erythropoiesis
Reading File
Finding Sources
Searching PubMed
erythropoiesis regulation
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Here it is:
Erythropoiesis
Erythropoiesis is the process by which the body produces red blood cells (erythrocytes) to maintain adequate oxygen delivery to peripheral tissues. It occurs primarily in the red bone marrow and is tightly regulated by a negative-feedback loop centered on the hormone erythropoietin (EPO).
1. Overview and Regulation
The delivery of oxygen to tissues is the driving force behind erythropoiesis. Under normal conditions, approximately 1% of circulating erythrocytes is replaced daily - roughly 2.5 to 3.0 million cells per second, or ~250 billion per day. This is balanced against the destruction of senescent cells.
The central regulator is EPO, a 30.4 kDa glycoprotein hormone produced by peritubular interstitial fibroblasts in the renal cortex. When tissue oxygenation falls (due to anemia, hemorrhage, or hypoxia), these cells increase EPO output. EPO then acts on specific EPO receptors (EPO-Rs) on bone marrow erythroid progenitors to stimulate red cell production.
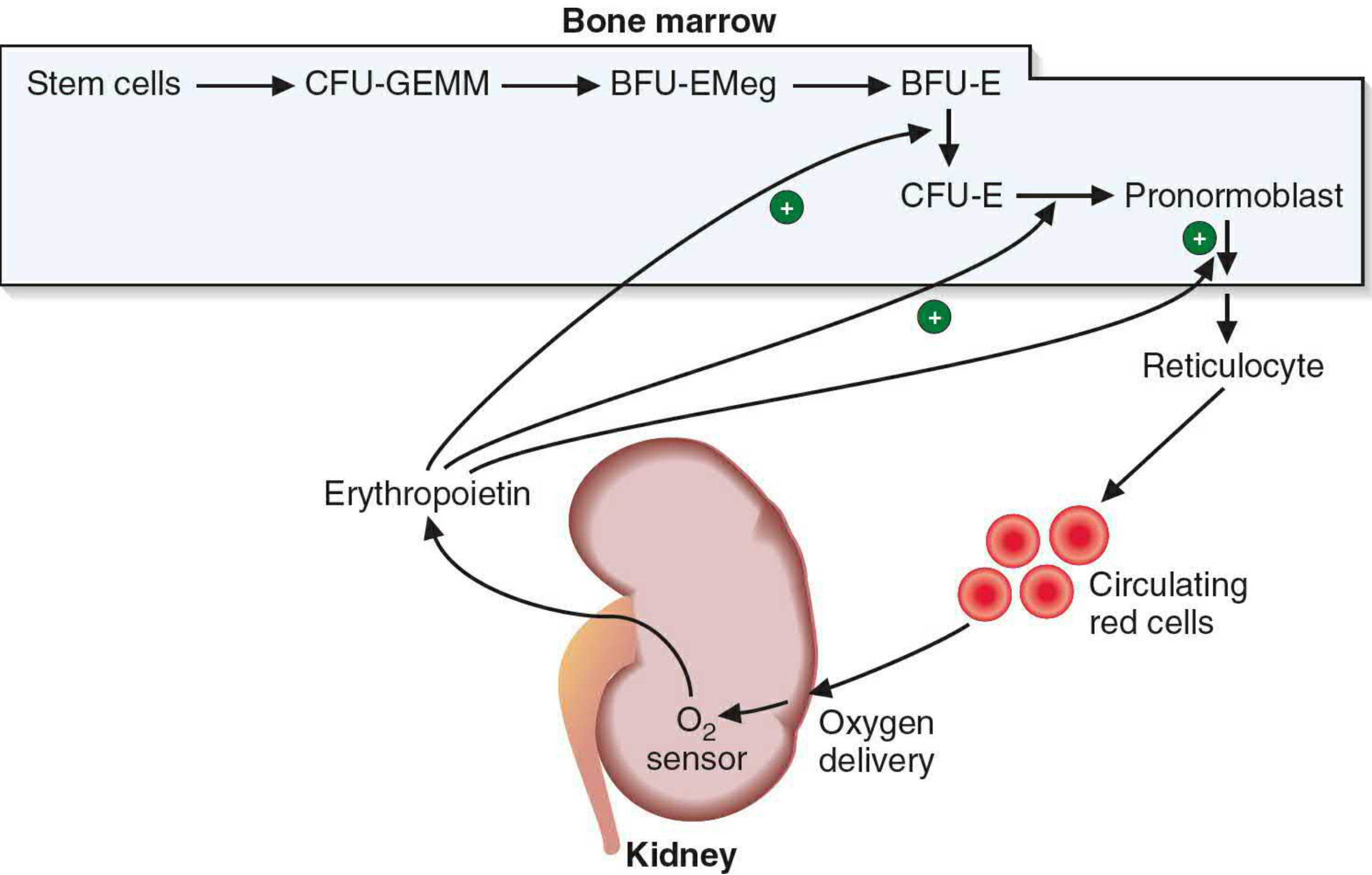
2. Progenitor Hierarchy
The erythroid lineage follows a defined progression from pluripotent stem cell to mature RBC:
| Stage | Description |
|---|---|
| Hematopoietic stem cell (HSC) | Pluripotent, self-renewing |
| CFU-GEMM | Mixed myeloid progenitor (granulocyte, erythroid, monocyte, megakaryocyte) |
| BFU-EMeg / BFU-E | Burst-forming unit-erythroid; earliest cell exclusively committed to erythroid line; named for multiclustered colony formation |
| CFU-E | Colony-forming unit-erythroid; first cell to express EPO-R |
| Pronormoblast / Proerythroblast | First morphologically recognizable RBC precursor |
EPO does not directly stimulate erythroid proliferation - rather, it prevents apoptosis of erythroid progenitors, particularly CFU-E and early basophilic erythroblasts. This key insight (Koury and Bondurant) explains why EPO loss leads to a rapid collapse of erythropoiesis.
