NOT cross the placenta."),
("AR", 17,
None,
("Assertion (A): Lupus anticoagulant prolongs the APTT in vitro but causes thrombosis in vivo.",
"Reason (R): LAC inhibits phospholipid-dependent coagulation reactions in the test tube, but in vivo it activates platelets and endothelium via β2-glycoprotein-1."),
AR_OPTIONS,
"A. Both A and R are true, and R is the correct explanation of A",
"The paradox of LAC: It inhibits phospholipid-dependent coagulation IN VITRO (prolonged aPTT, DRVVT), but IN VIVO it binds β2-GP1 on cell surfaces, activating platelets, monocytes and endothelial cells - causing a prothrombotic state. This explains why 'anticoagulant' in the name is misleading for clinical management."),
("AR", 18,
None,
("Assertion (A): Approximately 50% of couples evaluated for RPL have no identifiable etiology.",
"Reason (R): This is because current investigations do not test for all possible causes, and some causes remain scientifically uncharacterized."),
AR_OPTIONS,
"A. Both A and R are true, and R is the correct explanation of A",
"Despite complete evaluation (genetic, anatomic, endocrine, immunologic, thrombophilic workup), at least 50% of RPL couples have no single dominant etiology identified. The reason includes both limitations of current testing and genuinely unknown mechanisms. These couples receive the diagnosis of 'unexplained RPL' and are managed with supportive care."),
("AR", 19,
None,
("Assertion (A): Routine thrombophilia screening (Factor V Leiden, Prothrombin mutation) is recommended in all women with RPL.",
"Reason (R): Inherited thrombophilias cause placental thrombosis and treatment with heparin significantly improves live birth rates."),
AR_OPTIONS,
"E. Both A and R are false",
"Both the assertion and reason are FALSE. ACOG, ASRM, and ESHRE all RECOMMEND AGAINST routine thrombophilia screening in RPL. Furthermore, meta-analyses (Cochrane review) confirm that heparin treatment does NOT significantly improve live birth rates in women with inherited thrombophilia + RPL without APS. Screening is reserved for personal/family history of thrombosis."),
("AR", 20,
None,
("Assertion (A): A false positive VDRL test in a woman with RPL may indicate APS rather than syphilis.",
"Reason (R): Cardiolipin is the antigen used in non-treponemal tests for syphilis, and anticardiolipin antibodies in APS cross-react with this test."),
AR_OPTIONS,
"A. Both A and R are true, and R is the correct explanation of A",
"Classic NEET PG question. Non-treponemal tests (VDRL, RPR) use cardiolipin-lecithin-cholesterol antigen. aCL antibodies in APS bind cardiolipin and cause false positivity. Confirm with treponemal test (FTA-ABS, TPHA) - this will be NEGATIVE in APS. Always think APS in a woman with RPL + false positive VDRL."),
]
# ─── PDF BUILD ───────────────────────────────────────────────────────────────
def build_pdf():
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
topMargin=2.5*cm, bottomMargin=2.2*cm,
leftMargin=2*cm, rightMargin=2*cm,
title="NEET PG Question Bank: APS & RPL Management",
author="Orris Medical AI"
)
story = []
# ── Cover Banner ──────────────────────────────────────────────────────────
cover_data = [[
Paragraph("NEET PG QUESTION BANK", title_style),
]]
cover_table = Table(cover_data, colWidths=[17*cm])
cover_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), DARK_BLUE),
("ROUNDEDCORNERS", [8]),
("TOPPADDING", (0,0), (-1,-1), 18),
("BOTTOMPADDING", (0,0), (-1,-1), 6),