3. Morphological Stages of Maturation
Once committed, precursor cells undergo sequential morphological changes in the bone marrow. Mitoses occur through the polychromatophilic stage, then cease:
Proerythroblast (Pronormoblast)
- Largest cell in the lineage (~20 µm)
- Large nucleus with prominent nucleoli
- Basophilic cytoplasm (no hemoglobin yet)
- Golgi apparatus visible as a pale zone
Basophilic Erythroblast
- Smaller than proerythroblast (arises by mitosis)
- Intense cytoplasmic basophilia - ribosomes are massively upregulated for hemoglobin synthesis
- Smaller nucleus, coarser chromatin, no nucleoli
Polychromatophilic Erythroblast
- Hemoglobin begins to accumulate; cytoplasm transitions from blue-gray to mixed blue-pink ("polychromasia")
- Nucleus progressively smaller and more condensed
- Last stage capable of mitosis
Orthochromatophilic Erythroblast (Normoblast)
- Nucleus is extremely condensed ("pyknotic")
- Cytoplasm is predominantly eosinophilic (hemoglobin-rich)
- Slightly larger than a mature RBC
- No longer capable of division
- Nucleus is extruded, producing a reticulocyte
Reticulocyte (Polychromatophilic Erythrocyte)
- Anucleate but retains ribosomes and mRNA - still capable of hemoglobin synthesis
- Slightly blue-tinged on Wright stain (compared to fully mature RBCs)
- Released from bone marrow and circulates for 1-2 days
- Matures in the spleen, where ribosomes and mRNA are lost
Mature Erythrocyte
- Biconcave disc, ~7-8 µm
- No nucleus, no organelles
- Packed with hemoglobin (~300 million molecules/cell)
- Lifespan: ~120 days
It takes approximately one week from a newly formed basophilic erythroblast to a circulating reticulocyte. Bone marrow is not a storage site for erythrocytes - nearly all are released as soon as formed.
4. EPO Receptor Signaling
EPO binds EPO-R (a 55 kDa cytokine receptor superfamily member) expressed on CFU-E through late basophilic erythroblasts (~1000 receptors/cell). The signaling cascade:
- EPO binding → EPO-R homodimerization and conformational change
- Activation of JAK2 (physically associated with EPO-R)
- JAK2 phosphorylates cytoplasmic tyrosines on EPO-R, exposing SH2 binding sites
- Multiple downstream cascades activate: Ras/MAP kinase, JNK/p38, JAK/STAT, PI3K/AKT
- STAT5 phosphorylation → homodimerization → nuclear translocation → activation of EPO-inducible genes (pro-survival)
- Negative feedback via tyrosine phosphatases and CIS/SOCS proteins downregulate the signal
Mutations causing EPO-R truncation (loss of Y429/Y431) impair receptor internalization, prolong signaling, and cause familial polycythemia.
5. Nutritional Requirements
Because the body produces ~10¹² RBCs per day, any nutritional deficiency severely impairs erythropoiesis:
| Nutrient | Role | Deficiency Result |
|---|---|---|
| Iron | Heme synthesis (ferroprotoporphyrin IX) | Microcytic, hypochromic anemia |
| Vitamin B12 | DNA synthesis (cofactor for thymidine) | Megaloblastic anemia |
| Folate | DNA synthesis (one-carbon metabolism) | Megaloblastic anemia |
6. Senescent RBC Destruction
At ~120 days, erythrocytes become senescent. The macrophage system of the spleen, bone marrow, and liver phagocytoses and degrades them:
- Heme + globin dissociate
- Globin is hydrolyzed to amino acids (re-enter metabolic pool)
- Iron is released and stored as hemosiderin/ferritin (spleen) for reuse in Hgb synthesis
- Heme porphyrin ring is degraded to bilirubin, bound to albumin, transported to the liver, conjugated to bilirubin glucuronide, and excreted in bile
7. High-Altitude Adaptation
At high altitude, hypoxia increases renal EPO output within 24-48 hours, driving erythrocytosis. Serum EPO peaks then declines over ~3 weeks as hematocrit rises. Polycythemia augments arterial O₂ content, but a hematocrit >60% becomes counterproductive due to hyperviscosity impairing cardiac output. Interestingly, Tibetan/Sherpa populations carry partial loss-of-function variants in HIF-2α (the transcription factor driving renal EPO gene expression), resulting in lower hematocrits - a genetic adaptation to chronic high-altitude living.
Sources:
- Basic Medical Biochemistry: A Clinical Approach, 6e, p. 1536
- Brenner and Rector's The Kidney, 2-Volume Set, pp. 2465-2467
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology, pp. 746, 774-777
- Murray & Nadel's Textbook of Respiratory Medicine, p. 2427
Physiology question about erythropoiesis
What's your question?
Ask a specific physiology question about erythropoiesis
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.