("LEFTPADDING", (0,0), (-1,-1), 16),
("RIGHTPADDING", (0,0), (-1,-1), 16),
]))
story.append(cover_table)
story.append(Spacer(1, 0.3*cm))
sub_data = [[
Paragraph("Antiphospholipid Syndrome (APS) & Recurrent Pregnancy Loss (RPL) Management", subtitle_style),
]]
sub_table = Table(sub_data, colWidths=[17*cm])
sub_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), MED_BLUE),
("ROUNDEDCORNERS", [6]),
("TOPPADDING", (0,0), (-1,-1), 10),
("BOTTOMPADDING", (0,0), (-1,-1), 10),
("LEFTPADDING", (0,0), (-1,-1), 16),
("RIGHTPADDING", (0,0), (-1,-1), 16),
]))
story.append(sub_table)
story.append(Spacer(1, 0.4*cm))
# Stats bar
stats_data = [["20 Questions", "3 Types", "OB/GYN | Immunology", "July 2026"]]
stats_table = Table(stats_data, colWidths=[4.25*cm]*4)
stats_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), LIGHT_BLUE),
("FONTNAME", (0,0), (-1,-1), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,-1), 9),
("TEXTCOLOR", (0,0), (-1,-1), DARK_BLUE),
("ALIGN", (0,0), (-1,-1), "CENTER"),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("TOPPADDING", (0,0), (-1,-1), 8),
("BOTTOMPADDING", (0,0), (-1,-1), 8),
("GRID", (0,0), (-1,-1), 0.5, MED_BLUE),
("ROUNDEDCORNERS", [4]),
]))
story.append(stats_table)
story.append(Spacer(1, 0.5*cm))
# Legend
legend_data = [
[
Paragraph("<b>Question Types:</b>", ParagraphStyle("l", fontName="Helvetica-Bold", fontSize=9, textColor=DARK_BLUE)),
Paragraph("■ SBA = Single Best Answer", ParagraphStyle("l2", fontName="Helvetica", fontSize=9, textColor=colors.black)),
Paragraph("■ Clinical Vignette = Case-based SBA", ParagraphStyle("l2", fontName="Helvetica", fontSize=9, textColor=colors.black)),
Paragraph("■ A/R = Assertion-Reason", ParagraphStyle("l2", fontName="Helvetica", fontSize=9, textColor=colors.black)),
]
]
legend_table = Table(legend_data, colWidths=[3.5*cm, 4*cm, 5*cm, 4.5*cm])
legend_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), PALE_GREY),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING", (0,0), (-1,-1), 6),
("LEFTPADDING", (0,0), (-1,-1), 8),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
]))
story.append(legend_table)
story.append(Spacer(1, 0.8*cm))
story.append(HRFlowable(width="100%", thickness=1.5, color=MED_BLUE))
story.append(Spacer(1, 0.5*cm))
current_section = None
for idx, q in enumerate(questions):
qtype, qnum, section_label, stem, options, answer, explanation = q
items = []
# Section header
if section_label and section_label != current_section:
current_section = section_label
# Determine background color
if "A:" in section_label:
bg = MED_BLUE
elif "B:" in section_label:
bg = colors.HexColor("#B85C00")
else:
bg = colors.HexColor("#6A1B9A")
sec_data = [[Paragraph(section_label, section_style)]]
sec_table = Table(sec_data, colWidths=[17*cm])
sec_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), bg),
("TOPPADDING", (0,0), (-1,-1), 10),
("BOTTOMPADDING", (0,0), (-1,-1), 10),
("LEFTPADDING", (0,0), (-1,-1), 12),
("ROUNDEDCORNERS", [6]),
]))
items.append(sec_table)
items.append(Spacer(1, 0.4*cm))
# Question number + type badge
type_colors = {"SBA": MED_BLUE, "VIGNETTE": colors.HexColor("#B85C00"), "AR": colors.HexColor("#6A1B9A")}
badge_color = type_colors.get(qtype, MED_BLUE)
badge_data = [[
Paragraph(f"<b>Q{qnum}.</b>", q_num_style),
Paragraph(f"<b>{qtype}</b>", ParagraphStyle("Badge", fontName="Helvetica-Bold",
fontSize=8, textColor=colors.white, alignment=TA_CENTER)),
]]
badge_table = Table(badge_data, colWidths=[15.2*cm, 1.8*cm])
badge_table.setStyle(TableStyle([
("BACKGROUND", (1,0), (1,0), badge_color),
("ALIGN", (1,0), (1,0), "CENTER"),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("TOPPADDING", (1,0), (1,0), 4),
("BOTTOMPADDING", (1,0), (1,0), 4),
("ROUNDEDCORNERS", [4]),
]))
items.append(badge_table)
# Stem / Vignette
if qtype == "VIGNETTE":
items.append(Paragraph(stem, vignette_style))
elif qtype == "AR":
assertion_text, reason_text = stem
ar_bg_data = [[
Paragraph(f"<b>Assertion (A):</b> {assertion_text.replace('Assertion (A): ', '')}", q_text_style),
]]
ar_bg_table = Table(ar_bg_data, colWidths=[17*cm])
ar_bg_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), VIGNETTE_BG),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 10),
]))
items.append(ar_bg_table)
ar_r_data = [[
Paragraph(f"<b>Reason (R):</b> {reason_text.replace('Reason (R): ', '')}", q_text_style),
]]
ar_r_table = Table(ar_r_data, colWidths=[17*cm])
ar_r_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), AR_BG),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING", (0,0), (-1,-1), 6),
("LEFTPADDING", (0,0), (-1,-1), 10),
]))
items.append(ar_r_table)
items.append(Spacer(1, 0.2*cm))
else:
items.append(Paragraph(stem, q_text_style))
# Options
if options:
for opt in options:
is_answer = opt.startswith(answer[:2])
opt_style = ParagraphStyle(
"OptHL" if is_answer else "Opt",
fontName="Helvetica-Bold" if is_answer else "Helvetica",
fontSize=10,
textColor=GREEN if is_answer else colors.HexColor("#333333"),
leftIndent=16, spaceAfter=3, leading=14,
)
items.append(Paragraph(opt, opt_style))
items.append(Spacer(1, 0.25*cm))
# Answer box
ans_data = [[
Paragraph(f"✓ Correct Answer: {answer}", ParagraphStyle(
"AnsBox", fontName="Helvetica-Bold", fontSize=10,
textColor=GREEN)),
]]
ans_table = Table(ans_data, colWidths=[17*cm])
ans_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), ANSWER_BG),
("TOPPADDING", (0,0), (-1,-1), 7),
("BOTTOMPADDING", (0,0), (-1,-1), 7),
("LEFTPADDING", (0,0), (-1,-1), 12),
("LINEABOVE", (0,0), (-1,0), 1.5, GREEN),
("LINEBELOW", (0,-1), (-1,-1), 1.5, GREEN),
]))
items.append(ans_table)
items.append(Spacer(1, 0.15*cm))
# Explanation box
exp_data = [[
Paragraph(f"<b>Explanation:</b> {explanation}", explanation_style),
]]
exp_table = Table(exp_data, colWidths=[17*cm])
exp_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), PALE_GREY),
("TOPPADDING", (0,0), (-1,-1), 8),
("BOTTOMPADDING", (0,0), (-1,-1), 8),
("LEFTPADDING", (0,0), (-1,-1), 12),
("RIGHTPADDING", (0,0), (-1,-1), 12),
("LINEBEFORE", (0,0), (0,-1), 3, MED_BLUE),
]))
items.append(exp_table)
items.append(Spacer(1, 0.6*cm))
story.append(KeepTogether(items))
# ── Back matter: Quick Reference Table ────────────────────────────────────
story.append(PageBreak())
story.append(Paragraph("QUICK REFERENCE: APS & RPL Cheat Sheet", ParagraphStyle(
"CheatTitle", fontName="Helvetica-Bold", fontSize=14, textColor=DARK_BLUE,
spaceAfter=12, alignment=TA_CENTER)))
cheat_data = [
["Topic", "Key Fact"],
["RPL Definition (ASRM/ESHRE)", "2 or more pregnancy losses"],
["RPL Definition (Traditional/RCOG)", "3 or more consecutive losses before 20 weeks"],
["Most common cause of 1st trimester loss", "Fetal aneuploidy (50-75% of samples)"],
["Most common aneuploidy in miscarriage", "Autosomal trisomy (~60-70%)"],
["APS lab confirmation interval", "Two tests at least 12 weeks apart"],
["Most predictive aPL antibody", "Lupus anticoagulant (LAC)"],
["APS treatment (no prior thrombosis)", "Prophylactic LMWH + Low-dose aspirin"],
["APS treatment (with prior thrombosis)", "Therapeutic LMWH + Low-dose aspirin"],
["Warfarin in pregnancy", "CONTRAINDICATED (embryopathy)"],
["False positive VDRL", "Think APS (anticardiolipin antibodies)"],
["IVIG for RPL", "No benefit - not recommended"],
["Leukocyte immunization for RPL", "Not recommended"],
["Thrombophilia screening in RPL", "NOT routinely recommended"],
["Most treatable cause of RPL", "Antiphospholipid Syndrome (APS)"],
["Best surgical option for septate uterus", "Hysteroscopic metroplasty"],
["Unexplained RPL prevalence", "At least 50% of RPL couples"],
["PROMISE trial (progesterone)", "No benefit in RPL without bleeding"],
["PRISM trial (progesterone)", "Benefit in 1-2 losses WITH bleeding"],
["Hydroxychloroquine in APS", "Conditionally recommended (new addition)"],
["TSH target in 1st trimester", "< 2.5 mIU/L"],
]
cheat_table = Table(cheat_data, colWidths=[8.5*cm, 8.5*cm])
cheat_style = TableStyle([
("BACKGROUND", (0,0), (-1,0), DARK_BLUE),
("TEXTCOLOR", (0,0), (-1,0), colors.white),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,-1), 9),
("FONTNAME", (0,1), (0,-1), "Helvetica-Bold"),
("TEXTCOLOR", (0,1), (0,-1), DARK_BLUE),
("ALIGN", (0,0), (-1,-1), "LEFT"),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING", (0,0), (-1,-1), 6),
("LEFTPADDING", (0,0), (-1,-1), 8),
("ROWBACKGROUNDS", (0,1), (-1,-1), [colors.white, LIGHT_BLUE]),
("GRID", (0,0), (-1,-1), 0.5, colors.HexColor("#AAAAAA")),
("LINEBELOW", (0,0), (-1,0), 2, MED_BLUE),
])
cheat_table.setStyle(cheat_style)
story.append(cheat_table)
doc.build(story, onFirstPage=add_page_number, onLaterPages=add_page_number)
print(f"PDF created: {OUTPUT}")
build_pdf()
Running Command
cd /home/daytona/workspace/neet-pg-qbank && python generate_qbank.py 2>&1
Running Command
ls -lh /home/daytona/workspace/neet-pg-qbank/NEET_PG_APS_RPL_QBank.pdf
Your NEET PG Question Bank is ready:
NEET PG APS RPL QBank
PDF Document · PDF
Here's what's inside the PDF:
Section A - Single Best Answer (Q1-10)
| Q | Topic |
|---|---|
| 1 | Most common cause of 1st trimester RPL |
| 2 | APS lab criteria - 12-week interval trap |
| 3 | APS treatment in pregnancy (no prior thrombosis) |
| 4 | Most predictive aPL antibody |
| 5 | Thrombophilia screening in RPL |
| 6 | False positive VDRL in RPL (APS trap) |
| 7 | APS criteria - losses before vs after 10 weeks |
| 8 | Uterine anomaly most associated with RPL |
| 9 | IVIG evidence for RPL |
| 10 | RPL definition - ASRM vs RCOG |
Section B - Clinical Vignettes (Q11-15)
| Q | Scenario |
|---|---|
| 11 | APS workup - confirmatory test timing dilemma |
| 12 | Triple-positive APS - treatment choice |
| 13 | PCOS with RPL - mechanism |
| 14 | Progesterone in RPL - PROMISE vs PRISM trial evidence |
| 15 | APS with prior DVT - therapeutic vs prophylactic dose |
Section C - Assertion-Reason (Q16-20)
| Q | Topic |
|---|---|
| 16 | Warfarin contraindication in pregnancy |
| 17 | Lupus anticoagulant paradox (prolongs APTT but causes thrombosis) |
| 18 | 50% unexplained RPL |
| 19 | Thrombophilia screening - both A and R false |
| 20 | False positive VDRL and aCL cross-reactivity |
The PDF also includes a Quick Reference Cheat Sheet with 21 one-liner facts at the end - perfect for last-minute revision.
This is a shared conversation. Sign in to Orris to start your own chat.